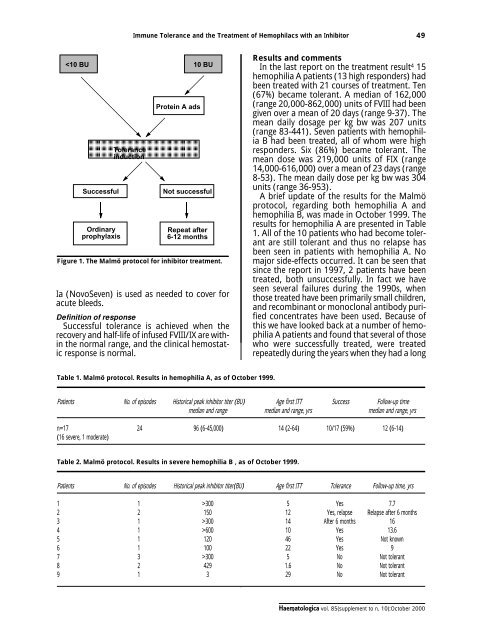
Immune Tolerance and the Treatment of Hemophilacs with an Inhibi<strong>to</strong>r 49 300 5 Yes 7.7 2 2 150 12 Yes, relapse Relapse after 6 months 3 1 >300 14 After 6 months 16 4 1 >600 <strong>10</strong> Yes 13.6 5 1 120 46 Yes Not k<strong>no</strong>wn 6 1 <strong>10</strong>0 22 Yes 9 7 3 >300 5 No Not <strong>to</strong>lerant 8 2 429 1.6 No Not <strong>to</strong>lerant 9 1 3 29 No Not <strong>to</strong>lerant <strong>Haema<strong>to</strong>logica</strong> vol. <strong>85</strong>(<strong>supplement</strong> <strong>to</strong> n. <strong>10</strong>):Oc<strong>to</strong>ber <strong>2000</strong>
50 E. Bern<strong>to</strong>rp et al. standing inhibi<strong>to</strong>r, prior <strong>to</strong> immune <strong>to</strong>lerance induction. In several patients it is evident that frequent treatment with FVIII alone or in combination with cyclophosphamide attenuated the anamnestic response. Thus the his<strong>to</strong>rical peak is probably <strong>no</strong>t really relevant <strong>to</strong> the type of immune response in certain patients entering the Malmö pro<strong>to</strong>col. This might explain the apparent decrease in the success rate during recent years. An alternative explanation may be that a switch from intermediate purity products <strong>to</strong> ultrapure or recombinant products has occurred, especially during the last decade. Whether product purity has an impact on IT <strong>to</strong>lerance outcome remains an open question, however. Our IT regimen for hemophilia A has changed somewhat, because of the observation that important fac<strong>to</strong>rs for a successful outcome are, among others, low current inhibi<strong>to</strong>r titer and long intervals since previous replacement therapy. This means that in a small child who develops an inhibi<strong>to</strong>r, the optimal use of the Malmö pro<strong>to</strong>col would require a long waiting period before IT is implemented. This could jeopardize the child´s health, due <strong>to</strong> recurrent hemorrhages. Therefore, in children with a newly detected inhibi<strong>to</strong>r we prefer <strong>to</strong> start immediately with a Bonn-like regimen, giving at least 200 units of FVIII per kg bw daily. The Malmö pro<strong>to</strong>col is mainly reserved for patients with longstanding inhibi<strong>to</strong>rs prior <strong>to</strong> IT. For hemophilia B, we have treated 9 patients as of Oc<strong>to</strong>ber 1999. The study material and the results are shown in Table 2, from which it can be seen that one relapse occurred after 6 months. This patient received a<strong>no</strong>ther course of treatment, which was terminated when the patient developed signs of an acute myocardial infarction. He later developed cardiac failure and expired from heart failure several years later. The treatment given was the full pro<strong>to</strong>col including protein A adsorption. The FIX concentrate used was a prothrombin complex concentrate. Thus, of the 9 patients treated of whom one had a low-responding inhibi<strong>to</strong>r, <strong>to</strong>lerance was achieved in 6 (67%). Relapse occurred in one patient so the final success rate was 5/9 (56%). The conclusions drawn from treatment of patients with hemophilia B are that the Malmö model gives a comparatively high response rate in the treatment of high-responding FIX inhibi<strong>to</strong>rs, and that only purified FIX concentrate should be used, in order <strong>to</strong> minimize the risk of thromboembolic complications. In addition, the short treatment period used for the Malmö pro<strong>to</strong>col should, from a theoretical point of view, minimize the risk of developing nephrotic syndrome, a k<strong>no</strong>wn complication of long-term high-dose FIX treatment. 5 REFERENCES 1. Nilsson IM, Jonsson S, Sundqvist SB, Ahlberg Å, Bergentz SE. A procedure for removing high titer antibodies by extracorporeal protein sepharose A adsorption in hemophilia: substitution therapy and surgery in patients with hemophilia B and antibodies. Blood 1981; 58:38-44. 2. Nilsson IM, Bern<strong>to</strong>rp E, Zettervall O. Induction of split <strong>to</strong>lerance and clinical cure in high-responding hemophiliacs with fac<strong>to</strong>r IX antibodies. Proc Natl Acad Sci USA 1986; 83:9169-73. 3. Nilsson IM, Bern<strong>to</strong>rp E, Zettervall O. Induction of immune <strong>to</strong>lerance in patients with hemophilia and antibodies <strong>to</strong> fac<strong>to</strong>r VIII by combined treatment with intrave<strong>no</strong>us IgG, cyclophosphamide, and fac<strong>to</strong>r VIII. N Engl J Med 1988; 318:947-50. 4. Freiburghaus C, Bern<strong>to</strong>rp E, Ekman M, Gunnarsson M, Kjellberg BM, Nilsson IM. Immu<strong>no</strong>adsorption for removal of inhibi<strong>to</strong>rs: update on treatment in Malmö- Lund between 1980 and 1995. Haemophilia 1998; 4: 16-20. 5. Warrier I. Management of haemophilia B patients with inhibi<strong>to</strong>rs and anaphylaxis. Haemophilia 1998; 4: 574-6. DISCUSSION 6 The Malmö Pro<strong>to</strong>col Update Bern<strong>to</strong>rp E (Malmö, Sweden) DI MICHELE: I would like <strong>to</strong> make a comment and ask a question with respect <strong>to</strong> the hemophilia B data. If you look at your success rates and the relapse in six months, I’m <strong>no</strong>t convinced that you shouldn’t consider it five successes out of nine patients. What is more important is that if you count up the number of courses of treatment that they were required <strong>to</strong> achieve those successes, what you really have are seven successful courses out of a <strong>to</strong>tal of thirteen. Most of us were presenting success in terms of immune <strong>to</strong>lerance perceived success in terms of a single course of therapy. You have multiple courses here. BERNTORP: In a few patients we gave multiple courses. It is very important <strong>to</strong> look at the eco<strong>no</strong>mic aspects here. We have always stressed that these courses sometimes have <strong>to</strong> be repeated. There is a big difference between a median of twelve months immune <strong>to</strong>lerance induction <strong>Haema<strong>to</strong>logica</strong> vol. <strong>85</strong>(<strong>supplement</strong> <strong>to</strong> n. <strong>10</strong>):Oc<strong>to</strong>ber <strong>2000</strong>