1 home visit checklist for parent mentors initial ... - UT Southwestern
1 home visit checklist for parent mentors initial ... - UT Southwestern
1 home visit checklist for parent mentors initial ... - UT Southwestern

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
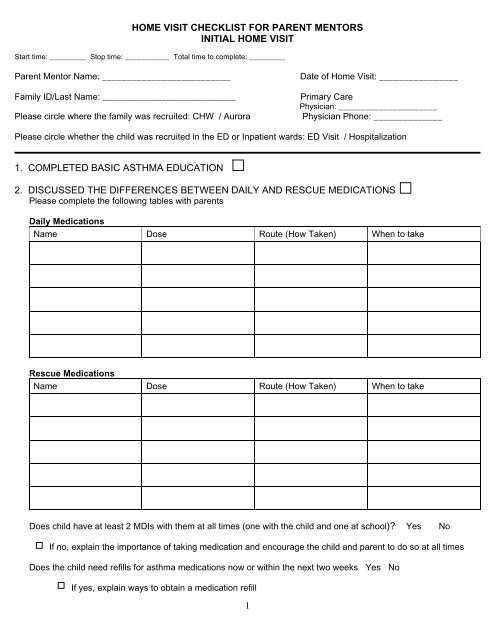
HOME VISIT CHECKLIST FOR PARENT MENTORS<br />
INITIAL HOME VISIT<br />
Start time: _________ Stop time: ___________ Total time to complete: _________<br />
Parent Mentor Name: __________________________<br />
Family ID/Last Name: ___________________________<br />
Please circle where the family was recruited: CHW / Aurora<br />
Date of Home Visit: ________________<br />
Primary Care<br />
Physician: ______________________<br />
Physician Phone: ______________<br />
Please circle whether the child was recruited in the ED or Inpatient wards: ED Visit / Hospitalization<br />
1. COMPLETED BASIC ASTHMA EDUCATION<br />
2. DISCUSSED THE DIFFERENCES BETWEEN DAILY AND RESCUE MEDICATIONS<br />
Please complete the following tables with <strong>parent</strong>s<br />
Daily Medications<br />
Name Dose Route (How Taken) When to take<br />
Rescue Medications<br />
Name Dose Route (How Taken) When to take<br />
Does child have at least 2 MDIs with them at all times (one with the child and one at school) Yes No<br />
If no, explain the importance of taking medication and encourage the child and <strong>parent</strong> to do so at all times<br />
Does the child need refills <strong>for</strong> asthma medications now or within the next two weeks Yes No<br />
If yes, explain ways to obtain a medication refill<br />
1
Does the child have any asthma medications that are expired, out, or almost out<br />
Yes No<br />
If yes, explain ways to obtain a medication refill<br />
3. ASTHMA EQUIPTMENT<br />
Are nebulizer machines, spacers, and peak flow meters all in working condition Yes No<br />
If no, encourage families to contact their health care provider to obtain new equipment<br />
4. HELP FAMILIES IDENTIFY EARLY AND LATE WARNING SIGNS OF AN ASTHMA ATTACK<br />
Early Warning Signs<br />
Late Warning Signs<br />
5. ASTHMA CARE PLANS<br />
Does child have a written asthma care plan from his/her health care provider (Please circle) Yes / No<br />
If yes, does he/she follow his/her asthma care plan (Please circle) Yes / No<br />
If yes, is there also a care plan <strong>for</strong>:<br />
School Daycare Babysitters Other: __________________________<br />
If no asthma care plan or if family doesn’t follow care plan, why / Additional Comments<br />
Parent Mentor Review (place a check next to those discussed with <strong>parent</strong>; if something doesn’t<br />
apply put “NA” in the box)<br />
How to read/use asthma care plans<br />
The importance of following asthma care plan<br />
The importance of keeping asthma care plan at school/daycare/babysitters<br />
Asthma care plan when child is showing early warning signs<br />
Asthma care plan when child is showing late warning signs<br />
Discussed daily asthma prevention<br />
2
6. PEAK FLOW METERS<br />
Does child have a peak flow meter (Please circle) Yes / No<br />
NA<br />
If no explain to <strong>parent</strong>s the importance of peak flow meters, instruct <strong>parent</strong> how to obtain<br />
one (call health care provider<br />
If yes, does the child use the peak flow meter when necessary (Please circle) Yes / No<br />
NA<br />
What is the child’s: Green zone: ________________<br />
Yellow Zone: ________________<br />
Red Zone:<br />
________________<br />
If no peak flow meter, family doesn’t regularly use peak flow meter, why<br />
Additional Comments<br />
______________________________________________________________________<br />
______________________________________________________________________<br />
______________________________________________________________________<br />
______________________________________________________________________<br />
______________________________________________________________________<br />
______________________________________________________________________<br />
Parent Mentor Review (place a check next to those discussed with <strong>parent</strong>; if something doesn’t<br />
apply put “NA” in the box)<br />
When/how to use a peak flow meter<br />
Peak flow chart<br />
How to track peak flow results<br />
How to clean peak flow meter<br />
How to obtain new peak flow meter if lost or broken<br />
Special recommendations from the child’s primary care provider<br />
7. TRIGGERS<br />
What are some things that make your child have an asthma attack (Check all that apply)<br />
Tobacco Smoke<br />
Mold<br />
Strong Smells<br />
Pets<br />
Dust<br />
Exercise<br />
Foods<br />
Cockroaches<br />
Dust mites<br />
Colds or Flu<br />
Pollution<br />
Grass<br />
Flowers<br />
Trees<br />
Humidity<br />
Cold or hot weather (temperature changes)<br />
Ozone<br />
Heat<br />
Additional things that may make your child have an asthma attack<br />
_______________________________________________________________________________<br />
_______________________________________________________________________________<br />
_______________________________________________________________________________<br />
_______________________________________________________________________________<br />
3
Trigger/Environmental Control (Check all discussed with <strong>parent</strong> if not applicable put NA in box)<br />
Damp dust surfaces weekly<br />
Manage pests in the <strong>home</strong><br />
Avoid food allergens<br />
Take steps to eliminate smoke in the <strong>home</strong><br />
Medications taken be<strong>for</strong>e and attainable during<br />
exercise<br />
Vacuum carpeted areas and furniture at least<br />
once a week<br />
Pillow Covers<br />
Mattress covers<br />
Establish “pet free zones”<br />
Eliminate or wash heavy curtains<br />
Eliminate stuffed furniture from the child’s<br />
bedroom<br />
Avoid strong smells (perfumes, scented lotion,<br />
cleaning supplies, bleach)<br />
Keep areas free of water and dampness<br />
Get an annual flu shot<br />
Wash bedding in hot water weekly<br />
Change filters in air conditioners and humidifiers<br />
Keep child away from trees and outdoor<br />
triggers<br />
Keep windows shut and use air conditioners<br />
instead of fans<br />
Stay inside during very hot/cold temperatures Keep child away from fresh flowers<br />
Smokers in the <strong>home</strong> (Smoking Cessation)<br />
8. ASTHMA AND SCHOOL/DAY CARE<br />
Have <strong>parent</strong>s:<br />
Communicated asthma care plan with school/day care personnel Yes No<br />
Notified school/daycare personnel about medications taken during school/day care hours Yes No<br />
Given school/daycare emergency contact in<strong>for</strong>mation Yes No<br />
Medications given at school/daycare<br />
Medication Name How much to take (dose) When to take<br />
Triggers:<br />
What are some things that make your child have an asthma attack at school/daycare (Check All that<br />
apply<br />
Stuffed Animals<br />
Pillows<br />
Dust on bookshelves and toys<br />
Classroom pets<br />
Plants or flowers<br />
Chalk dust<br />
Strong scents like<br />
4
Trigger/Environmental Control at school/daycare<br />
(Check all discussed with <strong>parent</strong> if not applicable put NA in box)<br />
Stuffed animals<br />
Dust<br />
Plants or flowers<br />
Food<br />
Change in weather<br />
Pillows<br />
Classroom pets<br />
Chalk dust<br />
Exercise<br />
Strong scents<br />
Parent Mentor Review (place a check next to those discussed with <strong>parent</strong>; if something doesn’t<br />
apply put “NA” in the box)<br />
Importance of having asthma care plan at school<br />
Importance of notifying personnel about medications taken during school/daycare hours<br />
Exercise-induced asthma<br />
Comments<br />
_____________________________________________________________________________<br />
_____________________________________________________________________________<br />
_____________________________________________________________________________<br />
_____________________________________________________________________________<br />
_____________________________________________________________________________<br />
_____________________________________________________________________________<br />
9. TRACKING REGULAR AND FOLLOW-UP APPOINTMENTS<br />
Does the child have a primary health care provider Yes No<br />
Does the child and family have regular scheduled <strong>visit</strong>s <strong>for</strong> asthma Yes No<br />
Has the child and family missed any of their child’s routine <strong>visit</strong>s <strong>for</strong> asthma Yes No<br />
If child and family have missed any appointments why/Comments<br />
__________________________________________________________________________________<br />
__________________________________________________________________________________<br />
__________________________________________________________________________________<br />
__________________________________________________________________________________<br />
__________________________________________________________________________________<br />
Parent Mentor Review (place a check next to those discussed with <strong>parent</strong>; if something doesn’t apply put<br />
“NA” in the box)<br />
Importance of scheduled <strong>visit</strong>s<br />
Identify contact in<strong>for</strong>mation <strong>for</strong> health care providers (give families contact resource sheet)<br />
Identify next routine appointment with health care provider<br />
Identify monthly meeting with other asthma families<br />
10. CARE PLAN AFTER ED VISIT AND HOSPITALIZATION<br />
Did family receive a care plan after ED <strong>visit</strong> or Hospitalization Yes No<br />
Does the child have an asthma specialist Yes No<br />
Date of the next follow-up appointment with health care provider: _____________________________<br />
5