BRF Hospital Holdings - LSUHSC Medical Communications Home ...
BRF Hospital Holdings - LSUHSC Medical Communications Home ...
BRF Hospital Holdings - LSUHSC Medical Communications Home ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>BRF</strong> <strong>Hospital</strong> <strong>Holdings</strong><br />
Benefit Guide 2013 - 2014
Welcome to <strong>BRF</strong> <strong>Hospital</strong> <strong>Holdings</strong><br />
Welcome to <strong>BRF</strong> <strong>Hospital</strong> <strong>Holdings</strong><br />
In recognition of the diverse needs of its employees, <strong>BRF</strong> <strong>Hospital</strong> <strong>Holdings</strong> offers a variety of employee benefit programs,<br />
allowing you to select a level of protection and security best suited to your personal situation. This booklet provides an<br />
overview of the following Benefit Plans:<br />
Paid Time Off<br />
Retirement<br />
<strong>Medical</strong><br />
Dental<br />
Vision<br />
Flexible Spending Accounts (Health Care and Dependent Care)<br />
Basic Life & Accidental Death & Dismemberment<br />
Voluntary Life & Accidental Death & Dismemberment<br />
Short and Long Term Disability<br />
Critical Illness<br />
Employee Assistance Program<br />
Travel Assistance<br />
More detailed plan information, access to carrier websites, and claim forms are available on the online enrollment website<br />
www.enrollme.biz.<br />
Each Plan described in this booklet is governed by a legal document called the Plan Document which can be found on the<br />
online enrollment website, www.enrollme.biz. This booklet is not intended to be all-inclusive or supersede the individual<br />
Plan Documents, rules or policies. Therefore, in the event of a discrepancy between this booklet and the Plan Documents,<br />
the Plan Documents will be followed.<br />
It is important for you to have a good understanding of each Benefit Plan that is offered. Please review this booklet<br />
carefully and if you have any questions, please contact your local Human Resource/Benefits Department or HUB<br />
International at 318-629-8769 or 877-309-2224.<br />
<strong>BRF</strong> <strong>Hospital</strong> <strong>Holdings</strong><br />
<strong>BRF</strong> <strong>Hospital</strong> <strong>Holdings</strong><br />
2013 - 2014 Benefits
Table of Contents and Contact Information<br />
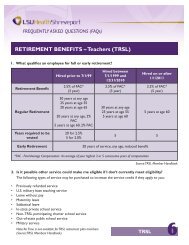
Eligibility<br />
Cost of coverage<br />
See page:<br />
Benefit<br />
Full Time<br />
60 hours/<br />
bi-weekly<br />
pay period<br />
Part Time<br />
40 hours/<br />
bi-weekly<br />
pay period<br />
Family<br />
Paid Time Off Shared 2<br />
Retirement Shared 2<br />
Basic Life & AD&D Employer Paid 3<br />
<strong>Medical</strong> & Prescription Drugs Shared 3<br />
Dental Employee paid 5<br />
Vision Employee paid 6<br />
Voluntary Life & AD&D Employee paid 7<br />
Short Term Disability Employee paid 8<br />
Long Term Disability Employee paid 9<br />
Critical Illness Employee paid 10<br />
Flexible Spending Accounts Employee paid 11<br />
Online Enrollment 12<br />
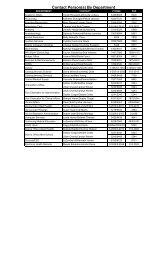
Contact Information<br />
Provider Phone Number Website<br />
HUB Benefits Helpline<br />
318-629-8769<br />
877-309-2224<br />
Online Enrollment: www.enrollme.biz<br />
Email: <strong>BRF</strong>HH@hubinternational.com<br />
BlueCross BlueShield<br />
<strong>Medical</strong><br />
AlwaysCare<br />
Dental<br />
Vision<br />
Boon-Chapman<br />
Health Care and Dependent Care<br />
Flexible Spending Accounts<br />
Mutual of Omaha<br />
Basic Life & AD&D<br />
Voluntary Life & AD&D<br />
<br />
<br />
Short Term Disability<br />
Long Term Disability<br />
Employee Assistance Program (EAP)<br />
Travel Assistance<br />
HM Life Insurance Company<br />
Critical Illness<br />
Great-West Financial<br />
Retirement Plan<br />
800-830-1501 www.MyHealthToolKitLA.com<br />
888-729-5433 x 2013 www.alwaysassist.com<br />
800-252-9653 - Option 6 www.boonchapman.com<br />
Claims:<br />
Life: 800-775-8805<br />
Disability: 800-877-5176<br />
Portability / Conversion:<br />
877-466-8367<br />
800-316-2796<br />
800-856-9947<br />
Customer Service/Eligibility:<br />
800-323-0774<br />
Claims: 888-529-8983<br />
www.mutualofomaha.com/<br />
customer-service<br />
www.mutualofomaha.com/EAP<br />
www.hmig.com<br />
800-338-4015 www.gwrs.com<br />
<strong>BRF</strong> <strong>Hospital</strong> <strong>Holdings</strong><br />
2013 - 2014 Benefits
Benefits and Eligibility<br />
Eligibility<br />
This booklet provides a summary of the benefits you are<br />
eligible to select as a benefits eligible employee of <strong>BRF</strong><br />
<strong>Hospital</strong> <strong>Holdings</strong>. Benefits eligible employees are employees<br />
working at least 60 hours per bi-weekly pay period who have<br />
satisfied the company defined waiting periods. This booklet<br />
contains information that is important for you to know in<br />
order to select the benefits that are best for you and your<br />
family. All benefits and an individual’s right to them are<br />
subject to federal regulations, <strong>BRF</strong> <strong>Hospital</strong> Holding’s policies<br />
and procedures, the individual plan documents, and our<br />
receipt of your executed and recorded election.<br />
Effective Date of Coverage<br />
Benefits are effective the first day of the month following<br />
your first full calendar month of employment. For Example:<br />
Date of hire = August 20th, Effective Date = October 1st<br />
Dependent Coverage<br />
An eligible dependent is defined as:<br />
Your lawful spouse<br />
You or your spouse’s child who is under age 26, including<br />
a natural child, step child, a legally adopted child, a child<br />
placed for adoption, or a child for whom you or your<br />
spouse are the legal guardian; or<br />
An unmarried child age 26 or over who is or becomes<br />
disabled and dependent upon you<br />
Dependent Certification Required for <strong>Medical</strong><br />
Insurance:<br />
To deter fraud, abuse, and assure the proper use of<br />
company funds and Plan Members’ premium dollars, <strong>BRF</strong><br />
<strong>Hospital</strong> <strong>Holdings</strong> joins the majority of public and private<br />
health benefit programs by requiring proof that the<br />
dependents covered are your legal dependents. All Active<br />
employees are required to provide written proof that each<br />
dependent to be covered under Your <strong>Medical</strong> Plan is your<br />
actual legal dependent. This documentation is necessary<br />
ONLY if you are enrolling in <strong>Medical</strong> Insurance. Failure to<br />
provide this documentation within 30 days will result in the<br />
inability to enroll your dependents under your <strong>Medical</strong> Plan.<br />
If you have any questions about the dependent<br />
verification policy, contact your local HR/Benefits<br />
Department or HUB International.<br />
Written Verification Required for Dependents:<br />
If you are adding a dependent to your <strong>Medical</strong> Plan you<br />
MUST submit dependent eligibility documentation.<br />
Spouse:<br />
To document a Legal Spousal Relationship, submit a copy of:<br />
Marriage License, and Page 1 of your Federal Income Tax<br />
Return if your filing status is “joint” – or Marriage License,<br />
and if your filing status is “Married Filing Separate” also<br />
submit Page 1 of both Federal Income Tax Returns; and<br />
If you have not been married long enough to file a “joint”<br />
Federal Income Tax Return, please only submit a<br />
photocopy of your marriage license.<br />
Children up to age 26 and disabled children:<br />
Natural Child<br />
A copy of the Certified Birth Certificate showing the<br />
subscriber as the Parent;<br />
Step Child<br />
A copy of the Certified Birth Certificate showing the name<br />
of the natural Parent, and proof that the natural parent<br />
and the subscriber are married (e.g., Marriage License);<br />
Adopted Child<br />
Court documentation verifying completion of Adoption<br />
Proceedings; or<br />
A letter of placement from an Adoption Agency, an<br />
Attorney or the State Department of Social Services,<br />
verifying that adoption is in process;<br />
Foster Child<br />
A Court Order or other legal document placing the Child<br />
with the subscriber, who is a licensed foster parent;<br />
Other Children<br />
For all other children for whom a subscriber has legal<br />
custody, a Court Order or other legal document granting<br />
custody to the subscriber. Documentation must verify that<br />
the subscriber has guardianship responsibility for child, not<br />
merely financial responsibility.<br />
Incapacitated Child<br />
Proof that incapacitation was established at time of<br />
enrollment, and for the appropriate child type<br />
documentation as outlined above based on relationship.<br />
In addition, you should submit a copy of Page 1 of your<br />
Federal Income Tax Return to demonstrate that the child<br />
is principally dependent on you/the subscriber for support<br />
and maintenance. If your incapacitated child is employed,<br />
you may be asked to also submit a copy of Page 1 of his/<br />
her Federal Income Tax Return.<br />
1 <strong>BRF</strong> <strong>Hospital</strong> <strong>Holdings</strong> 2013 - 2014 Benefits
Benefits and Eligibility<br />
Qualifying Events<br />
Once you have enrolled in benefits, you cannot change your<br />
elections unless you have a “qualifying event”, and you must<br />
submit a change form to your HR/Benefits Department within<br />
30 days of the event. You can obtain a change form from<br />
your HR/Benefits Department or from the enrollment<br />
website, www.enrollme.biz. For newly eligible dependents,<br />
coverage will be effective as of the date of the event, when a<br />
change form is submitted within 30 days.<br />
IMPORTANT NOTE: Newborns are not automatically added<br />
to your policy. You must complete a change form in order to<br />
effectively add them to your coverage.<br />
Change in Family Status affecting covered persons<br />
such as:<br />
Marriage or divorce<br />
Death of a spouse or dependent child<br />
Birth or adoption of a child<br />
Loss of other coverage<br />
Loss of dependent status (if a child reaches the age limit<br />
under the plan or is no longer eligible as a dependent)<br />
Change in your employment status affecting your<br />
benefits such as:<br />
Beginning or returning from a leave of absence<br />
Changing to/from part time<br />
Change in your spouse’s employment status causing<br />
a gain or loss of health coverage for you, your spouse<br />
or your eligible dependents:<br />
Beginning or ending employment<br />
Increasing or decreasing hours<br />
Changes associated with a spouse’s open enrollment<br />
period including changes in the type and cost of<br />
coverage<br />
Gain or loss of eligibility for Medicare/Medicaid for<br />
you, your spouse, or your eligible dependents (Note -<br />
Changes must be made within 60 days)<br />
Paid Time Off (PTO)<br />
Termination of Benefits<br />
Your benefits will terminate on your termination<br />
date.<br />
Continuation of <strong>Medical</strong> Coverage<br />
At Termination of Employment or Ineligibility of a<br />
Dependent:<br />
COBRA (Consolidated Omnibus Budget Reconciliation Act) is<br />
a federal law, which requires that group plans offer covered<br />
employees and dependents the opportunity to continue<br />
health insurance coverage when coverage would normally<br />
end for certain specified reasons. The following provisions<br />
outline the requirements for continued coverage in<br />
accordance with the law:<br />
<br />
<br />
You and your covered dependents may continue<br />
coverage for up to 18 months if coverage ends because<br />
of either a permanent reduction in the number of hours<br />
worked or termination of employment for any reason<br />
other than gross misconduct. You and/or your covered<br />
dependent must apply within 60 days of the date<br />
coverage ends or the date you are notified of your<br />
continuation rights, whichever is later<br />
Your dependents may continue their coverage under the<br />
group plan for up to 36 months if their coverage ends for<br />
any of the following reasons<br />
Divorce from the employee<br />
<br />
<br />
Death of the employee, or<br />
Dependent child reaches the maximum age or<br />
otherwise ceases to qualify as a dependent under<br />
the plan<br />
Coverage would be effective the day after the event.<br />
Paid time off will include between 15 and 25 days based on length of service, up to 10 days of Extended Sick Leave, and 9<br />
paid holidays for all eligible employees (New Year’s Day, Memorial Day, Good Friday or Easter Sunday, 4 th of July, Labor Day,<br />
Thanksgiving Day, Christmas Eve, Christmas Day, and 1 Floating Holiday). Eligible employees are those that work at least 40<br />
hours per bi-weekly pay period. Please refer to the employee manual for more information.<br />
Retirement Plan - Great-West Financial<br />
The Retirement Plan encourages personal savings. <strong>BRF</strong> <strong>Hospital</strong> <strong>Holdings</strong> will contribute 3% of your pay into a 401k<br />
retirement plan for all eligible employees. An eligible employee is one who works at least 40 hours per bi-weekly pay period.<br />
In addition, employees can receive a matched benefit of 50% if they choose to contribute pre tax dollars from their check.<br />
Employees can contribute up to $17,500 annually ($23,000 if over age 50). The maximum amount the hospital will match will<br />
not exceed 3% of employees compensation. You are eligible to participate after 1 year of service, however if you are<br />
employed on October 1, 2013 you are immediately eligible to participate. You can enroll on the first day of each quarter<br />
(January 1 st , April 1 st , July 1 st and October 1 st ). Gradual vesting applies to the matching contributions. Please refer to the<br />
Summary Plan Description and Enrollment Materials for more information.<br />
<strong>BRF</strong> <strong>Hospital</strong> <strong>Holdings</strong><br />
2013 - 2014 Benefits<br />
2
Basic Life & AD&D / EAP / Travel Assistance / <strong>Medical</strong><br />
Employer Paid Basic Life & AD&D<br />
As an employee of <strong>BRF</strong> <strong>Hospital</strong> <strong>Holdings</strong> you are<br />
provided with a Basic Life & Accidental Death &<br />
Dismemberment (AD&D) policy in the amount of<br />
$25,000 at no cost to you. Mutual of Omaha is the carrier<br />
for this company paid benefit. It provides protection for you in<br />
the event of a disabling injury or death. In addition to this<br />
basic coverage, you have the option to purchase additional life<br />
insurance for yourself and your family members. Your amount<br />
of Basic Life & AD&D insurance will be reduced by 50% at age<br />
70. If you leave the company, you may convert this Basic Life<br />
policy into an individual, whole life policy.<br />
Employee Assistance Program (EAP)<br />
Mutual of Omaha sponsors your Employer Paid Employee<br />
Assistance Program (EAP). This benefit provides free<br />
confidential consultation and resource services to you and<br />
your dependents. Master’s level professionals can provide<br />
assistance for a variety of personal and professional matters<br />
such as: emotional well being, family and relationships, legal<br />
and financial, healthy life styles, and work and life transitions.<br />
Your EAP includes a robust network of licensed and/or<br />
certified mental health professionals. EAP Benefits include:<br />
Unlimited telephonic access to EAP Professionals 24/7<br />
3 face-to-face sessions (per calendar year) with a counselor,<br />
legal, or financial consultant<br />
Legal, financial, mental health, and substance abuse<br />
assistance<br />
Connecting employees with resources for:<br />
Dependent Care Assistance & Referral Services<br />
Elder Care Assistance & Referral Services<br />
Travel Assistance<br />
Travel Assistance through Mutual of Omaha provides access to<br />
support professionals who can help you, your spouse, and<br />
dependents find quality local medical care or provide other<br />
emergency assistance functions in foreign locations. Services<br />
include: Translation/interpreter services, locating legal<br />
services, and assistance with lost, stolen, or delayed baggage.<br />
Summary of Benefits & Coverage (SBC)<br />
In accordance with Patient Protection and Affordable<br />
Care Act (PPACA), BlueCross BlueShield has created a<br />
Summary of Benefits & Coverage (SBC), which<br />
provides additional information about your medical<br />
plan. You can find the SBC online at<br />
www.enrollme.biz, or you may request a copy by<br />
contacting your HR representative.<br />
Health Insurance Options<br />
<strong>BRF</strong> <strong>Hospital</strong> <strong>Holdings</strong> is committed to providing a<br />
comprehensive medical benefits program that will serve to<br />
protect both your physical health as well as your financial well<br />
being. You are offered two plan options through BlueCross<br />
BlueShield (BCBS):<br />
Plan 1 - Preferred Provider Organization (PPO)<br />
The PPO plan provides a network of Louisiana providers.<br />
There are no referrals required to see a specialist. As an<br />
employee of <strong>BRF</strong> <strong>Hospital</strong> <strong>Holdings</strong>, you are encouraged to<br />
utilize <strong>BRF</strong> <strong>Hospital</strong> Holding’s health care providers and will<br />
receive lower out-of-pocket amounts by doing so. You may<br />
also choose to use BCBS’s In-Network and Out-of-Network<br />
providers, however, you will be subject to a higher copay and<br />
deductible for services rendered.<br />
Plan 2 - High Deductible Health Plan (HDHP)<br />
This plan starts once you satisfy your deductible. You must<br />
pay the deductible, $5,500 (individual), out-of-pocket before<br />
your plan begins covering your care. HDHPs will cover<br />
preventive services before you meet your deductible and<br />
without having to pay a copay or coinsurance. Keep in mind<br />
that this applies to services provided by In-Network providers.<br />
Case Management<br />
Case management is a special service of BCBS and ensures<br />
your care is appropriate. The program assesses, plans, assists,<br />
and backs options and services to meet an individual’s health<br />
needs.<br />
<strong>BRF</strong> <strong>Hospital</strong> <strong>Holdings</strong> will be assigned a Specific Case<br />
Manager and all employees on the <strong>Medical</strong> Plans MUST<br />
participate to achieve the most efficient and effective use of<br />
medical resources.<br />
Waive <strong>Medical</strong> Insurance<br />
Note: If you elect not to participate in <strong>BRF</strong> <strong>Hospital</strong><br />
<strong>Holdings</strong> medical plans, you will need to go online and<br />
enter your electronic signature ‘pin’ indicating you are<br />
waiving health coverage. You will be prompted for<br />
your pin on the Confirmation Page. If the reason for your<br />
waiver of this coverage on you and your dependents<br />
(including your spouse) is because of other health coverage,<br />
you may be able to enroll yourself or your dependents in this<br />
plan at a later date if such other coverage ends. You must<br />
request enrollment within thirty (30) days after your other<br />
coverage ends.<br />
3<br />
<strong>BRF</strong> <strong>Hospital</strong> <strong>Holdings</strong><br />
2013 - 2014 Benefits
<strong>Medical</strong> - BlueCross BlueShield<br />
Feature<br />
Annual Deductible 1<br />
(Individual/Family 2 )<br />
<strong>BRF</strong>HH Provider<br />
PPO<br />
BCBS<br />
HDHP<br />
BCBS - Bronze<br />
In-Network Out-of-Network In-Network Out-of-Network<br />
$0 $500 / $1,500 $2,500 / $7,500 $5,500 / $16,500 $11,000 / $33,000<br />
Coinsurance Percentage 100% 85% 40% 80% 40%<br />
Annual Out-of-Pocket Maximum 1<br />
(Individual/Family 2 )<br />
$1,000 / $3,000 $4,000 / $12,000<br />
Unlimited /<br />
Unlimited<br />
$6,250 / $18,750<br />
(Inc ded)<br />
Unlimited / Unlimited<br />
Preventive Care 100% 100% 40% after ded 100% 40% after ded<br />
Office Copays / Coinsurance<br />
Primary Care Physician<br />
Specialist<br />
High Tech Imaging (MRI, CAT<br />
Scan, PET)<br />
Office Diagnostic Lab & X-Ray<br />
$10<br />
$20<br />
$20<br />
$40<br />
40% after ded<br />
40% after ded<br />
80% after ded<br />
80% after ded<br />
40% after ded<br />
40% after ded<br />
$25 $200 40% after ded 80% after ded 40% after ded<br />
Included in Office<br />
Visit Copay<br />
Included in Office<br />
Visit Copay<br />
Outpatient Diagnostic Lab & X-Ray 100% 85% 40% after ded<br />
40% after ded 80% after ded 40% after ded<br />
Urgent Care N/A $75 per visit 40% after ded 80% after ded 40% after ded<br />
<strong>Hospital</strong> Services<br />
Inpatient <strong>Hospital</strong> Service<br />
(requires preauthorization)<br />
$250 per admit $600 per admit<br />
40% after $2,500<br />
Copay + ded<br />
80% after ded 40% after ded<br />
Outpatient <strong>Hospital</strong> Services $100 per visit $250 per visit 40% after ded 80% after ded 40% after ded<br />
Emergency Room<br />
(True Emergency/Non-Emergency)<br />
$50 / $100<br />
per visit<br />
$150 / $250<br />
per visit<br />
80% after ded 40% after ded<br />
Rehab Services $10 $30 40% after ded 80% after ded 40% after ded<br />
<strong>Home</strong> Health - 100 visits per year<br />
(requires preauthorization)<br />
Mental Health<br />
Inpatient Office Visits<br />
N/A $40 40% after ded 80% after ded 40% after ded<br />
$50 per day up to<br />
$250 per admit<br />
$100 per day up to<br />
$600 per admit<br />
40% after ded 80% after ded 40% after ded<br />
Outpatient Office Visits $10 $20 40% after ded 80% after ded 40% after ded<br />
Pharmacy - Caremark<br />
RX Deductible 1<br />
$150 (Brand Only)<br />
Generic $10 (No deductible) 80% after ded 40% after ded<br />
Brand<br />
$30 Preferred / $60 Non-preferred / $120 Specialty<br />
after deductible<br />
80% after ded 40% after ded<br />
1<br />
Deductible and Out-of-Pocket Maximum - Based on Calendar Year. For the remainder of 2013 you will only be responsible for 25% of the amounts shown above.<br />
2<br />
Family Deductible and Out-of-Pocket Maximum - No one covered member is required to pay more than the Individual amount<br />
<strong>BRF</strong> <strong>Hospital</strong> Holding’s Monthly Contribution to your <strong>Medical</strong> Plan<br />
<strong>Medical</strong> Employee Only Employee & Spouse Employee & Children<br />
(up to age 26)<br />
Employee & Family<br />
PPO $452.46 $606.55 $620.94 $914.48<br />
HDHP $336.72 $422.08 $444.66 $660.14<br />
Employee Bi-Weekly <strong>Medical</strong> Deduction<br />
<strong>Medical</strong> Employee Only Employee & Spouse Employee & Children<br />
(up to age 26)<br />
Employee & Family<br />
PPO $46.15 $196.15 $138.46 $276.92<br />
HDHP $23.08 $138.46 $92.31 $184.62<br />
<strong>BRF</strong> <strong>Hospital</strong> <strong>Holdings</strong><br />
2013 - 2014 Benefits<br />
4
Dental - AlwaysCare<br />
Basic Plan Enhanced Plan<br />
Benefit Year<br />
Maximum<br />
$1,500 per calendar year for Type 1, 2, 3 $2,000 per calendar year for Type 1,2, 3<br />
Plan Year<br />
Deductible<br />
No deductible for Preventive Services<br />
One time $100 Lifetime applies to Basic and Major Services.<br />
Deductible amount applies separately to each covered person<br />
No deductible<br />
Carryover Benefit<br />
Members who take care of their teeth, but use only part of their annual maximum benefit during a benefit period are rewarded with<br />
extra benefits in future years. If an insured submits qualifying claims for covered expenses during a benefit year and, in that benefit<br />
year, receives benefits that are less than their group’s Threshold Limit, the insured will be credited a Carryover Benefit. Carryover<br />
Benefits will be accrued and stored in the Insured’s Carryover Account to be used in the next benefit year. If an insured reaches his<br />
or her Certificate Year Maximum Benefit, a benefit from the Insured’s Carryover Account will be paid up to the amount stored in the<br />
Insured’s Carryover account. The accrued Carryover Benefits stored in the Carryover Account may not be greater than the<br />
Carryover Account Limit.<br />
Coinsurance<br />
Type 1<br />
Type 2<br />
Type 3<br />
Type 4<br />
Type 1 /<br />
Preventive<br />
Services<br />
Type 2 / Basic<br />
Services<br />
Type 3 / Major<br />
Services<br />
Type 4 /<br />
Orthodontics<br />
Carryover Benefit $350, Threshold Limit $700, Carryover Account<br />
Limit $1,250<br />
In-Network and Out-of-Network<br />
100% of usual and customary fees<br />
100% of scheduled fees<br />
100% of scheduled fees<br />
N/A<br />
Waiting Period: None<br />
· Routine exams (2 per 12 mos.)<br />
· Prophylaxis (2 per 12 mos.)<br />
· Bitewing x-rays (max 4 films; 1 per 12 mos.)<br />
· Full mouth x-ray (1 per 24 mos.)<br />
· Space maintainers to age 16 (1 per 24 mos.)<br />
· Fluoride to age 16 (1 per 12 mos.)<br />
· Sealants to age 16 (permanent molars, 1 per 36 mos.)<br />
· Adjunctive pre-diagnostic oral cancer screening (max 1 per 12<br />
mo for age 40+)<br />
Waiting Period: None<br />
· Emergency Pain (1 per 12 mos.)<br />
· Fillings<br />
· Anesthesia (subject to review, covered with complex oral<br />
surgery)<br />
· Simple extractions<br />
· Non-Surgical Periodontics<br />
· Oral surgery (surgical extractions & impactions)<br />
· Crown, denture, bridge repair<br />
· Full mouth x-ray (1 per 24 mos.)<br />
Waiting Period: None<br />
· Simple Periodontics<br />
· Endodontics (root canals)<br />
· Surgical Periodontics (gum treatments)<br />
· Inlays and Onlays<br />
· Crowns, Bridges, Dentures, and Endosteal Implants<br />
N/A<br />
Carryover Benefit $400, Threshold Limit $800, Carryover<br />
Account Limit $1,500<br />
In-Network - Negotiated Discount Fees (no balance billing) /<br />
Out-of-Network - usual and customary<br />
100%<br />
80%<br />
50%<br />
50%<br />
Waiting Period: None<br />
· Routine exams (2 per 12 mos.)<br />
· Prophylaxis (2 per 12 mos.)<br />
· Bitewing x-rays (max 4 films; 1 per 12 mos.)<br />
· Full mouth x-ray (1 per 24 mos.)<br />
· Emergency Pain (1 per12 mos.)<br />
· Space maintainers to age 16 (1 per 24 mos.)<br />
· Fluoride to age 16 (1 per 12 mos.)<br />
· Sealants to age 16 (permanent molars, 1 per 36 mos.)<br />
· Adjunctive pre-diagnostic oral cancer screening (max 1 per 12<br />
mo for age 40+)<br />
Waiting Period: None<br />
· Fillings<br />
· Anesthesia (subject to review, covered with complex oral<br />
surgery)<br />
· Simple extractions<br />
· Non-Surgical Periodontics<br />
· Oral Surgery (surgical extractions & impactions)<br />
· Endodontics (root canals)<br />
· Crown, denture, bridge repairs<br />
Waiting Period: None<br />
· Inlays and Onlays<br />
· Crowns, Bridges, Dentures, and Endosteal Implants<br />
· Surgical Periodontics (gum treatments)<br />
Waiting Period: None<br />
· Separate Lifetime maximum: $1500<br />
· Dependent children to age 19 only<br />
Dental Employee Only Employee & Spouse<br />
Employee & Children<br />
(up to age 26)<br />
Employee & Family<br />
Basic Bi-Weekly Deduction $8.39 $15.77 $21.80 $29.17<br />
Enhanced Bi-Weekly Deduction $13.31 $26.03 $31.64 $44.37<br />
5<br />
<strong>BRF</strong> <strong>Hospital</strong> <strong>Holdings</strong><br />
2013 - 2014 Benefits
Vision - AlwaysCare<br />
EXAM covered every 12 months<br />
<br />
<br />
Prescription Glasses<br />
Standard Plastic Lenses covered every 12 months<br />
Frames - once every 12 months<br />
<br />
<br />
Once every 12 months<br />
Contact Lenses<br />
Includes evaluation, fitting, and follow-up care<br />
Vision Care Services In-Network Out-of-Network Allowance<br />
Exam $10 Copay Up to $35<br />
Materials<br />
Standard Plastic Lenses:<br />
Single Vision<br />
Bifocal Lined<br />
Trifocal Lined<br />
Lenticular<br />
Progressive<br />
$0 Copay<br />
Covered<br />
Covered<br />
Covered<br />
$80 Allowance<br />
$70 Allowance<br />
Up to $25<br />
Up to $40<br />
Up to $50<br />
Up to $50<br />
Up to $50<br />
Lens Options:<br />
Scratch resistant coating<br />
Solid / Gradient tint<br />
UV Coating<br />
Frames:<br />
Members choose from any<br />
frame available at provider<br />
locations<br />
Covered<br />
Covered<br />
Covered<br />
$130 Retail Allowance<br />
($94 retail frame at Costco, WalMart, and<br />
Sam’s Club)<br />
N/A<br />
N/A<br />
N/A<br />
Up to $50 retail allowance<br />
Contact Lenses: Includes evaluation, fitting,<br />
and follow up care<br />
Elective<br />
<strong>Medical</strong>ly Necessary<br />
No Copay<br />
Up to $130 Retail<br />
Covered in full<br />
Up to $100 retail<br />
Up to $210 retail<br />
Vision Employee Only Employee & Spouse<br />
Employee & Children<br />
(14 days up to age 26)<br />
Employee & Family<br />
Bi-Weekly Deduction $3.54 $5.95 $6.08 $9.80<br />
<strong>BRF</strong> <strong>Hospital</strong> <strong>Holdings</strong><br />
2013 - 2014 Benefits<br />
6
Voluntary Life & AD&D - Mutual Of Omaha<br />
Life Benefit Employee Spouse Dependent<br />
Amount<br />
Increments of $10,000 up to 7 times<br />
annual salary or $300,000<br />
Increments of $10,000 up to $100,000<br />
$10,000 for children 14 days old up to age 26<br />
Age Reduction: Benefit will be reduced<br />
by 50% at age 70 and will terminate at<br />
retirement<br />
Employee must elect coverage for<br />
spouse to be eligible. Benefit not to<br />
exceed 100% of employees elected<br />
amount, benefit will terminate at<br />
employee age 70<br />
Employee must elect coverage for child(ren)<br />
to be eligible. Newborn children to age 13<br />
days are not eligible for a benefit.<br />
Guarantee Issue<br />
$300,000<br />
$100,000<br />
$10,000<br />
Eligibility<br />
Accidental Death &<br />
Dismemberment<br />
Living Care Benefit<br />
Guarantee Issue<br />
Portability<br />
Conversion<br />
You must be actively at work (able to perform all normal duties of your job) to be eligible for this benefit. Your spouse must be<br />
able to perform normal activities and not confined at home, in a hospital, or in any other care facility<br />
AD&D coverage is available if you or your dependents are injured or die as a result of an accident, and the injury or death is<br />
independent of sickness and all other causes. The benefit amount depends on the type of loss incurred, and is either all or a<br />
portion of the Principal Sum, which is equal to the amount of the life insurance benefit.<br />
When diagnosed as terminally ill (having 12 months or less to live), you may withdraw up to 80% of your life insurance coverage<br />
to a maximum of $240,000. The death benefit will be reduced by the amount withdrawn.<br />
For timely entrants enrolled within 31 days of becoming eligible, the Guarantee Issue amount is available without any Evidence of<br />
Insurability requirement. For late enrollees, Evidence of Insurability will be required for any amount and it will be provided at your<br />
own expense.<br />
When you are no longer an eligible employee, you will have 31 days to port coverage. This feature allows you to continue this<br />
insurance for yourself and your dependents (if applicable), allowing you to keep the coverage until you are 70.<br />
When you are no longer an eligible employee, you will have 31 days to convert coverage. This takes the term life policy to an<br />
individual life insurance policy.<br />
Waiver of Premium If you become totally and permanently disabled prior to age 60, your life insurance will continue in force without further payment<br />
of premium on a year-to-year basis. You must be totally disabled for 9 months in order to qualify, and waiver terms at age 65.<br />
*Subject to periodic submission of evidence of total and permanent disability.<br />
Voluntary Life & AD&D Insurance Bi-Weekly Deduction<br />
Spouse age is based on Employee age<br />
Age $10,000 $20,000 $30,000 $40,000 $50,000 $60,000 $70,000 $80,000 $90,000 $100,000 $200,000 $300,000<br />
0-19 $0.31 $0.63 $0.94 $1.26 $1.57 $1.88 $2.20 $2.51 $2.82 $3.14 $6.28 $9.42<br />
20-24 $0.44 $0.88 $1.32 $1.75 $2.19 $2.63 $3.07 $3.51 $3.95 $4.38 $8.77 $13.15<br />
25-29 $0.44 $0.88 $1.32 $1.75 $2.19 $2.63 $3.07 $3.51 $3.95 $4.38 $8.77 $13.15<br />
30 - 34 $0.44 $0.88 $1.32 $1.75 $2.19 $2.63 $3.07 $3.51 $3.95 $4.38 $8.77 $13.15<br />
35 - 39 $0.52 $1.03 $1.55 $2.07 $2.58 $3.10 $3.62 $4.14 $4.65 $5.17 $10.34 $15.51<br />
40 - 44 $0.70 $1.40 $2.10 $2.81 $3.51 $4.21 $4.91 $5.61 $6.31 $7.02 $14.03 $21.05<br />
45 - 49 $1.01 $2.01 $3.02 $4.02 $5.03 $6.04 $7.04 $8.05 $9.06 $10.06 $20.12 $30.18<br />
50 - 54 $1.55 $3.09 $4.64 $6.18 $7.73 $9.28 $10.82 $12.37 $13.92 $15.46 $30.92 $46.38<br />
55 - 59 $2.43 $4.86 $7.30 $9.73 $12.16 $14.59 $17.03 $19.46 $21.89 $24.32 $48.65 $72.97<br />
60 - 64 $3.68 $7.36 $11.04 $14.71 $18.39 $22.07 $25.75 $29.43 $33.11 $36.78 $73.57 $110.35<br />
65 - 69 $6.17 $12.34 $18.51 $24.68 $30.85 $37.02 $43.20 $49.37 $55.54 $61.71 $123.42 $185.12<br />
Age $5,000 $10,000 $15,000 $20,000 $25,000 $30,000 $35,000 $40,000 $45,000 $50,000 $100,000 $150,000<br />
70 -74 $5.82 $11.63 $14.45 $23.26 $29.08 $34.89 $40.71 $46.52 $52.34 $58.15 $116.31 $174.46<br />
75-99 $10.94 $21.88 $32.82 $43.76 $54.70 $65.64 $76.59 $87.53 $98.47 $109.41 $218.82 $328.22<br />
Voluntary Life & AD&D Insurance Bi-Weekly Deduction for Children<br />
Age $10,000<br />
14 days up to 26 years $1.06<br />
7<br />
<strong>BRF</strong> <strong>Hospital</strong> <strong>Holdings</strong><br />
2013 - 2014 Benefits
Short Term Disability - Mutual of Omaha<br />
Income Protection<br />
Insurance<br />
Eligibility<br />
Maximum Weekly Benefit<br />
Waiver of Premium<br />
Pays a benefit for a disability resulting from a covered injury or sickness. Benefits begin on the 8th day (after a 7<br />
day waiting period) for both injury and sickness, and continue while you are disabled up to the maximum benefit<br />
duration of 12 weeks.<br />
You must be actively at work (able to perform all normal duties of your job) to be eligible for coverage.<br />
You have the option to elect either 40% or 60% of your weekly covered earnings to $1,500. The minimum benefit<br />
amount is $25.<br />
Beginning on the first of the month following the date of disability, you will not be required to pay premiums during<br />
any time of approved total or partial disability.<br />
Disability<br />
Partial Disability<br />
Continuation of Disability<br />
Pre-Existing Condition<br />
Benefit Exclusions<br />
Portability<br />
Disability and disabled mean that because of an injury or illness, a significant change in your mental or functional<br />
abilities has occurred, for which you are prevented from performing at least one of the material duties of your<br />
regular job and are unable to generate current earnings which exceed 99% of your weekly earnings from your<br />
regular job. You can be totally or partially disabled during the elimination period.<br />
If you become disabled and can work part time (but not full time), you may be eligible for partial disability benefits,<br />
which will help supplement your income until you are able to return to work full time.<br />
If you return to work full time but become disabled from the same disability within two weeks of returning to work,<br />
you will begin receiving benefits again immediately.<br />
Any sickness or injury for which you have received medical treatment, consultation, care or services (including<br />
diagnostic measures or took prescribed medications) during the three (3) months prior to the coverage effective<br />
date. Benefits will not be paid for a disability caused by, contributed to by or resulting from a pre-existing condition<br />
unless the insured has been actively at work for one (1) full day following the end of six (6) consecutive months<br />
from the date he/she became an Insured.<br />
You will not receive benefits in the following circumstances:<br />
Your disability is the result of a self-inflicted injury<br />
An act of war, declared or undeclared<br />
Your disability is the result of committing a felony<br />
Your disability is covered under a worker’s compensation plan and/or is due to a job-related sickness or injury<br />
which occurs out of or in the course of work for wage or profit<br />
When you are no longer an eligible employee, you will have 31 days to port coverage. This will allow you to keep<br />
the coverage up to age 70.<br />
Your benefit is based on your Salary. Calculate your Bi-Weekly deduction using<br />
the following examples (This example assumes a 40 hour work week):<br />
40% of your Salary 60% of your Salary<br />
Hourly Pay Rate 20.00 20.00<br />
Times 40 - weekly payroll 800.00 800.00<br />
Times 40% / 60% - weekly benefit 320.00 480.00<br />
Times .060 19.20 28.80<br />
Times 12 / by 26 to get your<br />
Bi-Weekly Deduction<br />
$8.86 $13.29<br />
<strong>BRF</strong> <strong>Hospital</strong> <strong>Holdings</strong><br />
2013 - 2014 Benefits<br />
8
Long Term Disability - Mutual of Omaha<br />
Eligibility<br />
Maximum Monthly Benefit<br />
Maximum Benefit Duration<br />
Elimination Period<br />
Waiver of Premium<br />
Survivor Income Benefit<br />
You must be actively at work (able to perform all normal duties of your job) to be eligible for coverage.<br />
You have the option to elect either 40% or 60% of your monthly covered earnings to a maximum of $12,000 per<br />
month. The minimum benefit is $100.<br />
Benefits continue to normal social security retirement age while you remain disabled.<br />
90 days - The number of days you must be disabled prior to collecting disability benefits.<br />
You will not be required to pay premiums during any time of approved total or partial disability.<br />
A 3 months survivor benefit may be paid to your beneficiary if you should die while receiving qualifying disability<br />
payments.<br />
Disability<br />
Partial Disability<br />
Continuation of Disability<br />
Pre-Existing Condition<br />
Benefit Exclusions<br />
Benefit Reductions<br />
Benefit Termination<br />
Portability<br />
Disability and disabled mean that because of an injury or illness, a significant change in your mental or functional<br />
abilities has occurred, for which you are prevented from performing at least one of the material duties of your regular<br />
job and are unable to generate current earnings which exceed 99% of your weekly earnings from your regular job.<br />
You can be totally or partially disabled during the elimination period.<br />
If you become disabled and can work part time (but not full time), you may be eligible for partial disability benefits,<br />
which will help supplement your income until you are able to return to work full time.<br />
If you return to work full time but become disabled from the same disability within six months of returning to work,<br />
you will begin receiving benefits again immediately.<br />
Any sickness or injury for which you have received medical treatment, consultation, care or services (including<br />
diagnostic measures or the taking of prescribed medications) during the 3 months prior to the coverage effective date.<br />
A disability arising from any such sickness or injury will be covered only if it begins after you have performed your<br />
regular occupation on a full time basis for 12 months following the coverage effective date.<br />
You will not receive benefits in the following circumstances:<br />
Your disability is the result of a self-inflicted injury<br />
You were involved in a felony commission, act of war or participation in a riot<br />
* See certificate for full list of exclusions<br />
Your benefits may be reduced if you are receiving benefits from any of the following sources:<br />
Any compulsory benefit act or law (such as state disability plans)<br />
Any governmental retirement system earned as a result of working for the current policyholder<br />
Any disability or retirement benefit received under a retirement plan<br />
Any Social Security, or similar plan or act, benefits<br />
Earnings the insured earns or receives from any form of employment<br />
Workers compensation<br />
<br />
This coverage will terminate when you terminate employment with this policyholder or at your retirement.<br />
When you are no longer an eligible employee, you will have 31 days to port coverage, allowing you to continue this<br />
insurance until you are 70.<br />
Your benefit is based on your Salary. Calculate your Bi-Weekly deduction using the<br />
following examples (This example assumes a 40 hour work week):<br />
40% of your Salary 60% of your Salary<br />
Hourly Pay Rate 20.00 20.00<br />
Times 40 - weekly payroll 800.00 800.00<br />
Times 52 / 12 3,466.67 3,466.67<br />
Times 40% / 60% - monthly benefit 1,386.67 2,080.00<br />
Times .0136 18.86 28.29<br />
Times 12 / 26 to get your<br />
Bi-Weekly Deduction<br />
$8.70 $13.06<br />
9<br />
<strong>BRF</strong> <strong>Hospital</strong> <strong>Holdings</strong><br />
2013 - 2014 Benefits
Critical Illness - HM Life<br />
Covered Critical Illnesses <br />
Covered<br />
Critical Illness<br />
Myocardial Infarction (Heart<br />
Attack)<br />
Percentage of<br />
Face amount<br />
Covered<br />
Critical Illness<br />
100% + Major Organ Transplant 100%<br />
Percentage of<br />
Face amount<br />
Coronary Artery Bypass 25% * End-stage Renal Disease<br />
(Kidney Disease)<br />
Stroke 100% Loss of Sight, Speech or<br />
Hearing<br />
100%<br />
100% *<br />
Invasive Cancer 100% + Coma 100% *<br />
Carcinoma in Situ 25 % * Paralysis 100% *<br />
Skin Cancer 10% *<br />
+ Benefits paid for Carcinoma in Situ, Skin Cancer and Coronary Artery Bypass Surgery, reduce the benefit payable for<br />
subsequently diagnosed Invasive Cancer and Heart Attack, respectively.<br />
* Payable once per lifetime. Minimum benefit is $250.<br />
Plan Type & Age<br />
Guidelines<br />
Benefit Options<br />
Guarantee Issue Amount<br />
Healthy Screening<br />
Coverage<br />
Pays a lump sum for<br />
three types of<br />
diagnoses – initial,<br />
reoccurrence and<br />
additional covered<br />
occurrences<br />
Employee and Spouse may be covered from ages 18 to 69 years, benefits reduce by 50% at 70<br />
Children up to age 26<br />
Employee - $2,500 up to $100,000; Spouse – Up to 100% of employee amount to a max of $100,000; Children<br />
automatically get 25% of employee amount up to $20,000 at no additional cost<br />
Employee - $25,000; Spouse - 50% of employee amount<br />
$50 - One per covered individual per year. Benefit paid regardless of diagnosis or results of the test.<br />
First Occurrence – provides a lump sum payment when a covered critical illness is first diagnosed<br />
Reoccurrence – pays when a covered critical illness reoccurs. The reoccurrence must be separated from the initial<br />
diagnosis by at least 180 days (365 days treatment - free for cancer) or separated from another reoccurrence by at least<br />
180 days (365 days treatment - free for cancer)<br />
Additional Occurrence – pays an additional benefit upon the diagnosis of a covered condition for which benefits<br />
previously have not been paid. The diagnosis must be separated from the other critical illness by at least 180 days<br />
Continuation of Coverage Employees continuously insured for at least 12 consecutive months under this plan or a prior plan may have the<br />
opportunity to continue their coverage.<br />
Pre-Existing Condition<br />
Limitation<br />
Issue Age<br />
No benefits will be provided for the first 12 months a person is covered under the policy for conditions for which medical<br />
advice or treatment was received or recommended during the 12 month period prior to the effective date of coverage.<br />
If elected, your Critical Illness deductions will not change from year to year; your deductions will remain the same<br />
throughout the life of your policy.<br />
Employee<br />
Issue Age<br />
Critical Illness Benefit Amounts & Bi-Weekly Deduction<br />
$2,500 $5,000 $10,000 $15,000 $20,000 $25,000 $30,000 $50,000 $75,000 $100,000<br />
18 - 24 $0.47 $0.70 $1.18 $1.65 $2.13 $2.60 $3.07 $4.97 $7.34 $9.55<br />
25 - 29 $0.69 $1.06 $1.80 $2.54 $3.28 $4.02 $4.76 $7.71 $11.40 $14.93<br />
30 - 34 $1.03 $1.61 $2.77 $3.93 $5.09 $6.25 $7.41 $12.05 $17.84 $23.47<br />
35 - 39 $1.58 $2.54 $4.44 $6.35 $8.26 $10.17 $12.07 $19.70 $29.24 $38.61<br />
40 - 44 $2.42 $3.98 $7.08 $10.18 $13.28 $16.39 $19.49 $31.90 $47.41 $62.76<br />
45 - 49 $3.59 $5.99 $10.79 $15.58 $20.38 $25.17 $29.97 $49.15 $73.13 $96.94<br />
50 - 54 $5.17 $8.74 $15.88 $23.03 $30.17 $37.32 $44.46 $73.04 $108.77 $144.32<br />
55 - 59 $6.94 $11.92 $21.89 $31.86 $41.83 $51.80 $61.77 $101.65 $151.49 $201.17<br />
60 - 64 $8.67 $15.09 $27.93 $40.77 $53.61 $66.45 $79.30 $130.66 $194.88 $258.92<br />
65 - 69 $9.20 $16.20 $30.21 $44.21 $58.22 $72.22 $86.23 $142.25 $212.28 $282.15<br />
Guarantee Issue - Employee Only<br />
<strong>BRF</strong> <strong>Hospital</strong> <strong>Holdings</strong><br />
2013 - 2014 Benefits<br />
10
Flexible Spending Account - Boon-Chapman<br />
Flexible Spending Account (FSA)<br />
This benefit provides you with the opportunity to set aside<br />
tax-exempt dollars for out-of-pocket health care or<br />
dependent care expenses incurred by you and/or your<br />
eligible dependents. The deduction is made before taxes<br />
are computed, thus making the spending account dollars<br />
tax-free. FSA contributions are “use it or lose it” and<br />
balances do not roll over from year to year.<br />
You will have two different FSA policy years, the<br />
first will begin October 1, 2013 and will end<br />
December 31, 2013. The second FSA policy year will<br />
begin January 1, 2014 and will end December 31,<br />
2014.<br />
You must determine the amount to be deducted from each<br />
paycheck, and you will be provided with a Debit Card. Your<br />
Health Care election will be pre-loaded with this amount for<br />
your use throughout the 2013 Plan Year. The dependent<br />
Care election is not preloaded and is only available as the<br />
funds are payroll deducted. Determine the amount to be<br />
withheld by forecasting your out-of-pocket health care and/<br />
or dependent care expenses for the entire Plan year, plus<br />
the grace period (January 1 st through March 15 th ). To<br />
access the money in your account, you can either use your<br />
FSA Debit Card at the time of service, or you can file a<br />
claim form to request reimbursement. This form is available<br />
in your HR / Benefits Department or you can find it on the<br />
website www.enrollme.biz.<br />
Qualifications and Eligible Expenses:<br />
Many health care expenses, such as Copayments and<br />
deductibles, are not fully reimbursed by health, dental, or<br />
vision insurance and may be eligible for reimbursement<br />
through a Health Care FSA. For a detailed list of health care<br />
expenses that may qualify for reimbursement under the<br />
Health Care Spending Account, visit the website<br />
www.boonchapman.com.<br />
Dependent Care FSA<br />
Qualifications:<br />
You may receive tax-exempt reimbursements for the care<br />
of certain individuals in your household, which includes your<br />
dependent children age 12 or younger and any other<br />
individuals who reside with you and who rely on you for at<br />
least half of their support or are physically or mentally<br />
unable to care for themselves.<br />
Eligible Expenses:<br />
Daycare expenses are defined as those that are necessary<br />
in order for you (and your spouse, if you’re married) to<br />
continue working. You are required to report on your<br />
annual federal income tax return the name(s) of those<br />
providers of dependent care expenses whose expenses<br />
have been reimbursed to you through your Dependent Care<br />
Account.<br />
Eligible Dependent Care Account expenses include:<br />
<br />
<br />
<br />
<br />
<br />
<br />
<br />
Day-care costs for children 12 and under.<br />
Schooling costs, not including food and clothing, for<br />
either private or public schools, for children not yet in<br />
kindergarten.<br />
If expenses for food and clothing cannot be separated<br />
from the total cost of child care, then they are eligible<br />
expenses.<br />
If your child is 12 years or younger and you pay for<br />
before/after-school care, it is reimbursable<br />
Babysitting and licensed day-care center costs<br />
Minimal housekeeping services in your home as long as<br />
day care is the primary duty<br />
Elder care if dependent is claimed on your tax return<br />
Costs of transportation, overnight camping, nursing care<br />
facilities, and the schooling costs of children in the first<br />
grade or above are generally ineligible expenses.<br />
Health Care FSA Contributions<br />
Minimum per year $150<br />
Maximum per year $2,500<br />
Dependent Care FSA Contributions<br />
Minimum per year $150<br />
Maximum per year $5,000 per household<br />
11<br />
<strong>BRF</strong> <strong>Hospital</strong> <strong>Holdings</strong><br />
2013 - 2014 Benefits
Online Enrollment Instructions<br />
The Benefit Administration Systems website is home to all of the tools and resources you will need during Annual<br />
Enrollment and throughout the year. It is also where you will enroll in your benefits. See below for a list of detailed<br />
instructions that will navigate you through the enrollment process with ease.<br />
Log On<br />
Using any computer with Internet access, go to<br />
www.enrollme.biz<br />
Enter your user name and password:<br />
Employee Username – Your Social Security<br />
Number (no dashes)<br />
Password – Last 4 digits of your Social Security<br />
Number<br />
You will change your password on the next screen -<br />
Re-enter the last 4 digits of your Social Security<br />
Number as the previous password, enter a new one<br />
that is at least 5 characters, then re-enter the new<br />
password<br />
Click ‘Enroll In Benefits’ to proceed to your benefits<br />
Employee / Dependent Information<br />
<br />
<br />
<br />
<br />
From the menu on the left, click:<br />
Employee Info – Verify your information on this page<br />
and make necessary changes to address, phone<br />
number, and/or email address<br />
Dependent Info – Add or make changes to Dependent<br />
information on this screen<br />
Enter dependent information BEFORE selecting<br />
your benefits<br />
SSN, DOB, and Address are required for<br />
each dependent<br />
*Note: Specific documentation required -<br />
See page 1 if enrolling dependents in<br />
<strong>Medical</strong> coverage<br />
Beneficiary info – Add or make changes to beneficiary<br />
information on this screen. Since the company<br />
provides a Basic Life policy all employees need to<br />
provide this information<br />
Electing Benefits<br />
<br />
<br />
<br />
Click on each of the benefits from the left menu. On<br />
the right, you will have the option to attain more<br />
information and elect that benefit<br />
If you are interested in the benefit, check the ‘I elect<br />
coverage for this benefit’ box, and select the<br />
dependents you wish to cover under that benefit<br />
You may also use the left and right arrow keys to<br />
scroll through each benefit<br />
Confirm<br />
<br />
<br />
<br />
<br />
<br />
Once you’ve made your choices, from the menu on<br />
the left, click Confirmation<br />
Verify the elections are what you want<br />
Check the ’I Accept’ Box, enter your NEW password,<br />
and click the blue ‘I Accept’ button<br />
Wait for a message to appear telling you that you<br />
have successfully enrolled in benefits<br />
Print a confirmation of your enrollment or enter your<br />
email address at the top of the screen to have a copy<br />
of your confirmation page emailed directly to you<br />
If you have any questions regarding the online<br />
enrollment or if you do not have access to a<br />
computer and are unable to enroll online, please<br />
contact HUB International at 318-629-8769 or<br />
877-309-2224, or you can contact HUB by email at<br />
<strong>BRF</strong>HH@hubinternational.com.<br />
Note: You MUST go to the online enrollment<br />
website whether enrolling in benefits or not<br />
to:<br />
1) Enter beneficiaries for your Basic Life Policy<br />
2) Decline <strong>Medical</strong> coverage by electronically<br />
signing with your Pin number<br />
<strong>BRF</strong> <strong>Hospital</strong> <strong>Holdings</strong><br />
2013 - 2014 Benefits<br />
12
<strong>BRF</strong> <strong>Hospital</strong> <strong>Holdings</strong><br />
Benefit Guide 2013 - 2014<br />
8/19/13