National Collaborating Centre for Women's and Children's Health
National Collaborating Centre for Women's and Children's Health
National Collaborating Centre for Women's and Children's Health

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Spasticity in children <strong>and</strong> young people with non-progressive brain disorders<br />
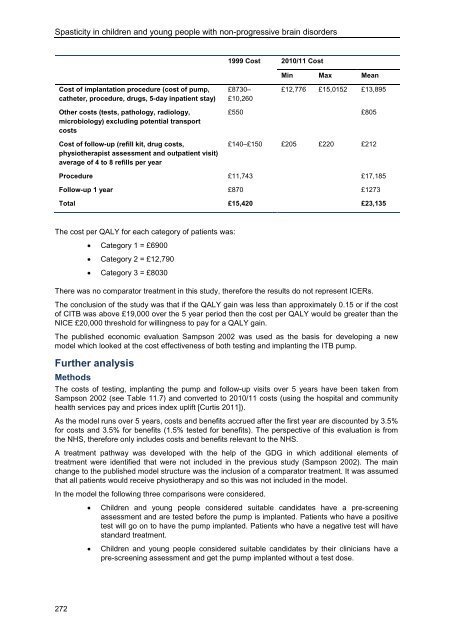
1999 Cost 2010/11 Cost<br />
Min Max Mean<br />
Cost of implantation procedure (cost of pump,<br />
catheter, procedure, drugs, 5-day inpatient stay)<br />
£8730–<br />
£10,260<br />
£12,776 £15,0152 £13,895<br />
Other costs (tests, pathology, radiology,<br />
microbiology) excluding potential transport<br />
costs<br />
Cost of follow-up (refill kit, drug costs,<br />
physiotherapist assessment <strong>and</strong> outpatient visit)<br />
average of 4 to 8 refills per year<br />
£550 £805<br />
£140–£150 £205 £220 £212<br />
Procedure £11,743 £17,185<br />
Follow-up 1 year £870 £1273<br />
Total £15,420 £23,135<br />
The cost per QALY <strong>for</strong> each category of patients was:<br />
• Category 1 = £6900<br />
• Category 2 = £12,790<br />
• Category 3 = £8030<br />
There was no comparator treatment in this study, there<strong>for</strong>e the results do not represent ICERs.<br />
The conclusion of the study was that if the QALY gain was less than approximately 0.15 or if the cost<br />
of CITB was above £19,000 over the 5 year period then the cost per QALY would be greater than the<br />
NICE £20,000 threshold <strong>for</strong> willingness to pay <strong>for</strong> a QALY gain.<br />
The published economic evaluation Sampson 2002 was used as the basis <strong>for</strong> developing a new<br />
model which looked at the cost effectiveness of both testing <strong>and</strong> implanting the ITB pump.<br />
Further analysis<br />
Methods<br />
The costs of testing, implanting the pump <strong>and</strong> follow-up visits over 5 years have been taken from<br />
Sampson 2002 (see Table 11.7) <strong>and</strong> converted to 2010/11 costs (using the hospital <strong>and</strong> community<br />
health services pay <strong>and</strong> prices index uplift [Curtis 2011]).<br />
As the model runs over 5 years, costs <strong>and</strong> benefits accrued after the first year are discounted by 3.5%<br />
<strong>for</strong> costs <strong>and</strong> 3.5% <strong>for</strong> benefits (1.5% tested <strong>for</strong> benefits). The perspective of this evaluation is from<br />
the NHS, there<strong>for</strong>e only includes costs <strong>and</strong> benefits relevant to the NHS.<br />
A treatment pathway was developed with the help of the GDG in which additional elements of<br />
treatment were identified that were not included in the previous study (Sampson 2002). The main<br />
change to the published model structure was the inclusion of a comparator treatment. It was assumed<br />
that all patients would receive physiotherapy <strong>and</strong> so this was not included in the model.<br />
In the model the following three comparisons were considered.<br />
• Children <strong>and</strong> young people considered suitable c<strong>and</strong>idates have a pre-screening<br />
assessment <strong>and</strong> are tested be<strong>for</strong>e the pump is implanted. Patients who have a positive<br />
test will go on to have the pump implanted. Patients who have a negative test will have<br />
st<strong>and</strong>ard treatment.<br />
• Children <strong>and</strong> young people considered suitable c<strong>and</strong>idates by their clinicians have a<br />
pre-screening assessment <strong>and</strong> get the pump implanted without a test dose.<br />
272