Commissioning policy for exceptional treatment requests - National ...
Commissioning policy for exceptional treatment requests - National ...
Commissioning policy for exceptional treatment requests - National ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>Commissioning</strong> Policy<br />
<strong>for</strong><br />
Exceptional Treatment Requests<br />
A <strong>policy</strong> <strong>for</strong> unlicensed and/or unapproved drugs and<br />
therapeutic interventions to support clinical care outside<br />
current Service Level Agreements<br />
February 2008<br />
Document Reference Number<br />
Version 1.20 – February 2008 – db<br />
Previous Document Number<br />
Version 1.19 – February 2007 – nb<br />
Author‟s Name<br />
Alan Marsh/Nickie Burgess/Denise Bell<br />
Author‟s Job Title<br />
Head of Contracting/Contracts Manager/IFR Manager<br />
Department/Service/Directorate<br />
Contracts Department<br />
Document Status<br />
Re-draft<br />
Issue Date/Publication Date April 2008<br />
Initial Review Date September 2007<br />
Full Review Date April 2009<br />
Distribution<br />
All GP Practices<br />
All PBC Cluster Chairs<br />
Professional Executive Team<br />
Local Acute Providers<br />
Patient Advice & Liaison Service (PALS)<br />
Committee Ratifying Policy<br />
Date of Approval<br />
Professional Executive Committee (PEC)<br />
20 February 2008<br />
Committee Ratifying Policy<br />
Date of Approval<br />
Dudley PCT Trust Board<br />
20 February 2008<br />
Page 1 of 35
Contents<br />
<strong>Commissioning</strong> Policy <strong>for</strong> Exceptional Treatment Requests<br />
1 Executive Summary ................................................................................................................... 3<br />
2 Introduction ................................................................................................................................ 3<br />
3 The Scope of this Policy ............................................................................................................ 5<br />
4 The Referral Process to make an Exceptional Treatment Request (ETR)................................. 5<br />
5 Ethical Framework ................................................................................................................... 12<br />
6 The Legal Framework .............................................................................................................. 13<br />
7 The <strong>National</strong> Context ............................................................................................................... 14<br />
8 Research ................................................................................................................................. 16<br />
9 Decision Process <strong>for</strong> unlicensed or unproven Drug and Therapeutic Interventions ................. 17<br />
10 Managing the entry of new drugs ............................................................................................ 17<br />
11 Co-Funding ............................................................................................................................ 18<br />
12 Policy review .......................................................................................................................... 18<br />
13 Distribution ............................................................................................................................. 18<br />
14 Reference Documents ........................................................................................................... 18<br />
Appendix 1- Membership of ETAP ............................................................................................. 19<br />
Appendix 2 – ETR Pro-<strong>for</strong>ma ....................................................................................................... 20<br />
Appendix 3- Appeals Procedure ................................................................................................. 24<br />
Appendix 4- Digital Recording of Appeals Procedure ................................................................. 28<br />
Appendix 5 – Business Case Guidance ....................................................................................... 29<br />
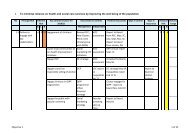
Appendix 6 – Process of Managing Exceptional Treatment Requests ........................................ 33<br />
Appendix 7 – ETR Decision Report ............................................................................................ 34<br />
Appendix 8 – Abbreviations ......................................................................................................... 35<br />
Page 2 of 35
<strong>Commissioning</strong> Policy <strong>for</strong> Exceptional Treatment Requests<br />
1. Executive Summary<br />
This <strong>policy</strong> covers the Primary Care Trust‟s (PCTs) decision making process <strong>for</strong> the commissioning<br />
of interventions/<strong>treatment</strong>s that fall outside of current commissioning contracts. The <strong>policy</strong> includes<br />
the legal and national framework <strong>for</strong> such decisions.<br />
All applications <strong>for</strong> Exceptional Treatment Request (ETR) funding are required to make a <strong>for</strong>mal<br />
case outlining the rationale <strong>for</strong> the intervention/<strong>treatment</strong>, appropriate monitoring and the potential<br />
benefits to the individual and the health economy and include details of the overall costs involved.<br />
When considering an ETR the following points are taken into account:<br />
* Available evidence on the effectiveness and safety of the intervention <strong>for</strong> the patient.<br />
* The potential <strong>for</strong> a precedent to be set with regard to the future funding of the<br />
intervention/<strong>treatment</strong>.<br />
* Agreeing funding in isolation may distort clinical and commissioning priorities.<br />
* Funding may subject the PCT to unplanned financial risk.<br />
* The existence of any research programmes, that may lead to benefits <strong>for</strong> other patients<br />
This <strong>policy</strong> does not cover new developments which clinicians wish to provide on a regular basis.<br />
Funding <strong>for</strong> these must be requested through the Local Development Plan (LDP) process.<br />
2. Introduction<br />
2.1 The role and responsibilities of Dudley PCT in commissioning healthcare services<br />
This is a <strong>policy</strong> regarding the PCTs decision-making process <strong>for</strong> responding to Exceptional<br />
Treatment Requests and the commissioning of drugs, <strong>treatment</strong>s, procedures, investigations, that<br />
fall outside of current commissioning contracts.<br />
It is the statutory duty of the NHS and Primary Care Trusts (PCTs) to provide services to such<br />
extent as it considers necessary to meet all reasonable requirements within the resources<br />
available. “A national health service will always need to operate within the resources<br />
available. It is in no one‟s interest locally to „break the bank”. (Source: The NHS in England:<br />
the operating framework <strong>for</strong> 2006/07- Annex C Demand Management in 2006/07) This includes<br />
the responsibility to make decisions on the commissioning of healthcare services that do not fall<br />
under existing contracts or are unlicensed or not approved by the <strong>National</strong> Institute <strong>for</strong> Health and<br />
Clinical Excellence (NICE) and ensuring that all decisions are made in the interest of the whole<br />
population of Dudley within the resources available. The PCT owes this duty to patients registered<br />
with a Dudley PCT GP or to unregistered patients resident within its geographical boundary.<br />
Each year the PCT receives a number of <strong>requests</strong> <strong>for</strong> <strong>treatment</strong>s not covered by a Service Level<br />
Agreement or other Contract. This <strong>policy</strong> sets out the PCT processes <strong>for</strong> managing those<br />
<strong>requests</strong>. Throughout this document these <strong>requests</strong> will be known as Exceptional Treatment<br />
Requests or ETRs.<br />
Page 3 of 35
<strong>Commissioning</strong> Policy <strong>for</strong> Exceptional Treatment Requests<br />
Inevitably there will be occasions when it is both reasonable and legitimate <strong>for</strong> the PCT to restrict or<br />
not commission a particular healthcare intervention. In such circumstances, it is important that the<br />
process by which the PCT came to that decision is open and explicit. This <strong>policy</strong> document sets<br />
out that process and defines the framework within which such commissioning decisions are made.<br />
2.2 Policy Statement<br />
This <strong>policy</strong> covers the decision making process <strong>for</strong> ETRs including <strong>requests</strong> to fund the use of<br />
unlicensed and/or unapproved drugs and therapies. The <strong>policy</strong> does not cover <strong>requests</strong> <strong>for</strong> GPs to<br />
prescribe an FP10 (primary care prescription) – such <strong>requests</strong> must be passed to the PCT<br />
Prescribing Committee. There is a register associated with this <strong>policy</strong> which documents associated<br />
policies used <strong>for</strong> decision making regarding drugs, <strong>treatment</strong>s or interventions where a<br />
<strong>policy</strong>/procedure is in place <strong>for</strong> decision making with regard to a particular drug, <strong>treatment</strong> or<br />
intervention. This Register is available from the ETR Manager.<br />
The implications <strong>for</strong> the commissioner are:<br />
There is pressure on the Primary Care Trust (PCT) to fund a drug or intervention prior to the<br />
availability of significant evidence on the effectiveness and safety of the drug/intervention.<br />
PCTs require time to consider other aspects of the drug or intervention including cost<br />
effectiveness and priority rating.<br />
There is potential <strong>for</strong> a precedent to be set with regard to the future funding of the<br />
intervention, regardless of its cost-effectiveness and the priority it has in relation to other<br />
services.<br />
Agreeing the funding of a drug or therapy in isolation has the danger of distorting clinical and<br />
commissioning priorities.<br />
It may subject the PCT to unplanned financial risk.<br />
The PCT will not support the prescribing of unlicensed or unapproved drug/interventions or<br />
<strong>treatment</strong> unless there are fully assessed clinical and psychological circumstances that indicate<br />
significant benefit to the patient by the use of the <strong>treatment</strong>/intervention and there is sufficient<br />
resources within the PCT available to fund the <strong>treatment</strong> without jeopardizing funding to support<br />
currently commissioned or Local Delivery Plan (LDP) funded technologies, all of which need to be<br />
agreed in advance.<br />
The PCT will not be responsible <strong>for</strong> funding unlicensed or unapproved drugs that have been<br />
prescribed without prior approval.<br />
The PCT reserve the right to review the evidence of the safety, efficacy and cost efficiency of a<br />
drug or therapy prior to funding within a reasonable time period.<br />
New therapies, technologies, drugs or new indications <strong>for</strong> established drugs should be seen in the<br />
same light as any service development and Trusts or others making applications <strong>for</strong> funding are<br />
required to produce a <strong>for</strong>mal case <strong>for</strong> funding.<br />
Page 4 of 35
<strong>Commissioning</strong> Policy <strong>for</strong> Exceptional Treatment Requests<br />
Patient care that will be advised/used <strong>for</strong> <strong>treatment</strong> across multiple patients must not be processed<br />
through the ETR route and a <strong>for</strong>mal business case must be made to the Director of Patient<br />
Experience & Service Improvement. Submitted business cases should be endorsed by the Provider<br />
Organisation at a corporate level prior to their submission. This will ensure appropriate <strong>treatment</strong>s<br />
are fully evaluated and financed within contract, if necessary as an in-year decision through the<br />
Contract Variation process or annually through the LDP process. (See Appendix 5).<br />
3. The Scope of this Policy<br />
The PCT must ensure that it provides the community of Dudley with the best health care from the<br />
funds available. This includes the responsibility to make decisions <strong>for</strong> funding <strong>requests</strong> that do not<br />
fall under existing contracts which includes unlicensed or unproven therapeutic interventions and<br />
unusual or novel <strong>treatment</strong>s and ensuring that decisions made are in the interest of the whole<br />
Dudley population. An Exceptional Treatment Approval Panel (ETAP) has been established to<br />
consider these <strong>requests</strong> in the PCT. A list of the members of this group is available at Appendix 1.<br />
The purpose of this <strong>policy</strong> is to:<br />
Clarify the decision making process <strong>for</strong> dealing with ETRs and the responsibility <strong>for</strong><br />
taking those decisions.<br />
Provide a framework appropriate <strong>for</strong> the handling of <strong>exceptional</strong> cases.<br />
Ensure consistency between decisions on <strong>exceptional</strong> cases.<br />
Ensure limited resources are used to best effect.<br />
Provide clear criteria against which <strong>requests</strong> and any appeal can be judged.<br />
Set out the appeals process in the event that an initial request is refused.<br />
4. The Referral Process to make an Exceptional Treatment Request<br />
(ETR)<br />
The first stage of the process is <strong>for</strong> an ETR Pro-<strong>for</strong>ma (Appendix 2) to be completed by a GP,<br />
Consultant or a person involved in the clinical care of the patient to be sent to the Contracts<br />
Department at the PCT <strong>for</strong> a decision.<br />
In<strong>for</strong>mation required on the <strong>for</strong>m includes the following:<br />
Name of clinician making application.<br />
Patients name, address and date of birth.<br />
Patient‟s GP and Practice Address.<br />
Level of urgency.<br />
Brief health history including previous <strong>treatment</strong> <strong>for</strong> relevant indication.<br />
Treatment/intervention requested.<br />
Cost effectiveness, where possible include data from economic evaluations with a list of<br />
references.<br />
In<strong>for</strong>mation on alternative <strong>treatment</strong> available.<br />
Proposed provider of <strong>treatment</strong>.<br />
Costings and length of <strong>treatment</strong>.<br />
Page 5 of 35
<strong>Commissioning</strong> Policy <strong>for</strong> Exceptional Treatment Requests<br />
Evidence <strong>for</strong> improvement on health, including data from clinical trials or relevant guidance<br />
and patient monitoring arrangements.<br />
Implications <strong>for</strong> patient if not funded.<br />
Any patient <strong>exceptional</strong> applicable circumstances and a summary of what in<strong>for</strong>mation has<br />
been provided to the patient about the proposed <strong>treatment</strong>.<br />
Summary of NICE recommendations if this is an application to fund an interventional<br />
procedure.<br />
Rationale <strong>for</strong> bringing this case to the ETAP.<br />
Monitor and evaluate effectiveness/duration of reporting back to the PCT.<br />
Patient has been in<strong>for</strong>med of request.<br />
Benefits to the patient as a result of receiving <strong>treatment</strong>.<br />
Patient in<strong>for</strong>med of risks associated with <strong>treatment</strong>.<br />
Treatment/process fully explained to the patient.<br />
Additional in<strong>for</strong>mation submitted by the patient.<br />
The referring clinician is expected to advise the patient that they can submit comments to the panel<br />
<strong>for</strong> consideration in the decision making process. The patients comments should be <strong>for</strong>warded with<br />
the pro-<strong>for</strong>ma. The pro-<strong>for</strong>ma will ensure that the PCT receives the correct in<strong>for</strong>mation needed to<br />
make a decision as quickly as possible.<br />
This <strong>for</strong>m is to be used <strong>for</strong> equipment, drugs and <strong>treatment</strong>s outside of existing contracts including<br />
un-licensed or unapproved therapeutic interventions. Completed <strong>for</strong>ms should be sent to:<br />
Exceptional Treatment Requests Manager<br />
Contracts Department<br />
Dudley PCT<br />
St John‟s House<br />
Union Street<br />
Dudley<br />
DY2 8PP<br />
Fax: 01384 366497 (Safe haven fax rules apply)<br />
Email: ETR@dudley.nhs.uk<br />
When the ETR Pro-<strong>for</strong>ma is received by the Contracts Department at the PCT it will be logged to<br />
keep track of its progress and acknowledged by email within 3 working days confirming receipt to<br />
the referring clinician/contracts manager.<br />
Each request will be reviewed by 1 member of the Contracts and/or <strong>Commissioning</strong> Departments,<br />
with input from the Public Health Department when necessary to ensure its completion in line with<br />
this <strong>policy</strong> and to ensure that any related <strong>policy</strong> and relevant criteria are met and that the request is<br />
not funded by any national or local specialised commissioning arrangements. In instances where<br />
not all referral criteria are met and no <strong>exceptional</strong> circumstances have been identified, the request<br />
<strong>for</strong> funding will not be presented to ETAP <strong>for</strong> a decision and the patient, the GP and the referrer will<br />
be sent a <strong>for</strong>mal refusal of funding letter. There is no right of appeal against a PCT <strong>Commissioning</strong><br />
Policy within this process. Should the patient/referring clinician wish to challenge a PCT<br />
<strong>Commissioning</strong> <strong>policy</strong>, this should be addressed in writing to the Director of Patient Experience &<br />
Service Improvement in the first instance. Comments received from patients and referring<br />
clinicians will be considered when the <strong>policy</strong> is <strong>for</strong>mally reviewed.<br />
Page 6 of 35
<strong>Commissioning</strong> Policy <strong>for</strong> Exceptional Treatment Requests<br />
Where it is the case that the ETR provided by the referrer meets referral criteria, funding will<br />
automatically be approved without sending <strong>for</strong> additional in<strong>for</strong>mation from the patient or<br />
presentation to the ETAP. Requests that do not fall into either category will be <strong>for</strong>warded to the<br />
ETAP <strong>for</strong> consideration.<br />
A flow diagram showing the process of managing ETRs is available at Appendix 6. A register of<br />
associated policies is available by contacting the ETR Manager.<br />
4.1 The Decision Making Process<br />
4.2 The Exceptional Treatment Approval Panel (ETAP)<br />
The ETAP routinely meet once per month in order to make decisions on <strong>requests</strong> received. At each<br />
meeting the ETAP will receive anonymised referral in<strong>for</strong>mation and any copies of additional<br />
correspondence which may be relevant to the decision making process. A member of the Public<br />
Health Department and a member of the Contracts Department will ensure the ETAP receive and<br />
consider a briefing of the evidence concerning the requested <strong>treatment</strong>. When considering whether<br />
to support the request the ETAP will take the following into consideration:<br />
Details of evidence and decisions already considered by the PCT/ other PCTs and any<br />
relevant associated PCT <strong>policy</strong>.<br />
The nature of the proposed <strong>treatment</strong>.<br />
The individual needs of the patient, the case advanced by the clinician and the view of the<br />
GP (where the GPs view is provided and the referring clinician is not the GP).<br />
The seriousness of the illness/condition and availability of alternative <strong>treatment</strong> and relative<br />
evidence of the cost and clinical effectiveness and associated risks of such <strong>treatment</strong>. All<br />
<strong>treatment</strong>s/Interventions need to provide clear evidence of effectiveness * and value <strong>for</strong><br />
money. There must be evidence of the efficacy and safety of the <strong>treatment</strong>/intervention<br />
requested within the ETR, including relevant clinical trials and their outcomes, NICE<br />
Guidance, DoH Guidance or any other relevant guidance, if available and noted if the<br />
<strong>treatment</strong> has Medicines and Healthcare products Regulatory Agency (MHRA) approval.<br />
In<strong>for</strong>mation from specialist clinical network will be sought if required.<br />
The ETAP considers any evidence pertaining to the level of cost – effectiveness of the<br />
<strong>treatment</strong> and risk, it also considers cost benefit analysis to the population of Dudley <strong>for</strong><br />
whom the PCT serves, taking into account the PCT‟s financial position on agreed local<br />
priorities as outlined in the Local Delivery Plans (LDP) and other applications <strong>for</strong> <strong>exceptional</strong><br />
<strong>treatment</strong>.<br />
Regard will also be had to the available budget within the PCT and whether the case is likely<br />
to create a precedent which may commit the PCT to funding similar cases. In these<br />
circumstances the likely financial exposure <strong>for</strong> the PCT together with any opportunity costs<br />
in terms of competing priorities <strong>for</strong> funding will be considered.<br />
The willingness of the patient in the future to co-operate in having their condition regularly<br />
assessed to determine whether the <strong>treatment</strong> is effective and thus whether it should be<br />
continued.<br />
* This is defined as good quality observational control or case control studies or better i.e. controlled trials. This is<br />
based on the levels recommended by NICE.<br />
Page 7 of 35
<strong>Commissioning</strong> Policy <strong>for</strong> Exceptional Treatment Requests<br />
In Summary, the following factors will be considered:<br />
• Does the patient meet PCT referral criteria<br />
• Nature of proposed <strong>treatment</strong>/intervention and its clinical effectiveness<br />
• Analysis of alternative <strong>treatment</strong> and its cost effectiveness/value <strong>for</strong> money<br />
• Long term benefits/cost analysis<br />
• Patient <strong>exceptional</strong> circumstances<br />
• Number of people in Dudley that may be affected by the decision.<br />
• Precedent setting.<br />
The decision of the ETAP will be documented as identified at Appendix 7. Thereafter the decision<br />
will be communicated directly to the patient, the patients own GP and the referrer.<br />
In fulfilling the primary purpose of the ETAP meeting, the ETAP will ensure it has adequate<br />
supporting in<strong>for</strong>mation upon which to base its decision. In the absence of such in<strong>for</strong>mation,<br />
decisions will be deferred until supplementary in<strong>for</strong>mation is available to the ETAP.<br />
There will be a written response to the referrer within 10 working days or as soon as practicable<br />
after the ETAP taking place giving the outcome or feedback on the progress of the request.<br />
4.2.1 Exceptionality<br />
There can be no exhaustive definition of the conditions which may potentially come within the<br />
definition of an <strong>exceptional</strong> case. The word “exception” means “a person, thing or case to which<br />
the general rule is not applicable”. The following criteria, however, are indicative of the presence or<br />
absence of <strong>exceptional</strong>ity in the present context:<br />
To be an exception, there must be unusual or unique clinical factors about the patient that<br />
suggest that he or she is:<br />
I. Significantly different from the wider group of patients with the same condition; or<br />
II. Likely to gain significantly more benefit from the intervention than might be expected<br />
from the average patient with the same condition.<br />
The fact that a <strong>treatment</strong> is likely to be effective <strong>for</strong> a patient is not, in itself, a sufficient basis <strong>for</strong><br />
establishing an exception.<br />
If a patient‟s clinical condition matches the „accepted indications‟ <strong>for</strong> a <strong>treatment</strong>, but the<br />
<strong>treatment</strong> is not funded, then the patient‟s circumstances are not, by definition, <strong>exceptional</strong>.<br />
It is <strong>for</strong> the requesting clinician (or patient) to make the case <strong>for</strong> <strong>exceptional</strong> circumstances.<br />
Social value judgments are rarely relevant to the consideration of <strong>exceptional</strong> status.<br />
Page 8 of 35
4.3 Scheme of Delegation<br />
<strong>Commissioning</strong> Policy <strong>for</strong> Exceptional Treatment Requests<br />
The ETAP acts as a <strong>for</strong>mal sub-committee of the PCT Professional Executive Team (PEC) and has<br />
the authority to commit financial resources within the frameworks agreed. The ETAP will report a<br />
summary of the outcomes of its decisions to the PCT PEC meetings on an annual basis. On<br />
occasion ETAP may request PEC to input into the decision making process, in this case the<br />
request will be referred directly to the next PEC <strong>for</strong> their input. PEC may be asked <strong>for</strong> their input<br />
when there are significant financial or political implications or where a wider issue than the<br />
Exceptional Treatment Request is identified.<br />
The ETAP will be quorate when there is a minimum of 5 in attendance or involved in the decision<br />
making. These 5 persons should include the Chairperson (who will be the Director of Patient<br />
Experience and Service Improvement or their nominated deputy, a representative from Public<br />
Health from the PCT, 2 Clinical representatives, one of which must be a Dudley GP and a lay<br />
representative or Non-Executive Director. However, in the event of an even number in attendance<br />
at ETAP the Chair will abstain from the vote.<br />
4.4 In<strong>for</strong>ming Referrers of Decisions – Correspondence Standards<br />
Referrers will be sent an acknowledgement letter within 3 working days after receipt of an<br />
Exceptional request <strong>for</strong> funding. After the referral has been considered by the ETAP the final<br />
decision will be sent in writing to the referrer within 10 working days after the ETAP meeting at<br />
which the case has been presented. The decision of the ETAP will be communicated directly to<br />
the referrer, the patient and the patient‟s own GP. The right to appeal the process within 25 days of<br />
receipt of the decision letter will be communicated where a decision has been made not to fund a<br />
request. The ETAP will not enter into direct patient correspondence other than to communicate on<br />
matters of process, in<strong>for</strong>mation clarification and <strong>policy</strong> matters.<br />
4.5 What decision will be made<br />
There are 5 different decisions possible <strong>for</strong> an Exceptional case when presented to the ETAP.<br />
1. Agree to fund/support the request<br />
2. Defer decision pending further in<strong>for</strong>mation/investigation<br />
3. Refuse to support/fund the request<br />
4. Identify a Service Development which will be referred on to the appropriate PCT<br />
<strong>Commissioning</strong>/LDP group or HENIG if appropriate and in<strong>for</strong>m referrer. (See Section 9)<br />
5. Refer to PEC <strong>for</strong> input.<br />
4.6 Requirement <strong>for</strong> Urgent Decisions<br />
It is recognised that on occasions emergency and urgent decisions will be required. In such<br />
circumstances referring parties are encouraged to liaise with their patients and with their agreement<br />
include details of <strong>exceptional</strong> circumstances with the referral or encourage patients to send this<br />
in<strong>for</strong>mation to the PCT without delay. Given the need <strong>for</strong> expediency the ETAP will make the<br />
decision based on the in<strong>for</strong>mation put be<strong>for</strong>e it in such circumstances.<br />
Page 9 of 35
<strong>Commissioning</strong> Policy <strong>for</strong> Exceptional Treatment Requests<br />
In <strong>exceptional</strong>ly clinically urgent situations the ETAP will operate virtually e.g. using<br />
email/telephone to reach speedy decisions if it is necessary. It is important that no member of the<br />
group make decisions on their own. It is recommended that the decision is taken by the<br />
Chairperson of the ETAP (or nominated Deputy Chairperson), 1 GP and a representative from<br />
Public Health (3 members as a minimum). The decision will be recorded by the ETR Manager (or<br />
nominated representative) following discussion with panel members. The final decision will be<br />
reported to the panel members of the next scheduled ETAP.<br />
4.7 Appeals<br />
In the event that the patient wishes to appeal against the process the appeals procedure set out in<br />
Appendix 3 needs to be followed.<br />
The Appeals Panel (the Panel) is established as the Panel <strong>for</strong> the PCT Board to consider appeals<br />
by a referring Medical Practitioner and/or their patient against the process followed by the PCT with<br />
regard to an ETR. Where a decision to refuse an ETR is made the patient will be advised of their<br />
right to appeal the process in writing and the process <strong>for</strong> doing so. Where a Medical Practitioner is<br />
appealing on behalf of the patient this needs to be confirmed by patient‟s written consent to the<br />
PCT.<br />
4.8 Initiating the Appeal<br />
The right of appeal is valid <strong>for</strong> a period of 25 days following the date of letter advising that the ETR<br />
has been refused. It is the responsibility of the referring clinician to discuss the appeal process and<br />
implications fully with the patient concerned. A letter from the patient/advocate requesting an<br />
appeal against the decision must be provided to:<br />
Exceptional Treatment Requests Manager<br />
The Contracts Department<br />
Dudley PCT<br />
St Johns House<br />
Dudley<br />
DY2 8PP<br />
Fax No: 01384 366497 (safe haven fax rules apply)<br />
Email: ETR@dudley.nhs.uk<br />
Please note: Should this deadline 25 day deadline be missed a new ETR will be required.<br />
4.9 Role of the Appeals Panel<br />
The Panel‟s role is to consider whether the correct process has been followed to reach a decision.<br />
The appeals panel should ensure that the ETAP have considered the following factors:<br />
• Does the patient meet PCT referral criteria<br />
• Analysis of proposed <strong>treatment</strong><br />
• Analysis of alternative <strong>treatment</strong> and its cost effectiveness/value <strong>for</strong> money<br />
• Precedent setting<br />
• Long term benefits/cost analysis<br />
• Nature of proposed <strong>treatment</strong>/intervention and its clinical effectiveness<br />
• Patient <strong>exceptional</strong> circumstances<br />
• Number of people in Dudley that may be affected by the decision.<br />
Page 10 of 35
<strong>Commissioning</strong> Policy <strong>for</strong> Exceptional Treatment Requests<br />
The Appeals panel does not have the jurisdiction to change/amend PCT <strong>Commissioning</strong> Policies<br />
that have been approved by the PCT Board and will make decisions based on current<br />
<strong>Commissioning</strong> Policies at the time of the Appeals hearing.<br />
Should the referring clinician/patient wish to challenge a PCT <strong>Commissioning</strong> Policy, this will need<br />
to be in writing addressed to the Director of Patient Experience & Service Improvement in the first<br />
instance.<br />
Should the Appeals Panel uphold an appeal, the case must be referred back to the ETAP to be<br />
reconsidered.<br />
4.10 Membership of the Appeal Panel<br />
The Panel shall comprise of a minimum of 5 persons none of whom should have sat on the ETAP<br />
<strong>for</strong> the case under consideration. There shall be at least one Non-Executive Director, one Director<br />
who is not the Chief Executive and who is from the <strong>Commissioning</strong> arm of the PCT (not Provider<br />
Services), this includes Directors of Governance, Human Resources, Public Health and Patient<br />
Experience & Service Improvement), together with at least one GP representative (who must be a<br />
member of the PEC, a Clinical Lead or PBC Cluster Chair), a Public Health representative, a<br />
commissioning representative or a finance representative (this representative must have expertise<br />
in Local Development Plan (LDP) knowledge. The panel will decide prior to the meeting<br />
commencing who will Chair the appeals panel, this would normally be either the Non-Executive<br />
Director or PCT Director. The panel Chairperson may co-opt onto the Panel a Medical Practitioner,<br />
nurse or other healthcare professional with relevant healthcare expertise. The patient will be<br />
entitled to attend the hearing and to make oral representations either personally or by a parent,<br />
guardian, carer or other appropriate advocate.<br />
4.11 Complaints<br />
If a complaint is made about the handling of an appeal, the PCT‟s complaints procedure can be<br />
invoked within 6 months of the date of notification of the decision to the patient by the Appeal Panel<br />
Chairperson. If the complaint relates to the impact of a commissioning <strong>policy</strong> on an individual then<br />
the complaints procedure will only be implemented once the Appeal Panel has reached a final<br />
decision. Please note: A complaints investigation will review the process only and not the decision<br />
made by the Appeals Panel.<br />
4.12 Health Care Commission<br />
Following a complaint, if we have been unable to resolve all concerns, the patient has the right to<br />
ask the Healthcare Commission to review the process. This should be done within 6 months of<br />
receiving the response to the complaint. The Healthcare Commission is an independent body<br />
established to promote improvements in health care through the assessment of the per<strong>for</strong>mance of<br />
those who provide services. Their website address is: www.healthcarecommission.org.uk. You<br />
can contact the Healthcare Commission on 0845 601 3012 or write to them at:<br />
Healthcare Commission<br />
Complaints Team<br />
Peter House<br />
Ox<strong>for</strong>d Street<br />
Manchester M1 5AN<br />
Page 11 of 35
<strong>Commissioning</strong> Policy <strong>for</strong> Exceptional Treatment Requests<br />
4.13 Patient Advice and Liaison Service<br />
The role of PALS is to provide in<strong>for</strong>mation, advice and support to patients, service users, carers<br />
and relatives with concerns or issues about their health service.<br />
PALS liaises with service providers and other outside agencies to resolve patient queries, concerns<br />
and issues and assists services with learning lessons.<br />
5 Ethical Framework<br />
In reaching its decisions, the PCT aims to;<br />
take into account and weigh all the relevant evidence<br />
take into account the opinion of relevant clinicians<br />
give proper consideration to the views of the patient or group of patients involved and accord<br />
proper weight to their needs against other groups competing <strong>for</strong> scarce resources<br />
take into account only material factors<br />
act in the utmost good faith<br />
make a decision that is in every sense reasonable and af<strong>for</strong>dable to the PCT achieving<br />
financial balance<br />
This ethical framework should enable the PCT to make fair and consistent decisions that treat<br />
patients equitably and take full account of the needs of minority ethnic people recognising the<br />
varied requirements of patients and carers whether they are based on gender, culture, age,<br />
disability, race or religion.<br />
A patient‟s health needs will be assessed in relation to their capacity to benefit from a healthcare<br />
intervention, its efficacy, safety and risk cost benefit analysis. In the absence of evidence of health<br />
need, <strong>treatment</strong> will not generally be recommended solely because a patient <strong>requests</strong> it. Similarly,<br />
a <strong>treatment</strong> of potentially very little benefit and not good value <strong>for</strong> money will not be provided<br />
because it is the only <strong>treatment</strong> available. This is necessary to ensure that resources are used to<br />
provide the greatest health benefit <strong>for</strong> all the PCT population and that healthcare provided by the<br />
PCT is reasonable and af<strong>for</strong>dable.<br />
The Ethical Framework is especially concerned with the following:<br />
evidence of clinical and cost effectiveness and the resources available within the health<br />
community<br />
the needs of the patient(s)<br />
needs of the community<br />
5.1 Evidence of clinical and cost effectiveness<br />
In order to assess the potential healthcare benefits of drug therapies, interventions or procedures<br />
the PCT strives to obtain the best evidence of clinical effectiveness and Value For Money (VFM).<br />
Page 12 of 35
<strong>Commissioning</strong> Policy <strong>for</strong> Exceptional Treatment Requests<br />
„Clinical effectiveness‟ can be defined as, „the application of the best knowledge, derived from<br />
research, clinical experience and patient preferences to achieve optimum processes and<br />
outcomes of care <strong>for</strong> patients. The process involves a framework of in<strong>for</strong>ming, changing<br />
and monitoring practice‟ (Source: Promoting Clinical Effectiveness DOH 1996).<br />
Evidence <strong>for</strong> clinical effectiveness will be sought from large-scale randomised clinical trials, but if<br />
these have not been conducted or published, evidence from less authoritative sources will be<br />
considered, including controlled trials, cohort studies and case studies. Patients‟ evidence of<br />
clinical effectiveness will also be considered. When assessing evidence of clinical effectiveness the<br />
outcome measures which will be given greatest importance are those considered important by<br />
patients and clinicians.<br />
The PCT has a statutory obligation not to exceed its budget, the cost of healthcare interventions<br />
will be considered and also the impact of investing in one area of healthcare that will inevitably<br />
divert resources from other uses. The ETAP will compare the cost of <strong>treatment</strong> to its overall<br />
benefit, both to the individual and the community. It will consider technical cost-benefit<br />
calculations.<br />
6 The Legal Framework<br />
It is the statutory duty of the NHS and its PCTs „to provide comprehensive healthcare within the<br />
resources available‟. The Health Act 1999 identifies new section 97D of the NHS Act 1977 which<br />
places a financial duty on the PCT not to spend more than the sum of the amount allotted to them<br />
by their Health Authority (the cash limit). “Regulations 3(7)-(10) of the <strong>National</strong> Health Service<br />
(Functions of Strategic Health Authorities and Primary Care Trusts and Administrations<br />
Arrangements) (England) Regulations 2002 place upon the PCT the statutory duty to provide<br />
services to such extent as it considers necessary and to meet all reasonable requirements.<br />
Further, in making commissioning decisions, the ETAP and the PCT needs to consider the Human<br />
Rights Act (1998), in particular:<br />
Article 2<br />
Article 8<br />
Article 12<br />
Article 14<br />
the right to life<br />
respect <strong>for</strong> private and family life<br />
the right to marry and found a family<br />
prohibition of discrimination<br />
Under the Human Rights Act, a legal challenge regarding the inability of the PCT to<br />
fund/commission a particular <strong>treatment</strong> would focus on whether the decision was linked to (a)<br />
unaf<strong>for</strong>dability, (b) the PCT‟s priorities and (c) how those priorities were decided.<br />
The Rogers v. Swindon PCT appeal decision in April 2006 decided that it was “permissible <strong>for</strong> a<br />
PCT to carry out a cost/benefit analysis when deciding what <strong>treatment</strong> to fund and what to decline<br />
to fund. Given that all PCT‟s have a legal duty to break even, it is arguable that PCTs are obliged<br />
to consider the cost of all <strong>treatment</strong>s be<strong>for</strong>e agreeing to fund them.” Also the case recognised that<br />
PCTs cannot af<strong>for</strong>d to fund all patients who might benefit from all the <strong>treatment</strong>s that could be<br />
prescribed and “this case affirmed that it is permissible to select those patients who could benefit<br />
from a <strong>treatment</strong> using a combination of clinical effectiveness and social grounds. Provided the<br />
PCT accepts up front that cost grounds are relevant, it is lawful to have a <strong>policy</strong> which says that<br />
one patient will get funding because she has disabled dependants or other relevant social<br />
circumstances but another will not” (Source: Mills and Reeve Herceptin Briefing: 18 th April 2006).<br />
Page 13 of 35
<strong>Commissioning</strong> Policy <strong>for</strong> Exceptional Treatment Requests<br />
The PCT will not commit funds to the <strong>treatment</strong> <strong>for</strong> individuals which put other funding decisions<br />
already made through the LDP process at risk without due consideration. Patients with unusual or<br />
rare medical conditions have as much right to medical care as anyone else. Patients, through their<br />
doctor, have the opportunity to have their ETR considered on their own merits and against this PCT<br />
<strong>policy</strong> in each case.<br />
7 The <strong>National</strong> Context<br />
A further responsibility of the PCT is to implement changes in the local NHS in line with the<br />
requirements of the Department of Health. The PCT will do this through strategy <strong>for</strong>mulation,<br />
Service Level Agreement (SLA) review along with per<strong>for</strong>mance management and clinical<br />
governance.<br />
The Government‟s strategic plan <strong>for</strong> the modernisation of the NHS (The NHS Plan, Department of<br />
Health, 2000) states, as a core principle, that, "The NHS will work continuously to improve quality<br />
services and to minimise errors."<br />
“An important means of achieving this is <strong>for</strong> healthcare agencies and professionals to<br />
establish ways to identify procedures that should be modified or abandoned and new<br />
practices that will lead to improved patient care”.<br />
The Government and Department of Health have established „standard-setting‟ organisations as<br />
key drivers <strong>for</strong> their plans <strong>for</strong> service improvement and evidence-based healthcare.<br />
The work of two of these organisations is particularly relevant to this <strong>policy</strong>: the <strong>National</strong> Institute<br />
<strong>for</strong> Health and Clinical Excellence (NICE) and the Healthcare Commission. As identified by the<br />
Department of Health, by waiting to fund new drugs and interventions following NICE approval this<br />
process would “balance the need <strong>for</strong> speed with the need to ensure that all the evidence is looked<br />
at thoroughly and the guidance produced is authoritative” so that “patients can get access to<br />
clinically and cost-effective <strong>treatment</strong>s”. This national guidance was the government‟s action<br />
toward ending postcode prescribing and promoted as “providing national standards <strong>for</strong> a national<br />
health service. It makes sense <strong>for</strong> a national body to tackle these difficult decisions to avoid each<br />
health authority duplicating the process of what they can fund <strong>for</strong> patients and thereby reducing the<br />
incidence of post-code prescribing.” Source (Department of Health (DoH) published press release<br />
notice Ref 2000/0252)<br />
In addition, the release of <strong>National</strong> Service Frameworks that address, <strong>for</strong> example, the prevention,<br />
management and <strong>treatment</strong> of chronic diseases, are of importance.<br />
7.1 The <strong>National</strong> Institute <strong>for</strong> Health and Clinical Excellence (NICE)<br />
<strong>National</strong> Institute <strong>for</strong> Health and Clinical Excellence (NICE) is an independent organisation<br />
responsible <strong>for</strong> providing national guidance on <strong>treatment</strong>s and care. NICE guidance is available to<br />
healthcare professionals, patients and carers to help them make healthcare decisions.<br />
Page 14 of 35
<strong>Commissioning</strong> Policy <strong>for</strong> Exceptional Treatment Requests<br />
Once NICE guidance is published, health professionals are expected to take it fully into account<br />
when exercising their clinical judgment. However, NICE guidance does not override the individual<br />
responsibility of health professionals to make decisions appropriate to the circumstances of the<br />
individual patient, in consultation with the patient and/or their guardian or carer.<br />
The Chief Executive of each NHS organisation is ultimately accountable <strong>for</strong> the implementation of<br />
NICE guidance.<br />
7.2 Guidance from the <strong>National</strong> Institute <strong>for</strong> Health and Clinical Excellence (NICE)<br />
Currently NICE produces guidance in three areas:<br />
the use of new and existing medicines and <strong>treatment</strong>s within the NHS in England and Wales –<br />
Technology Appraisals<br />
the appropriate <strong>treatment</strong> and care of people with specific diseases and conditions with the<br />
NHS in England and Wales – Clinical Guidelines<br />
the use of surgical or other invasive interventions <strong>for</strong> diagnosis of <strong>treatment</strong> as to their safety<br />
and effectiveness – Interventional Procedures<br />
The NICE website also publishes Public Health Guidance.<br />
Since January 2002, Primary Care Trusts have been required to provide funding and resources <strong>for</strong><br />
drug therapies and other interventions recommended by NICE through its Technology<br />
Appraisals.<br />
The NHS normally has three months from the date of publication <strong>for</strong> each Technology Appraisal to<br />
provide funding and resources. NICE may extend this period if there are good reasons, such as<br />
lack of trained, specialist staff to implement the service.<br />
There is currently no standard time scale <strong>for</strong> the implementation of either NICE Clinical<br />
Guidelines or guidance on Interventional Procedures, although specific advice is sometimes<br />
given by the Department of Health. Where a referring clinician is of the opinion that the <strong>treatment</strong><br />
he advises to a patient falls within NICE Clinical Guidelines or Interventional Procedures that will be<br />
advised/used <strong>for</strong> <strong>treatment</strong> across multiple patients then this must not be processed through the<br />
ETR route and a <strong>for</strong>mal business case must be made to the Director of Patient Experience &<br />
Service Improvement. Submitted business cases should be endorsed by the Provider Organisation<br />
at a corporate level prior to their submission. This will ensure appropriate <strong>treatment</strong>s are fully<br />
evaluated and financed within contract, if necessary as an in-year decision through the Contract<br />
Variation process or annually through the LDP process. (See Appendix 5).<br />
7.3 The Healthcare Commission<br />
The Healthcare Commission (previously known as the Commission <strong>for</strong> Healthcare Audit and<br />
Inspection - CHAI) is responsible <strong>for</strong> monitoring progress on the implementation of NICE guidance<br />
nationally.<br />
7.4 <strong>National</strong> Service Frameworks<br />
As part of its commitment to improving health and reducing inequalities the Department of Health<br />
has produced <strong>National</strong> Service Frameworks (NSFs). NSFs do this by setting national standards,<br />
Page 15 of 35
<strong>Commissioning</strong> Policy <strong>for</strong> Exceptional Treatment Requests<br />
defining service models, putting in place strategies to support implementation and establishing<br />
per<strong>for</strong>mance measures against which progress is measured. NSFs have been published in a<br />
number of disease areas, <strong>for</strong> example, coronary heart disease; cancer; paediatric intensive care;<br />
mental health; older people; diabetes; long-term conditions; renal services; children, young people<br />
and maternity services.<br />
Where a referring clinician is of the opinion that the <strong>treatment</strong> he advises to a patient falls within<br />
NSF recommendations that will be advised/used <strong>for</strong> <strong>treatment</strong> across multiple patients then this<br />
must not be processed through the ETR route and a <strong>for</strong>mal business case must be made to the<br />
Director of Patient Experience & Service Improvement. Submitted business cases should be<br />
endorsed by the Provider Organisation at a corporate level prior to their submission. This will<br />
ensure appropriate <strong>treatment</strong>s are fully evaluated and financed within contract, if necessary as an<br />
in-year decision through the Contract Variation process or annually through the LDP process.<br />
8 Research<br />
As regards clinical research, this must be funded by appropriate research designated monies and<br />
not through budgets that the PCT has allocated <strong>for</strong> the commissioning of health services, or<br />
funding Exceptional Treatment Requests (ETRs).<br />
However, in line with Health Service Guideline (HSG (97) (32) – 1997) The PCT will meet the<br />
additional costs of patients entered into NHS supported research trials (only where local<br />
agreements have been negotiated.) The PCT will not support clinical trials that have not been<br />
supported by the NHS research and Development Agency.<br />
With regard to new healthcare interventions, the <strong>treatment</strong> of rare conditions, or interventions <strong>for</strong><br />
which there is currently little evidence of effectiveness, the PCT may request that NHS<br />
organisations provide data to national or regional databases in order to facilitate the accumulation<br />
of knowledge and experience.<br />
As indicated previously, the PCT will not support the prescribing of unlicensed or unapproved drugs<br />
outside the context of a well designed trial unless there are fully assessed clinical, social and<br />
psychological circumstances that prove undoubted benefit to the patient by the use of the<br />
<strong>treatment</strong>/intervention, with consideration of current resources, agreed in advance with the<br />
responsible PCT.<br />
The PCT will not automatically pick up the funding of a patient‟s drug once they come off a trial.<br />
Patients should be made aware of this if entered into a trial and the trial co-ordinator, not the PCT,<br />
must identify clear exit strategy to the PCT and the patient as part of the trial protocol, with this<br />
in<strong>for</strong>mation fully in<strong>for</strong>med to the patient.<br />
The PCT will not automatically pick up the funding of a patient who has been sponsored by a drug<br />
company <strong>for</strong> a limited period of time. Approval must be sought prior to discussing this with the<br />
patient and certainly be<strong>for</strong>e commencing <strong>treatment</strong>.<br />
The PCT reserve the right to review the evidence of the safety, efficacy and cost-efficiency of the<br />
drug trial prior to funding any drug and to take account of the PCT‟s financial situation.<br />
Page 16 of 35
<strong>Commissioning</strong> Policy <strong>for</strong> Exceptional Treatment Requests<br />
9 Decision Process <strong>for</strong> unlicensed or unproven Drug and<br />
Therapeutic Interventions<br />
In order to provide a broad view on the implications of a request <strong>for</strong> funding approval <strong>for</strong> an<br />
unlicensed drug or unproven therapeutic therapy, the Health Economy Nice Implementation Group,<br />
hereafter known as HENIG, supports the ETAP by providing a Guidance Note when requested <strong>for</strong><br />
a Technology Appraisal on the approval schedule whilst they are in progress prior to their<br />
approval/unapproval. A Public Health Specialist attends the ETAP to ensure specialist knowledge<br />
is available during the decision making <strong>for</strong> ETRs with regard to Clinical Guidelines and<br />
Interventional Procedures.<br />
HENIG will manage and correspond regarding funding <strong>requests</strong> <strong>for</strong>:<br />
* All technologies <strong>for</strong> which NICE has issued a draft consultation or subsequent document as part<br />
of the Technology Appraisal process.<br />
* All PbR exclusions which have been prospectively identified with the acute trust as subject to<br />
agreed guidelines (such as the Specific Product Characteristics (SPC) or appropriate clinical<br />
criteria).<br />
If a Clinician wishes to enable patient access to a specific healthcare intervention which is subject<br />
to NICE Clinical Guidelines and/or Interventional Procedures, or vary criteria within NICE Clinical<br />
Guidance <strong>for</strong> a Technology Appraisal, <strong>for</strong> all patients or a selected group of patients, then a<br />
Business Case proposal must be submitted to the PCT (See Appendix 5) and will be evaluated at<br />
HENIG in order that an appropriate analysis can be made and thereafter appropriate<br />
commissioning undertaken through the LDP, <strong>Commissioning</strong> and Contracting processes.<br />
If a clinician wishes to provide a <strong>treatment</strong> <strong>for</strong> an individual patient who does not meet the eligibility<br />
criteria specified in NICE Guidance as a Technology Appraisal, or the <strong>treatment</strong> is outside of the<br />
PCT Service Level Agreement/Contract, then an application should be made to the PCT‟s ETAP<br />
through the Exceptional Treatment (ETR) process. Details of the ETR procedure are listed in<br />
the ETR section at Section 4 of this <strong>policy</strong>. Public Health will provide specialist advice to ETAP<br />
on the evidence base <strong>for</strong> the intervention in addition to the in<strong>for</strong>mation provided by the clinician<br />
requesting funding.<br />
As required the PCT will also obtain a broad view on the implications of funding the intervention<br />
from appropriate teams including the Specialist Services <strong>Commissioning</strong> Team at the Strategic<br />
Health Authority (SHA).<br />
10 Managing the entry of new drugs<br />
New drug therapies are constantly being developed and this leads to pressure from both patients<br />
and the pharmaceutical industry to prescribe them.<br />
NHS Trusts employ their own mechanisms <strong>for</strong> managing the entry of new drugs into the health<br />
economy and should fund them from within their existing resources or planned <strong>for</strong> as a service<br />
development within the Local Delivery Plan.<br />
Page 17 of 35
<strong>Commissioning</strong> Policy <strong>for</strong> Exceptional Treatment Requests<br />
The PCT works with NHS Trusts and relevant clinical networks to develop joint prescribing<br />
arrangements to achieve the introduction of effective and cost-effective new drug therapies. Where<br />
a new drug or procedure is deemed to have significant<br />
health benefit and is not the subject of a Technology Appraisal a business case should be made<br />
and <strong>for</strong>warded as per Appendix 5 <strong>for</strong> evaluation at HENIG and funding will need to be prioritised<br />
against other clinical areas. Formulary approval from the Area Medicines Management Committee<br />
will also need to be sought.<br />
The PCT will not generally commission drugs that are unlicensed <strong>for</strong> use in the UK.<br />
10.1 Prescribing Responsibility<br />
Prescribing responsibility lies with the person who signs the prescription.<br />
11 Co-funding<br />
The PCT will not co-fund <strong>treatment</strong>s/drugs/therapeutic interventions as outlined in Section 13 of the<br />
<strong>National</strong> Health Services Act 2006. The PCT is currently developing a <strong>policy</strong> on Co-funding.<br />
12 Policy Review<br />
This <strong>policy</strong> will be reviewed as required or no later than 2 years after agreement or following the<br />
introduction of new and relevant legislation will be reviewed within 3 months. PEC will review this<br />
<strong>policy</strong> and will receive an annual report from the Contracts Department.<br />
13 Distribution<br />
This <strong>policy</strong> will be made available to all Dudley GP Practices, Professional Executive Team, Dudley<br />
Group of Hospitals NHS Trust, Local Acute Providers and PALS.<br />
14 Reference Documents<br />
1. Health Act 1999<br />
2. Department of Health HSG97(32)<br />
3. Department of Health press release notice 2000/0252<br />
4. Department of Health press release notice 2005/0379<br />
5. NICE 2006/017<br />
6. Redditch and Bromsgrove PCT <strong>Commissioning</strong> Policy, the funding of drugs <strong>for</strong> patients<br />
coming off drug trials or drug company sponsored patients<br />
7. Swindon PCT – Clinical Priorities Policy <strong>for</strong> commissioning Selected Services<br />
8. Mills and Reeve Solicitors: Herceptin: Briefing following Rogers v. Swindon PCT (April 2006)<br />
9. Mills and Reeve Solicitors: Vital Signs (Winter 2005)<br />
10. Department of Health - Improvement, Expansion and Re<strong>for</strong>m: The next 3 years: Priorities<br />
and Planning Framework 2003-2006<br />
11. Department of Health – The NHS Cancer Plan, A plan <strong>for</strong> investment, A plan <strong>for</strong> re<strong>for</strong>m<br />
(September 2000)<br />
12. Mills and Reeve Solicitors: Primary Care Trusts <strong>Commissioning</strong> novel or uncertain<br />
<strong>treatment</strong>s (Health Client Briefing – undated)<br />
Page 18 of 35
<strong>Commissioning</strong> Policy <strong>for</strong> Exceptional Treatment Requests<br />
Appendix 1 - Membership of ETAP<br />
Membership of Exceptional Treatment Approval Panel (ETAP) - February 2008<br />
Director of Patient Experience & Service Improvement (Chairperson) or nominated<br />
Deputy)<br />
2 Clinical Representatives of which 1 must be GP representatives (ensuring where<br />
possible representation from North and South Dudley Clusters)<br />
Public Health Advisor<br />
Lay representative and/or Non-Executive Director<br />
The PCT Manager with responsibility <strong>for</strong> Exceptional Treatment Requests will also attend<br />
the meetings.<br />
Notes:<br />
Other parties may be co-opted onto the group as the need arises, <strong>for</strong> example Health<br />
Economist.<br />
The ETAP will be quorate when there is a minimum of 5 in attendance or involved in the meeting.<br />
These 5 persons should include the Chairperson or nominated Deputy Chairperson, a<br />
representative from Public Health from the PCT, 2 Clinical representatives of which one must be a<br />
Dudley GP representative and a lay representative or Non-Executive Director. However, in the<br />
event of an even number in attendance at ETAP, the Chair will abstain from the vote.<br />
Expertise of the clinical panel members – Principal expertise is in interpreting clinical evidence and<br />
other clinical in<strong>for</strong>mation including cost effectiveness to enable decision making and allocating<br />
scarce resources across competing priorities. The panel will seek evidence when necessary from<br />
Specialists within<br />
individual clinical fields.<br />
Expertise of lay or Non-Executive Director members – Principal input is to provide patient<br />
independent perspective <strong>for</strong> input in decision making and allocating scarce resources across<br />
competing priorities.<br />
Page 19 of 35
<strong>Commissioning</strong> Policy <strong>for</strong> Exceptional Treatment Requests<br />
Appendix 2 – ETR Pro-<strong>for</strong>ma<br />
Application Form<br />
Exceptional Treatment Request (ETR) – Dudley PCT<br />
Name of clinician making application<br />
Patients Name<br />
Patients Address<br />
Date of Birth<br />
GP Name<br />
Practice Address<br />
Brief and relevant health history,<br />
current patient condition including any<br />
patient individual applicable<br />
circumstances<br />
Treatment/intervention requested<br />
Page 20 of 35
Clinical Urgency Rate:<br />
Emergency / Urgent / Routine<br />
(please delete as appropriate)<br />
Clinical Emergency<br />
Within 2 working days<br />
Clinically Urgent<br />
Within 14 working days<br />
Clinically Routine<br />
<strong>for</strong> decision at routine ETAP<br />
meetings<br />
<strong>Commissioning</strong> Policy <strong>for</strong> Exceptional Treatment Requests<br />
In<strong>for</strong>mation on alternative <strong>treatment</strong>(s)<br />
available and in<strong>for</strong>mation regarding<br />
previous <strong>treatment</strong>s provided.<br />
Proposed provider of <strong>treatment</strong> – to<br />
include alternative providers.<br />
Cost implications (including any<br />
maintenance costs) and length of any<br />
monitoring arrangements.<br />
Evidence that the <strong>treatment</strong> proposed<br />
has the potential to result in health<br />
improvement <strong>for</strong> the patient, including<br />
recent evidence of effectiveness. (A<br />
decision not to commission a<br />
service/therapy often reflects a lack of<br />
evidence of effectiveness, or evidence<br />
of limited benefit balanced against<br />
adverse effects. Please provide details<br />
of research/clinical evidence that<br />
supports this particular application.<br />
Reference to articles and copies of<br />
reports may be attached, including any<br />
NICE recommendations.<br />
Page 21 of 35
<strong>Commissioning</strong> Policy <strong>for</strong> Exceptional Treatment Requests<br />
Please document what in<strong>for</strong>mation<br />
regarding the proposed <strong>treatment</strong> you<br />
have provided to the patient and<br />
document what you have told the<br />
patient about the proposed <strong>treatment</strong>.<br />
Implications <strong>for</strong> the patient if proposed<br />
<strong>treatment</strong> is not funded.<br />
Rationale <strong>for</strong> bringing this case to the<br />
Exceptional Funding Approval (ETAP)<br />
How do you propose to monitor and<br />
evaluate effectiveness of this<br />
<strong>treatment</strong>/intervention and how and<br />
when will you report back to the PCT.<br />
Please confirm that you in<strong>for</strong>med the<br />
patient that you have applied <strong>for</strong><br />
funding.<br />
What benefits would you expect <strong>for</strong> this<br />
patient as a result of receiving this<br />
<strong>treatment</strong><br />
Has the patient been in<strong>for</strong>med of any<br />
associated risks associated with this<br />
<strong>treatment</strong><br />
I confirm that all of the in<strong>for</strong>mation<br />
provided within this <strong>for</strong>m is accurate<br />
and has been fully discussed with the<br />
patient.<br />
Page 22 of 35
<strong>Commissioning</strong> Policy <strong>for</strong> Exceptional Treatment Requests<br />
Additional in<strong>for</strong>mation may be<br />
submitted to the ETAP if they or their<br />
representatives wish.<br />
Please confirm you have discussed<br />
this with the patient.<br />
Any in<strong>for</strong>mation from the patient MUST<br />
be submitted with this pro-<strong>for</strong>ma.<br />
I confirm that I have read and<br />
understood the appropriate<br />
<strong>Commissioning</strong> Policy (if applicable).<br />
Signed<br />
Date<br />
Please Return <strong>for</strong>m to:<br />
Exceptional Treatment Request Manager<br />
Contracts Department<br />
Dudley PCT<br />
St Johns House<br />
Union Street<br />
Dudley<br />
DY2 8PP<br />
Fax No: 01384 366497<br />
Email: ETR@dudley.nhs uk<br />
Page 23 of 35
<strong>Commissioning</strong> Policy <strong>for</strong> Exceptional Treatment Requests<br />
APPENDIX 3 - Appeals Procedure<br />
Introduction<br />
Appeals Procedure <strong>for</strong> Exceptional Treatment Requests<br />
The Appeals Panel (the Panel) is established as the Panel <strong>for</strong> the PCT Board to consider appeals<br />
by a referring Medical Practitioner and/or their patient against a decision of the PCT Exceptional<br />
Treatment Approval Panel (ETAP). Where a decision to refuse an ETR is made the patient will be<br />
advised of their right to appeal the decision in writing and the process <strong>for</strong> doing so. Where a<br />
Medical Practitioner is appealing on behalf of the patient this needs to be confirmed by patient<br />
written consent to the PCT.<br />
Initiating the Appeal<br />
The right of appeal is valid <strong>for</strong> a period of 25 days following the date of letter advising that the ETR<br />
has been refused. A letter from the patient/advocate requesting an appeal against the process<br />
must be provided to:<br />
Exceptional Treatment Request Manager<br />
The Contracts Department<br />
Dudley PCT<br />
St Johns House<br />
Dudley<br />
DY2 8PP<br />
Fax No: 01384 366497(safe haven fax rules apply)<br />
Email: ETR@dudley.nhs.uk<br />
Role of the Appeals Panel<br />
The Panel‟s role is to consider whether the correct process has been followed to reach a decision.<br />
The appeals panel should ensure that the ETAP have considered the following factors:<br />
• Does the patient meet PCT referral criteria<br />
• Analysis of proposed <strong>treatment</strong><br />
• Analysis of alternative <strong>treatment</strong> and its cost effectiveness/value <strong>for</strong> money<br />
• Precedent setting<br />
• Long term benefits/cost analysis<br />
• Nature of proposed <strong>treatment</strong>/intervention and its clinical effectiveness<br />
• Patient <strong>exceptional</strong> circumstances<br />
• Number of people in Dudley that may be affected by the decision.<br />
The Appeals panel does not have the jurisdiction to change/amend PCT <strong>Commissioning</strong> Policies<br />
that have been approved by the PCT Board and will make decisions based on current<br />
<strong>Commissioning</strong> Policies at the time of the Appeals hearing.<br />
Should the referring clinician/patient wish to challenge a PCT <strong>Commissioning</strong> Policy, this will need<br />
to be in writing addressed to the Director of Patient Experience & Service Improvement in the first<br />
instance.<br />
Page 24 of 35
<strong>Commissioning</strong> Policy <strong>for</strong> Exceptional Treatment Requests<br />
Should the Appeals Panel uphold an appeal, the case must be referred back to the ETAP to be<br />
reconsidered.<br />
Membership<br />
The Panel shall comprise of a minimum of 5 persons none of whom should have sat on the ETAP<br />
<strong>for</strong> the case under consideration. There shall be at least one Non-Executive Director, one Director<br />
who is not the Chief Executive and who is from the <strong>Commissioning</strong> arm of the PCT (not Provider<br />
Services), this includes Directors of Governance, Public Health and Patient Experience & Service<br />
Improvement), together with at least one GP representative (who must be a member of the PEC, a<br />
Clinical Lead or PBC Cluster Chair), a Public Health representative, a commissioning<br />
representative or a finance representative (this representative must have expertise in Local<br />
Development Plan (LDP) knowledge). The panel will decide prior to the meeting commencing who<br />
will chair the appeals panel, this would normally be either the Non-Executive Director or PCT<br />
Director. The panel Chairperson may co-opt onto the Panel a Medical Practitioner, nurse or other<br />
healthcare professional with relevant healthcare expertise. The patient will be entitled to attend the<br />
hearing and to make oral representations either personally or by a parent, guardian, carer or other<br />
appropriate advocate.<br />
Appeals Secretary<br />
The servicing and administrative support to the Panel will be undertaken by a member of the PCT<br />
staff from the Contracts or <strong>Commissioning</strong> Departments who will be responsible <strong>for</strong> managing the<br />
administration of the appeal from receipt of the letter of appeal through to the notification of the<br />
decision. The Appeals Secretary will ensure the patient is provided with a copy of the papers which<br />
have been presented to the Panel.<br />
Evidence available to the Appeals Panel<br />
a) Documents<br />
i) All documents that were available to the ETAP together with the decision and<br />
reasons.<br />
ii)<br />
Any further in<strong>for</strong>mation that has come to light since the ETAP decision.<br />
b) Representations<br />
i) Upon prior written application by the patient to the Chairperson of the Panel at an<br />
interval of not less than 5 working days prior to the Appeals Panel Meeting date, the<br />
patient will be entitled to attend the hearing and to make oral representations either<br />
personally or by a parent, guardian, carer or other appropriate advocate. The patient<br />
must advise the Chairperson within the above timescale of any persons attending the<br />
hearing with them and in what capacity they will be attending. The maximum number<br />
of persons attending the Appeal Panel is 3 persons in total. Where this right is<br />
enacted upon by the patient, the patient/patient‟s representatives will have the<br />
opportunity during the meeting to present their case, however, the panel members will<br />
deliberate the decision in private thereafter.<br />
Page 25 of 35
Holding the Panel Hearing<br />
<strong>Commissioning</strong> Policy <strong>for</strong> Exceptional Treatment Requests<br />
The Chairperson of the Panel will state the remit of the panel and the criteria against which their<br />
decision is to be taken at the opening address to all in session at the hearing. The Chairperson of<br />
the panel will identify at the outset of the session which members are the decision makers and<br />
clearly identify in what capacity other members of the PCT are in session on behalf of the PCT.<br />
The Appeals Panel discussions will be recorded on digital recording equipment <strong>for</strong> the purpose of<br />
accurate minute taking only. The digital recording of each Appeal hearing will be kept no longer<br />
than is required to transcribe the recording into minutes <strong>for</strong> the Panel and in any event no longer<br />
than 10 working days. Once the minutes have been agreed by the Chair of the Appeals Panel, the<br />
digital recording will be destroyed. Consent to record this meeting will be sought from the patient<br />
prior to the Appeals Panel commencing (See Appendix 4) – Digital Recording of Appeals<br />
Procedure.<br />
The designated officer will <strong>for</strong>mally present and explain to the Panel the basis of the <strong>exceptional</strong><br />
request.<br />
The Panel will have the opportunity to question the designated officer and to clarify any points<br />
within the briefing papers.<br />
The patient and/or representative should then be invited to present any in<strong>for</strong>mation that s/he feels<br />
to be relevant to the Panel. The Panel may also wish to ask questions in order to clarify points with<br />
the patient/representative.<br />
The patient/representative and the designated officer will then be requested to withdraw from the<br />
meeting enabling the panel to deliberate in private.<br />
The Panel will then consider whether there is sufficient in<strong>for</strong>mation available to enable it to arrive at<br />
a decision. If this is not the case then the Chairperson should adjourn the hearing and request the<br />
designated officer to obtain the in<strong>for</strong>mation or arrange <strong>for</strong> the appropriate person to attend at the<br />
next meeting, along with the patient/representative if they request to do so.<br />
If no further in<strong>for</strong>mation is deemed necessary, the Panel should make its decision in accordance<br />
with the remit which is set out below.<br />
Decision making remit of the Panel:<br />
The Appeal Panel will at the end of their deliberation either<br />
1. Uphold the appeal and refer the case back to ETAP or<br />
2. Reject the appeal and confirm the decision of the ETR panel.<br />
The decision of the panel will be notified to the patient in writing by the Chief Executive of the PCT<br />
within 10 working days of the decision being taken.<br />
Any further clarification of the appeal decision by the patient must be made in writing and directed<br />
to the Chief Executive of the PCT. The PCT will respond accordingly in writing.<br />
When an appeal panel deems it necessary that a debriefing session <strong>for</strong> panel members following<br />
the appeal is necessary this will be organized by the Appeal Secretary.<br />
Page 26 of 35
<strong>Commissioning</strong> Policy <strong>for</strong> Exceptional Treatment Requests<br />
Confidentiality<br />
Panel members are bound by the Code of Confidentiality in respect of all written material and<br />
verbal discussions concerning the appeal. All papers are to be collected at the end of the Panel‟s<br />
sitting except those required by an executive member <strong>for</strong> subsequent action. Any member who<br />
does not attend the sitting is responsible <strong>for</strong> returning all papers to the Appeals Secretary <strong>for</strong><br />
shredding.<br />
Complaints<br />
If a complaint is made about the handling of an appeal, the PCT‟s complaints procedure can be<br />
invoked within 6 months of the date of notification of the decision to the patient by the Appeal Panel<br />
Chairperson. If the complaint relates to the impact of a commissioning <strong>policy</strong> on an individual then<br />
the complaints procedure will only be implemented once the Appeal Panel has reached a final<br />
decision. Please note: A complaints investigation will review the process only and not the decision<br />
made by the Appeals Panel.<br />
Health Care Commission<br />
Following a complaint, if we have been unable to resolve all concerns, the patient has the right to<br />
ask the Healthcare Commission to review the process. This should be done within 6 months of<br />
receiving the response to the complaint. The Healthcare Commission is an independent body<br />
established to promote improvements in health care through the assessment of the per<strong>for</strong>mance of<br />
those who provide services. Their website address is: www.healthcarecommission.org.uk.<br />
You can contact the Healthcare Commission on 0845 601 3012 or write to them at:<br />
Healthcare Commission<br />
Complaints Team<br />
Peter House<br />
Ox<strong>for</strong>d Street<br />
Manchester<br />
M1 5AN<br />
Patient Advice and Liaison Service<br />
The role of PALS is to provide in<strong>for</strong>mation, advice and support to patients, service users, carers<br />
and relatives with concerns or issues about their health service.<br />
PALS liaises with service providers and other outside agencies to resolve patient queries, concerns<br />
and issues and assists services with learning lessons.<br />
Page 27 of 35
<strong>Commissioning</strong> Policy <strong>for</strong> Exceptional Treatment Requests<br />
Appendix 4 – Digital Recording of Appeals Procedure<br />
Background<br />
The <strong>Commissioning</strong> Policy Group has agreed that due to the increasing complexities and length of<br />
Appeal hearings, that the accurate recording of minutes using manual shorthand alone is becoming<br />
unattainable. The group recognises the importance of accurate record keeping in this area and its<br />
impact on the Trust‟s requirements under the Data Protection Act 1998 and Freedom of In<strong>for</strong>mation<br />
Act 2000. The Group has purchased a number of dictaphones to enable the digital recording of<br />
Appeals as an administration aid only.<br />
Agreed Procedure<br />
At the commencement of each appeal hearing all attendee‟s will be in<strong>for</strong>med of the presence and<br />
purpose of the digital recording equipment. The digital recording of each Appeal hearing will be<br />
kept no longer than is required to transcribe the recording into minutes <strong>for</strong> the Panel and in any<br />
event no longer than 10 working days. This is solely <strong>for</strong> the purpose of minute taking.<br />
Management and Retention<br />
The digital recording will be stored in a secure area whilst not in use; all recording will be clearly<br />
labeled until such time as the digital recording is erased. The retention period <strong>for</strong> the digital<br />
recording is no longer than 10 working days. Should a request <strong>for</strong> a copy of the recording be<br />
received after this timescale has elapsed then a final check should be made to ensure that the<br />
Trust no longer holds the in<strong>for</strong>mation in digital recording <strong>for</strong>m, if this is the case a refusal <strong>for</strong> the<br />
in<strong>for</strong>mation can be appropriately provided under the requirements of both the Data Protection and<br />
Freedom of In<strong>for</strong>mation Act.<br />
Requests <strong>for</strong> In<strong>for</strong>mation<br />
Should a request <strong>for</strong> in<strong>for</strong>mation held on digital recording equipment be received prior to the<br />
expiration of the retention period the digital recording should immediately be removed from the<br />
process of erasure and re-use. All such <strong>requests</strong> and digital recordings should be provided to the<br />
In<strong>for</strong>mation Governance Department which will administer the process of duplication and release of<br />
appropriate in<strong>for</strong>mation with legislative boundaries.<br />
Dudley Primary Care Trust holds and processes personal in<strong>for</strong>mation in accordance with the<br />
requirements of the Data Protection Act 1998. Any person upon request is entitled to any<br />
in<strong>for</strong>mation held about them by the Trust. Any request <strong>for</strong> in<strong>for</strong>mation should be made in writing<br />
and addressed to:<br />
The In<strong>for</strong>mation Governance Department<br />
St Johns House<br />
Union Street<br />
Dudley<br />
DY2 8PP<br />
Page 28 of 35
<strong>Commissioning</strong> Policy <strong>for</strong> Exceptional Treatment Requests<br />
Appendix 5 - Business Case Guidance<br />
Advice and guidance <strong>for</strong> persons providing a Business Case <strong>for</strong> consideration<br />
by Dudley PCT.<br />
Presentation of new drugs, technologies or procedures<br />
The Dudley PCT identify at a local level, whether new drugs and <strong>treatment</strong>s, or <strong>treatment</strong>s that are<br />
not routinely available should be funded, as well as discussing the impact of service developments.<br />
All new Business Cases <strong>for</strong> consideration by the PCT must be sent to:<br />
Director of Patient Experience & Service Improvement<br />
Dudley PCT<br />
St Johns House<br />
Union Street<br />
Dudley<br />
West Midlands, DY2 8PP<br />
Presenters of a Business Case should note funding is allocated on an annual basis through the<br />
commissioning process and LDP planning process. In-year funding may be agreed where<br />
appropriate.<br />
What should the case include<br />
Background<br />
‣ An introduction to the new drug/technology<br />
‣ Is this a new innovation or a new indication <strong>for</strong> an existing drug/technology<br />
NICE guidance (if appropriate)<br />
‣ A summary of NICE recommendations<br />
‣ What are the differences between guidance and current<br />
practice<br />
‣ What are the clinical and service implications of the guidance<br />
‣ What are the financial implications of the guidance<br />
Guidance from other bodies (if appropriate)<br />
‣ Clinical Networks<br />
‣ <strong>National</strong> Professional Groups<br />
‣ Royal Colleges<br />
Current practice<br />
‣ What other/alternative drug/technology is currently being used in Dudley<br />
‣ How many patients are treated<br />
‣ What are the current criteria <strong>for</strong> <strong>treatment</strong><br />
‣ What is the cost of current methods per patient, full year effect<br />
Page 29 of 35
<strong>Commissioning</strong> Policy <strong>for</strong> Exceptional Treatment Requests<br />
Proposal <strong>for</strong> consideration<br />
‣ Outline of proposed usage of drug/technology<br />
‣ Any staffing or service implications<br />
‣ Briefing on drug/technology/indication not being carried out (if applicable)<br />
<strong>National</strong> Priorities<br />
‣ Is the drug/technology a <strong>National</strong> Priority<br />
‣ Has <strong>National</strong> guidance been issued in this area<br />
‣ Is <strong>National</strong> guidance in the pipeline<br />
Local Priorities<br />
‣ How can this <strong>treatment</strong> be funded within the current allocation of resource (i.e. How can<br />
this new <strong>treatment</strong> substitute another <strong>treatment</strong> that is of less value within current<br />
resources)<br />
‣ Where does the <strong>treatment</strong> rank in terms of other priorities within your specialty<br />
‣ Does this <strong>treatment</strong> support the PCTs LDP How<br />
Evidence of effectiveness<br />
‣ Data from research studies should be presented and a list of references provided<br />
‣ What are the benefits<br />
‣ What is the size of the benefit<br />
‣ Do any sub-groups of patients benefit more than others<br />
‣ How many patients will benefit<br />
Cost-effectiveness<br />
‣ Data from economic evaluations should be presented and a<br />
list of references provided<br />
‣ Cost per QALY should be shown where available<br />
Equity<br />
‣ How does the <strong>treatment</strong> compare with those (of the same general type) from other clinical<br />
areas (e.g. life extending <strong>treatment</strong>s from two different clinical areas)<br />
Patients Views<br />
What are the views of individual patients and patient groups with regards to:<br />
‣ Quality of Life<br />
‣ Convenience<br />
‣ Impact on their life<br />
Implications of not using this <strong>treatment</strong><br />
‣ What are the alternatives <strong>for</strong> <strong>treatment</strong><br />
‣ Are patients at risk if this <strong>treatment</strong> is not used If yes, how<br />
Audit process <strong>for</strong> NICE guidance<br />
‣ How will you audit the implementation of the NICE guidance in terms of adherence to the<br />
recommendations and its cost<br />
Financial Impact<br />
A financial impact statement (attached) should be completed and presented by the finance<br />
department of the organisation presenting the business case.<br />
Page 30 of 35
Financial Impact Statement<br />
<strong>Commissioning</strong> Policy <strong>for</strong> Exceptional Treatment Requests<br />
Name of Guideline, Innovation, Drug or Health Technology Assessment:<br />
Trust: Division/Directorate: Specialty:<br />
Change in practice, if any.<br />
Please include any procedure or drug this innovation will replace – where possible<br />
providing PbR HRG Code/s price or local price).<br />
Proposed Timetable <strong>for</strong> implementation – e.g. introduction with effect from a certain<br />
date or over a number of years.<br />
Major commissioners affected (so that we can work with them to find a consistent<br />
approach). If the data can be split over the main commissioners please do this, if<br />
not, then please list the commissioners here.<br />
„Work group‟ Involved – if applicable. If this has been discussed at a „work group‟<br />
meeting please give date of meeting and/or reference in minutes. (For example –<br />
Cancer Network, local LIT group)<br />
Has this been requested as an ETR previously If so please give date, reference<br />
number and result of decision.<br />
Form completed by /<br />
contact <strong>for</strong> queries:<br />
Name<br />
Position<br />
Tel E-mail Date<br />
Notes:<br />
Page 31 of 35
<strong>Commissioning</strong> Policy <strong>for</strong> Exceptional Treatment Requests<br />
Number of patients expected to be<br />
treated - this may build up over a period of<br />
years.<br />
Current Year<br />
Next Year<br />
Full Year<br />
Total (Gross) Cost – this may include<br />
staff, drugs, equipment etc. Again it would<br />
be useful to show the total costs <strong>for</strong> the<br />
Trust and the amount that would be<br />
required from each Commissioner. This<br />
may simply be in the same proportion as<br />
the number of patients.<br />
This section must also include any<br />
associated impacts on long and or short<br />
term PbR activity, <strong>for</strong> example: the<br />
inclusion of any associated day case costs<br />
to provide the <strong>treatment</strong>.<br />
Cost Savings from ceasing previous<br />
<strong>treatment</strong> – if applicable.<br />
Current Year<br />
Next Year<br />
Full Year<br />
Current Year<br />
Next Year<br />
Full Year<br />
Net (Additional) Cost – i.e. Total or Gross<br />
Cost less Savings. If the new procedure<br />
replace a more expensive one this will be<br />
Net Savings.<br />
Any funding already agreed – please<br />
say if some of this has already been<br />
recognised by the PCT or other<br />
Commissioners. Please say which<br />
Commissioners have agreed funding.<br />
Current Year<br />
Next Year<br />
Full Year<br />
Current Year<br />
Page 32 of 35
<strong>Commissioning</strong> Policy <strong>for</strong> Exceptional Treatment Requests<br />
Appendix 6 – Process of Managing Exceptional Treatment Requests<br />
ETR pro-<strong>for</strong>ma completed by<br />
Clinician and sent to the<br />
Contracts Department at the<br />
Dudley PCT<br />
Contracts Department log receipt of pro-<strong>for</strong>ma and acknowledge receipt to referrer via email within 3<br />
working days. Contracts/<strong>Commissioning</strong> staff check the pro-<strong>for</strong>ma <strong>for</strong> completeness against any related<br />
<strong>policy</strong>/relevant criteria. Incomplete or inappropriate referrals will be returned to the referrer.<br />
Completed <strong>for</strong>ms including any additional in<strong>for</strong>mation received are<br />
copied to the PCT Specialist in Pharmaceutical Public Health <strong>for</strong> review<br />
and a possible a funding decision where criteria are applicable where<br />
necessary (more details available in the full <strong>policy</strong> at Section 4)<br />
Refer to ETAP with any additional<br />
material received from Public Health<br />
or additional professional advice<br />
gathered <strong>for</strong> decision<br />
Decision taken at ETAP.<br />
The outcome from the ETAP or outcome of the criteria based<br />
decision is communicated in writing to the patient, the referrer<br />
and the patient‟s GP within 10 working days following the<br />
decision.<br />
Has there been an appeal<br />
against the process within<br />
25 days<br />
No<br />
Decision logged and any<br />
actions undertaken.<br />
Yes<br />
Refer on to Appeals Panel<br />
Page 33 of 35
<strong>Commissioning</strong> Policy <strong>for</strong> Exceptional Treatment Requests<br />
Appendix 7 – ETR Decision Report<br />
ETR<br />
Number<br />
Case No<br />
ETAP<br />
Decision<br />
Date<br />
Decision<br />
Outcome<br />
Decision<br />
Reasons<br />
1. Agree to fund<br />
2. Defer decision pending further in<strong>for</strong>mation/investigation<br />
3. Refuse to fund<br />
4. Service Development referred to :………………………..<br />
5. Refer to PEC<br />
TREATMENT REQUEST -<br />
Factors involved in considering the ETR decision:<br />
Does the patient meet PCT<br />
available referral criteria<br />
(Criteria score attached if applicable)<br />
Analysis of proposed<br />
<strong>treatment</strong> – documenting<br />
discussion around<br />
guidance available (eg<br />
NICE), effectiveness,<br />
efficacy and safety, MHRA<br />
approval recognition and<br />
VFM<br />
Analysis of alternative<br />
<strong>treatment</strong> and its cost and<br />
effectiveness and VFM<br />
discussion record<br />
Yes/No/Not applicable<br />
Likelihood and discussion<br />
record related to precedent<br />
setting and long term<br />
benefits/costs analysis<br />
Nature of the proposed<br />
<strong>treatment</strong>/intervention –<br />
discussion record regarding<br />
clinical case/s put <strong>for</strong>ward.<br />
Patient <strong>exceptional</strong><br />
circumstances taken into<br />
account – discussion<br />
record. Please note<br />
whether in<strong>for</strong>mation<br />
provided on an ETR Patient<br />
Additional In<strong>for</strong>mation Form<br />
was considered.<br />
Page 34 of 35
Appendix 8 – Abbreviations<br />
<strong>Commissioning</strong> Policy <strong>for</strong> Exceptional Treatment Requests<br />
DoH<br />
GP<br />
HC (CHAI)<br />
HENIG<br />
HRG<br />
HSG<br />
ETAP<br />
ETR<br />
LDP<br />
LIG<br />
MHRA<br />
NICE<br />
NHS<br />
NSF<br />
PALS<br />
PbR<br />
PEC<br />
PCT<br />
QALY<br />
SHA<br />
SPC<br />
VFM<br />
Department of Health<br />
General Practitioner<br />
Healthcare Commission (Commission <strong>for</strong> Healthcare Audit<br />
and Inspection)<br />
Health Economy Nice Implementation Group<br />
Healthcare Resource Group<br />
Health Service Guidance<br />
Exceptional Treatment Approval Panel<br />
Exceptional Treatment Request<br />
Local Delivery Plan<br />
Local Implementation Group<br />
Medicines and Healthcare Products Regulatory Agency<br />
<strong>National</strong> Institute <strong>for</strong> Health and Clinical Excellence<br />
<strong>National</strong> Health Service<br />
<strong>National</strong> Service Framework<br />
Patient Advice and Liaison Service<br />
Payment by Results<br />
Professional Executive Committee<br />
Primary Care Trust<br />
Quality Adjusted Life Year<br />
Strategic Health Authority<br />
Specific Product Characteristics<br />
Value For Money<br />
Page 35 of 35