

Download a PDF of this issue - Field Exchange - Emergency ...
Download a PDF of this issue - Field Exchange - Emergency ...
Download a PDF of this issue - Field Exchange - Emergency ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Research<br />
isation reports from the relevant field Programme<br />
Managers during 2009 and ACF Country Operational<br />
Strategy Reports (2009 and 2011) from ACF HQ Paris.<br />
Notes were taken from these documents to inform the questions<br />
for the interview guide. This information was also<br />
used to validate the data gathered from the interviews at a<br />
later stage, i.e. a triangulation approach 8 .<br />
3. Using information gathered from steps one and two, the<br />
interview guide with key questions was developed as a tool<br />
for conducting the interviews. These questions needed to<br />
be open ended to ensure accurate, non-biased answers.<br />
Probes and follow up questions were added where necessary,<br />
to ensure the question was fully answered. Seven key<br />
Figure 2: Eight Step Study Design<br />
1. Identify new innovative<br />
tools & methods for<br />
evaluating Programs<br />
qualitatively<br />
The analysis can be<br />
broken down into 4<br />
further stages:<br />
• Inductive Analysis<br />
• Classification<br />
Framework Development<br />
• Descriptive Phase<br />
• Interpretative Phase<br />
7. Develop a<br />
Success Factor Matrix<br />
Local<br />
Context<br />
Community<br />
Involvement<br />
ACF Nutrition<br />
Programme<br />
Design &<br />
Management<br />
Caregiver/<br />
Mother<br />
BNF/<br />
Child<br />
Local<br />
Context<br />
3. Use above<br />
two inputs to<br />
develop an interview<br />
guide<br />
4. Conduct<br />
in-depth interviews<br />
5. Pattern, Theme &<br />
Content Analysis<br />
6. Discuss findings in a workshop<br />
with supervisors<br />
(Patton 2002)<br />
2. Review all relevant<br />
existing documents<br />
from<br />
ACF Myanmar<br />
The interviews were:<br />
• Face-to-face and<br />
through Skype with a<br />
purposeful sample <strong>of</strong><br />
key multi-disciplinary<br />
people, who were<br />
directly involved with<br />
the programme.<br />
8. Develop a one Page Feasibility<br />
Grid for replication globally<br />
Figure 3: Placing the 14 success factors at the relevant level<br />
• Ideal Timing with absence <strong>of</strong> natural disaster & ‘normal’<br />
HH security<br />
• ACF Well Known with Good Reputation in the region<br />
• Community Sensitisation, Mobilisation & Support<br />
• Early Referrals<br />
• Adoption <strong>of</strong> WHO Standards<br />
• Time for Careful Planning<br />
• Staff Training & Capacity giving High Quality <strong>of</strong> Care<br />
• Simple, Organised Processes<br />
• Consistent, Experienced & Strong Leadership<br />
• Integration <strong>of</strong> Care Practices giving psycho-social support<br />
• Involving the Mother and Home Feeding in the<br />
Recovery Process<br />
• Close Monitoring & Use <strong>of</strong> BNR Methodology<br />
• The Product Quantity was more likely to be eaten by the<br />
child<br />
• 4 Month Follow-Up with Dry Rations<br />
BNF: Beneficiary<br />
These success factors were then placed at the relevant levels in terms <strong>of</strong> local context,<br />
community involvement, the Nutrition Programme, the mother/caregiver and the BNF/child.<br />
Figure 4: Placing the eight areas for improvement at the relevant<br />
level<br />
• Work to minimise regional constraints further and<br />
more advocacy to help the discriminated population<br />
• Develop a strategy to improve relationship with<br />
government at all levels<br />
• Further integration with other ACF programmes as<br />
well as co-ordination with other INGOs in the area and<br />
focus on a more global, preventative longer term<br />
approach<br />
areas were identified as areas to explore<br />
in the interview. Questions were developed<br />
for each and were incorporated into<br />
the interview guide. These areas were:<br />
• General introduction and context <strong>of</strong><br />
Myanmar.<br />
• Opinions and descriptions <strong>of</strong> the<br />
Nutrition Programme<br />
• Management Style<br />
• Training and Capacity Building<br />
• Community Involvement<br />
• Other ACF programmes<br />
• Other international non-governmental<br />
organisations (INGOs) working in<br />
the area.<br />
4. In-depth interviews were conducted,<br />
lasting up to an hour, with key informants<br />
across a range <strong>of</strong> pr<strong>of</strong>essional<br />
disciplines to obtain an accurate and<br />
balanced perspective <strong>of</strong> the programme,<br />
processes and relationships. Where possible,<br />
the interviews were held face-to-face<br />
- <strong>this</strong> was not always possible due to<br />
logistics and therefore several were done<br />
through Skype. Key people interviewed<br />
included the Nutrition Advisor in ACF<br />
Paris HQ, regional and local Nutrition<br />
Managers, the local Human Resources<br />
Manager for the programme, the Head <strong>of</strong><br />
Base (logistics and administration) and<br />
local Programme Managers in other ACF<br />
programmes.<br />
5. A Pattern, Theme and Content<br />
Analysis method was used to analyse the<br />
data collected. The analysis consisted <strong>of</strong><br />
identifying core consistencies and meanings<br />
from the material and interviews.<br />
Patterns and themes were searched for<br />
across all information provided (both<br />
interview transcripts and notes from the<br />
relevant documents) and re-occurring<br />
words and texts were identified, including<br />
their frequency and the context in<br />
which they were used 9 . Data were<br />
presented in the form <strong>of</strong> quotations with<br />
sufficient context to ensure that they<br />
could be interpreted.<br />
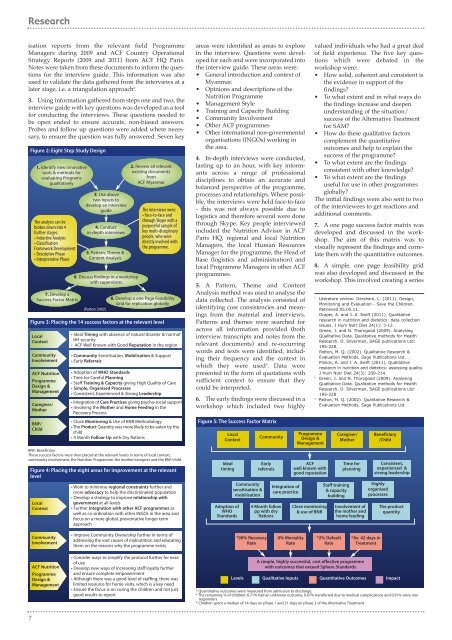
6. The early findings were discussed in a<br />
workshop which included two highly<br />
Figure 5: The Success Factor Matrix<br />
Local<br />
Context<br />
Ideal<br />
timing<br />
Adoption <strong>of</strong><br />
WHO<br />
Standards<br />
Community<br />
sensitisation &<br />
mobilisation<br />
Community<br />
Early<br />
referrals<br />
4 Month follow<br />
pp with dry<br />
Rations<br />
Integration <strong>of</strong><br />
care practice<br />
Programme<br />
Design &<br />
Management<br />
ACF<br />
well known with<br />
good reputation<br />
Close monitoring<br />
& use <strong>of</strong> BNR<br />
valued individuals who had a great deal<br />
<strong>of</strong> field experience. The five key questions<br />
which were debated in the<br />
workshop were:<br />
• How solid, coherent and consistent is<br />
the evidence in support <strong>of</strong> the<br />
findings?<br />
• To what extent and in what ways do<br />
the findings increase and deepen<br />
understanding <strong>of</strong> the situation/<br />
success <strong>of</strong> the Alternative Treatment<br />
for SAM?<br />
• How do these qualitative factors<br />
complement the quantitative<br />
outcomes and help to explain the<br />
success <strong>of</strong> the programme?<br />
• To what extent are the findings<br />
consistent with other knowledge?<br />
• To what extent are the findings<br />
useful for use in other programmes<br />
globally?<br />
The initial findings were also sent to two<br />
<strong>of</strong> the interviewees to get reactions and<br />
additional comments.<br />
7. A one page success factor matrix was<br />
developed and discussed in the workshop.<br />
The aim <strong>of</strong> <strong>this</strong> matrix was to<br />
visually represent the findings and correlate<br />
them with the quantitative outcomes.<br />
8. A simple, one page feasibility grid<br />
was also developed and discussed in the<br />
workshop. This involved creating a series<br />
7<br />
Literature review: Dersham, L. (2011). Design,<br />
Monitoring and Evaluation - Save the Children.<br />
Retrieved 05.05.11.<br />
Draper, A. and J. A. Swift (2011). Qualitative<br />
research in nutrition and dietetics: data collection<br />
<strong>issue</strong>s. J Hum Nutr Diet 24(1): 3-12.<br />
Green, J. and N. Thorogood (2009). Analysing<br />
Qualitative Data. Qualitative methods for Health<br />
Research. D. Silverman, SAGE publications Ltd:<br />
195-228.<br />
Patton, M. Q. (2002). Qualitative Research &<br />
Evaluation Methods, Sage Publications Ltd. .<br />
Pilnick, A. and J. A. Swift (2011). Qualitative<br />
research in nutrition and dietetics: assessing quality.<br />
J Hum Nutr Diet 24(3): 209-214.<br />
8<br />
Green, J. and N. Thorogood (2009). Analysing<br />
Qualitative Data. Qualitative methods for Health<br />
Research. D. Silverman, SAGE publications Ltd:<br />
195-228<br />
9<br />
Patton, M. Q. (2002). Qualitative Research &<br />
Evaluation Methods, Sage Publications Ltd.<br />
Caregiver/<br />
Mother<br />
Staff training<br />
& capacity<br />
building<br />
Time for<br />
planning<br />
Involvement <strong>of</strong><br />
the mother and<br />
home feeding<br />
Beneficiary<br />
/Child<br />
Consistent,<br />
experienced &<br />
strong leadership<br />
Highly<br />
organised<br />
processes<br />
The product<br />
quantity<br />
Community<br />
Involvement<br />
• Improve Community Ownership further in terms <strong>of</strong><br />
addressing the root causes <strong>of</strong> malnutrition and educating<br />
them on the reasons why the programme exists.<br />
*90% Recovery<br />
Rate<br />
0% Mortality<br />
Rate<br />
*2% Default<br />
Rate<br />
*Av. 42 days in<br />
Treatment<br />
ACF Nutrition<br />
Programme<br />
Design &<br />
Management<br />
• Consider ways to simplify the protocol further for ease<br />
<strong>of</strong> use<br />
• Develop new ways <strong>of</strong> increasing staff loyalty further<br />
and ensure complete empowerment<br />
• Although there was a good level <strong>of</strong> staffing, there was<br />
limited resource for home visits, which is a key need<br />
• Ensure the focus is on curing the children and not just<br />
good results to report<br />
Levels<br />
A simple, highly successful, cost effective programme<br />
with outcomes that exceed Sphere Standards<br />
Qualitative Inputs<br />
Quantitative Outcomes<br />
Impact<br />
* Quantitative outcomes were measured from admission to discharge.<br />
* The remaining % <strong>of</strong> children: 6.71% had an unknown outcome, 0.07% transferred due to medical complications and 0.91% were non<br />
responders<br />
* Children spent a median <strong>of</strong> 14 days on phase 1 and 21 days on phase 2 <strong>of</strong> the Alternative Treatment<br />
7













