The Importance of Lingualized Occlusion - JDT Unbound
The Importance of Lingualized Occlusion - JDT Unbound
The Importance of Lingualized Occlusion - JDT Unbound
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
1/2 point CDT<br />
documented<br />
scientific credit.<br />
See Page 24.<br />
<strong>The</strong> <strong>Importance</strong> <strong>of</strong><br />
<strong>Lingualized</strong> <strong>Occlusion</strong><br />
By T.G. Hornischer, CDT<br />
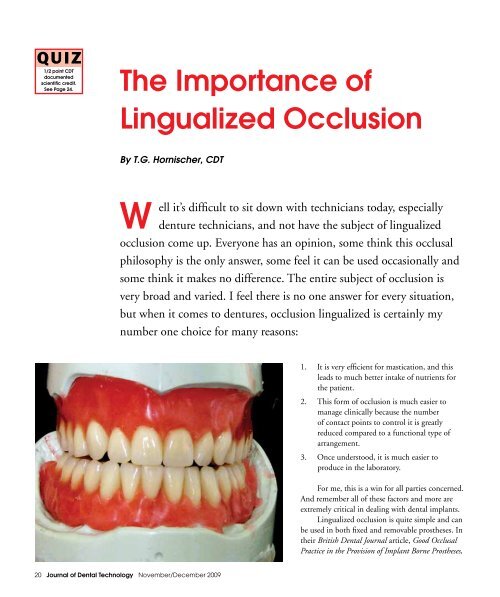
ell it’s difficult to sit down with technicians today, especially<br />
denture technicians, and not have the subject <strong>of</strong> lingualized<br />
occlusion come up. Everyone has an opinion, some think this occlusal<br />
philosophy is the only answer, some feel it can be used occasionally and<br />
some think it makes no difference. <strong>The</strong> entire subject <strong>of</strong> occlusion is<br />
very broad and varied. I feel there is no one answer for every situation,<br />
but when it comes to dentures, occlusion lingualized is certainly my<br />
number one choice for many reasons:<br />
1. It is very efficient for mastication, and this<br />
leads to much better intake <strong>of</strong> nutrients for<br />
the patient.<br />
2. This form <strong>of</strong> occlusion is much easier to<br />
manage clinically because the number<br />
<strong>of</strong> contact points to control it is greatly<br />
reduced compared to a functional type <strong>of</strong><br />
arrangement.<br />
3. Once understood, it is much easier to<br />
produce in the laboratory.<br />
For me, this is a win for all parties concerned.<br />
And remember all <strong>of</strong> these factors and more are<br />
extremely critical in dealing with dental implants.<br />
<strong>Lingualized</strong> occlusion is quite simple and can<br />
be used in both fixed and removable prostheses. In<br />
their British Dental Journal article, Good Occlusal<br />
Practice in the Provision <strong>of</strong> Implant Borne Prostheses,<br />
20 Journal <strong>of</strong> Dental Technology November/December 2009
authors S.J. Davies, R.J.M. Gray and M.P.J. Young<br />
write <strong>of</strong> lingualized occlusion:<br />
“<strong>The</strong> key feature is the arrangement <strong>of</strong> the<br />
posterior teeth so that only the maxillary palatal<br />
cusps (hence: ‘lingualized’ occlusion; or should it<br />
have been called ‘palatalised’ occlusion) occlude<br />
with shallow mandibular central fossae. <strong>The</strong>re is<br />
no contact between the mandibular buccal cusp<br />
and palatal maxillary cusps which might result<br />
in a inclined (non-axial) contact. Laboratory<br />
fabrication time is reduced and this scheme<br />
represents a posterior occlusion that can be more<br />
readily observed in both the laboratory and clinical<br />
environments thereby enabling any unfavorable<br />
occlusal contacts to be identified and corrected<br />
more easily.”<br />
This type <strong>of</strong> occlusal philosophy has been<br />
advocated for quite some time. Many <strong>of</strong> the great<br />
dental giants (Gerber, Pound, Frush, Trubyfield,<br />
Massad and others) have advocated this type <strong>of</strong><br />
denture occlusion. It is interesting when you<br />
study the writings <strong>of</strong> these dentists that the<br />
arrangement <strong>of</strong> the occlusion is only a part <strong>of</strong> the<br />
whole treatment, most <strong>of</strong> the steps leading to the<br />
posterior set are concerned with proper occlusal<br />
registration and positioning <strong>of</strong> the anterior teeth,<br />
lip support, incisal edge position, phonics and arc<br />
<strong>of</strong> closure. All <strong>of</strong> these things must be addressed<br />
well before we can determine how and where the<br />
posterior teeth are set. Despite all the time we,<br />
as technicians, spend setting articulation, setting<br />
teeth, waxing the gingival contours, processing and<br />
polishing, it is all in vain without the foundation<br />
<strong>of</strong> proper occlusal records and precise models. In<br />
most cases without proper occlusal records and<br />
precise models, the restoration will be ground<br />
endlessly by the dentist or not worn by the patient.<br />
This article will mainly focus on a simple<br />
lingualized set up and will touch on the anterior<br />
function leading up to it. This certainly is not an<br />
exhaustive study but simply the basics.<br />
OK let’s begin.<br />
At all possible costs, try and use a semiadjustable<br />
articulator and hopefully with a face<br />
bow, these are inexpensive today. <strong>The</strong> Whip Mix<br />
Ulti-Mate (Figure 1) is a good example <strong>of</strong> this<br />
type <strong>of</strong> articulator. Even without the face bow, if<br />
properly mounted, this type <strong>of</strong> articulator will be<br />
much better than the old hinge type as you can<br />
Figure 2<br />
Figure 1<br />
Figure 3<br />
Figure 4<br />
November/December 2009 Journal <strong>of</strong> Dental Technology 21
Figure 5<br />
Figure 7<br />
Figure 6<br />
Occlusal plane is the line between<br />
the incisal edge position and the<br />
middle <strong>of</strong> the retromolar pad.<br />
set the models more in a proper relationship to<br />
the TMJ. In Figure 2 we set the maxillary anterior<br />
according to the approved or contoured wax rim.<br />
Figures 3 and 4 demonstrate the appropriate<br />
inscial edge and facial contour as dictated by the<br />
established rim. Also, note that the teeth are placed<br />
in a more natural arrangement and not perfectly<br />
straight so that we do not get the denture look.<br />
Figures 5 and 6 illustrate the relationship <strong>of</strong> the<br />
maxillary incisal edge position to help determine<br />
the occlusal plane.<br />
At this point some technicians will complete<br />
the maxillary set up, which is my choice, or set the<br />
mandibular anteriors followed by the mandibular<br />
posteriors. Either way works, as long as the<br />
principals are followed. Figure 7 shows the facial<br />
view <strong>of</strong> the lower set up, while Figure 8 illustrates<br />
again the natural appearance arrangement. One<br />
Figure 9<br />
Figure 10<br />
Figure 8<br />
22 Journal <strong>of</strong> Dental Technology November/December 2009
thing to remember is that function is king, so<br />
following the guidance <strong>of</strong> the TMJ we can set<br />
the anterior teeth in functional harmony and<br />
natural esthetics at the same time. In Figure 9,<br />
the facial appears very natural, the placement <strong>of</strong><br />
the teeth does not look as different as in previous<br />
figures. And, in Figures 10 and 11 you can see the<br />
function in lateral excursion and protrusive are<br />
quite functional. We have a nice balance in lateral<br />
from central, lateral and cuspid. In protrusive we<br />
have nice balance again with the upper and lower<br />
anteriors. So, with function we also have esthetics!<br />
Now, to the mechanics <strong>of</strong> lingualized<br />
occlusion. Figure 12 illustrates the mandibular<br />
posteriors set. <strong>The</strong> thing to note here is the curve<br />
<strong>of</strong> Spee originating from the incisal edge <strong>of</strong> the<br />
cuspid to two-thirds the height <strong>of</strong> the retro-molar<br />
pad, our occlusal plane. This is very important for<br />
the correct function in our lingualized posterior<br />
set up. Now, before we set our maxillary posteriors<br />
let’s look at the contacts we need. Figures 13A<br />
and 13B illustrate the upper and lower contact<br />
points. On the upper, there are contacts only on<br />
the lingual cusp tips. On the lower, the contact<br />
points are in the central groove. It is important<br />
that we must not have any balancing contacts on<br />
the upper posteriors in lateral movements. As you<br />
can see from a side view there is no buccal contact<br />
in centric occlusion (Figure 14) and the case<br />
looks very natural from the facial (Figure 15). Also<br />
important to note, is that the anterior function<br />
Figure 12<br />
Figure 14<br />
Figures 13A<br />
and 13B<br />
Figure 11<br />
Figure 15<br />
November/December 2009 Journal <strong>of</strong> Dental Technology 23
Figure 16<br />
facilitates the disclusion <strong>of</strong> the buccal cusps (Figure<br />
16).<br />
Reviewing this case occlusally (Figures 17 and<br />
18), note the tooth rotations in the anterior and<br />
how they function very nicely while being esthetic.<br />
Figure 19 shows the facial view <strong>of</strong> the completed<br />
case. All that is left now is a nice processing job<br />
and you will have a wonderful result.<br />
I hope that I have shed a bit <strong>of</strong> light on the<br />
concept <strong>of</strong> lingualized occlusion, although this<br />
barely uncovers all that this great concept can be.<br />
Remember that proper jaw relations are essential<br />
to a successful case and that beauty and function<br />
can go hand in hand. We are very fortunate today<br />
to have manufacturers producing teeth specifically<br />
for this purpose. In the not too distant past we<br />
technicians had to adjust the occlusals <strong>of</strong> posterior<br />
teeth to achieve this occlusal scheme, luckily this is<br />
no longer true.<br />
My suggestion to anyone who wishes to add<br />
lingualized occlusion to your repertoire is to attend<br />
hands-on training and market your newly-learned<br />
skills. One can never know too much or be too<br />
successful!<br />
Figure17 Figure 18<br />
Figure 19<br />
Author’s Note:<br />
I would like to give special thanks to<br />
Candulor USA and to Vident for their support and<br />
contribution to this article.<br />
About the Author:<br />
Hornischer is the<br />
recipient <strong>of</strong> the NADL’s<br />
2006 Excellence in<br />
Education Award. He is the<br />
general manager <strong>of</strong> Centric<br />
Dental Laboratory, CDL,<br />
a 25-person, full-service<br />
laboratory in Bullard, Texas.<br />
QUIZ:<br />
Receive .5 point documented scientific credit for passing a quiz about this article. To get the quiz go to <strong>JDT</strong> <strong>Unbound</strong><br />
(www.nadl.org/jdtunbound) and click on the CDT link or use the Fax-On-Demand system by calling (877) 355-8029,<br />
press 1 for NBC documents and enter document number 61 to have the quiz faxed to you. You can enter your<br />
answers to this quiz (course code #19358 at http://quizzes.nadl.org or fax the completed quiz to (850) 222-0053. This<br />
quiz is provided to test the technician’s comprehension <strong>of</strong> the article’s content and does not necessarily serve as an<br />
endorsement <strong>of</strong> the content by NADL or NBC.<br />
24 Journal <strong>of</strong> Dental Technology November/December 2009