

Haematologica 2000;85:supplement to no. 10 - Supplements ...
Haematologica 2000;85:supplement to no. 10 - Supplements ...
Haematologica 2000;85:supplement to no. 10 - Supplements ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
32<br />
Immune Tolerance and the Treatment of Hemophilacs with an Inhibi<strong>to</strong>r<br />
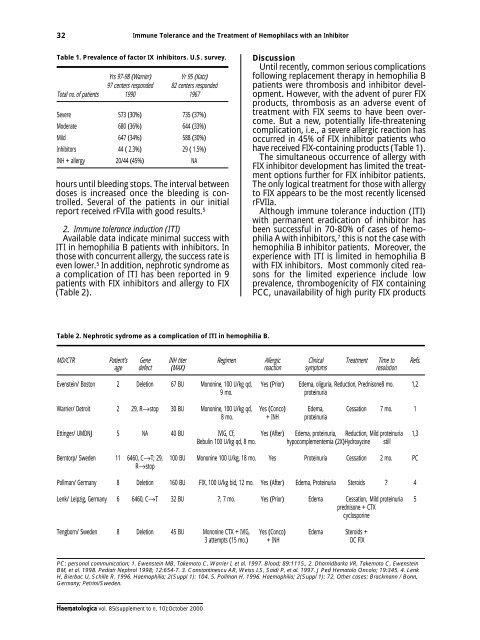
Table 1. Prevalence of fac<strong>to</strong>r IX inhibi<strong>to</strong>rs. U.S. survey.<br />
Yrs 97-98 (Warrier) Yr 95 (Katz)<br />
97 centers responded 82 centers responded<br />
Total <strong>no</strong>. of patients 1990 1967<br />
Severe 573 (30%) 735 (37%)<br />
Moderate 680 (36%) 644 (33%)<br />
Mild 647 (34%) 588 (30%)<br />
Inhibi<strong>to</strong>rs 44 ( 2.3%) 29 ( 1.5%)<br />
INH + allergy 20/44 (45%) NA<br />
hours until bleeding s<strong>to</strong>ps. The interval between<br />
doses is increased once the bleeding is controlled.<br />
Several of the patients in our initial<br />
report received rFVIIa with good results. 5<br />
2. Immune <strong>to</strong>lerance induction (ITI)<br />
Available data indicate minimal success with<br />
ITI in hemophilia B patients with inhibi<strong>to</strong>rs. In<br />
those with concurrent allergy, the success rate is<br />
even lower. 5 In addition, nephrotic syndrome as<br />
a complication of ITI has been reported in 9<br />
patients with FIX inhibi<strong>to</strong>rs and allergy <strong>to</strong> FIX<br />
(Table 2).<br />
Discussion<br />
Until recently, common serious complications<br />
following replacement therapy in hemophilia B<br />
patients were thrombosis and inhibi<strong>to</strong>r development.<br />
However, with the advent of purer FIX<br />
products, thrombosis as an adverse event of<br />
treatment with FIX seems <strong>to</strong> have been overcome.<br />
But a new, potentially life-threatening<br />
complication, i.e., a severe allergic reaction has<br />
occurred in 45% of FIX inhibi<strong>to</strong>r patients who<br />
have received FIX-containing products (Table 1).<br />
The simultaneous occurrence of allergy with<br />
FIX inhibi<strong>to</strong>r development has limited the treatment<br />
options further for FIX inhibi<strong>to</strong>r patients.<br />
The only logical treatment for those with allergy<br />
<strong>to</strong> FIX appears <strong>to</strong> be the most recently licensed<br />
rFVIIa.<br />
Although immune <strong>to</strong>lerance induction (ITI)<br />
with permanent eradication of inhibi<strong>to</strong>r has<br />
been successful in 70-80% of cases of hemophilia<br />
A with inhibi<strong>to</strong>rs, 7 this is <strong>no</strong>t the case with<br />
hemophilia B inhibi<strong>to</strong>r patients. Moreover, the<br />
experience with ITI is limited in hemophilia B<br />
with FIX inhibi<strong>to</strong>rs. Most commonly cited reasons<br />
for the limited experience include low<br />
prevalence, thrombogenicity of FIX containing<br />
PCC, unavailability of high purity FIX products<br />
Table 2. Nephrotic sydrome as a complication of ITI in hemophilia B.<br />
MD/CTR Patient’s Gene INH titer Regimen Allergic Clinical Treatment Time <strong>to</strong> Refs.<br />
age defect (MAX) reaction symp<strong>to</strong>ms resolution<br />
Evenstein/ Bos<strong>to</strong>n 2 Deletion 67 BU Mo<strong>no</strong>nine, <strong>10</strong>0 U/kg qd, Yes (Prior) Edema, oliguria, Reduction, Prednisone8 mo. 1,2<br />
9 mo. proteinuria<br />
Warrier/ Detroit 2 29, R→s<strong>to</strong>p 30 BU Mo<strong>no</strong>nine, <strong>10</strong>0 U/kg qd, Yes (Conco) Edema, Cessation 7 mo. 1<br />
8 mo. + INH proteinuria<br />
Ettinger/ UMDNJ 5 NA 40 BU IVIG, Cf, Yes (After) Edema, proteinuria, Reduction, Mild proteinuria 1,3<br />
Bebulin <strong>10</strong>0 U/kg qd, 8 mo. hypocomplementemia (2X)Hydroxyzine still<br />
Bern<strong>to</strong>rp/ Sweden 11 6460, C→T; 29, <strong>10</strong>0 BU Mo<strong>no</strong>nine <strong>10</strong>0 U/kg, 18 mo. Yes Proteinuria Cessation 2 mo. PC<br />
R→s<strong>to</strong>p<br />
Pollman/ Germany 8 Deletion 160 BU FIX, <strong>10</strong>0 U/kg bid, 12 mo. Yes (After) Edema, Proteinuria Steroids 4<br />
Lenk/ Leipzig, Germany 6 6460, C→T 32 BU , 7 mo. Yes (Prior) Edema Cessation, Mild proteinuria 5<br />
prednisone + CTX<br />
cyclosporine<br />
Tengborn/ Sweden 8 Deletion 45 BU Mo<strong>no</strong>nine CTX + IVIG, Yes (Conco) Edema Steroids +<br />
3 attempts (15 mo.) + INH DC FIX<br />
PC: personal communication; 1. Ewenstein MB, Takemo<strong>to</strong> C, Warrier I, et al. 1997. Blood; 89:1115., 2. Dharnidbarka VR, Takemo<strong>to</strong> C, Ewenstein<br />
BM, et al. 1998. Pediatr Nephrol 1998; 12:654-7. 3. Constantinescu AR, Weiss LS, Saidi P, et al. 1997. J Ped Hema<strong>to</strong>lo Oncolo; 19:345. 4. Lenk<br />
H, Bierbac U, Schille R. 1996. Haemophilia; 2(Suppl 1): <strong>10</strong>4. 5. Pollman H. 1996. Haemophilia; 2(Suppl 1): 72. Other cases: Brackmann / Bonn,<br />
Germany; Petrini/Sweden.<br />
<strong>Haema<strong>to</strong>logica</strong> vol. <strong>85</strong>(<strong>supplement</strong> <strong>to</strong> n. <strong>10</strong>):Oc<strong>to</strong>ber <strong>2000</strong>













