the dudley group of hospitals nhs trust - Dudley Primary Care Trust
the dudley group of hospitals nhs trust - Dudley Primary Care Trust
the dudley group of hospitals nhs trust - Dudley Primary Care Trust

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
AppendixTHE DUDLEY GROUP OF HOSPITALS NHS TRUSTINFECTION CONTROL SERIOUS ADVERSE INCIDENTSThis policy provides guidance to staff in reporting, managing and monitoringserious adverse infection control incidents. It is an important component <strong>of</strong> <strong>the</strong><strong>Trust</strong>’s Policy on Reporting, Managing and Monitoring <strong>of</strong> Adverse Incidentsand <strong>the</strong> <strong>Trust</strong>’s Risk Management and Patient Safety Strategies.Staff should follow <strong>the</strong> <strong>Trust</strong> main policy on Reporting. Managing andMonitoring Adverse Incidents for all infection control incidents.All Infection Control incidents should be reported in <strong>the</strong> same way as o<strong>the</strong>rincidents but in addition <strong>the</strong> report forms should be copied and sent to <strong>the</strong>Nursing Director /Director <strong>of</strong> Infection Prevention and Control.The following should be treated as Serious Untoward Incidents and should besubject to Root Cause Analysis Investigation with Action plans developed• MRSA Bacteraemias• Infection control ward outbreaks – MRSA, Clostridium difficile, o<strong>the</strong>rorganisms on advice <strong>of</strong> <strong>the</strong> ICT• Serious Infections related to invasive devices• Serious infections on advice <strong>of</strong> ICTMRSA BacteraemiasThe Strategic Health Authority requires <strong>Trust</strong>s to follow a common approach toreporting and investigating MRSA bacteraemias which is set out in Appendix 1for information. This has been incorporated into this <strong>Trust</strong> policy.This <strong>Trust</strong> is responsible for investigating all post 48 hour MRSA bacteraemias(i.e. those identified in <strong>the</strong> patients blood stream after <strong>the</strong> patients has beenadmitted for 48 hours or more).1. Staff must follow <strong>the</strong> pathway ‘Notification <strong>of</strong> MRSA Bacteraemia Infections’set out in Appendix 2.2. The Lead Nurse and Consultant ensure that all post 48 hour MRSAbacteraemias have been reported as a serious adverse incident accordingto <strong>Trust</strong> policy on Reporting, Managing and Monitoring Adverse Incidents.3. The Lead Nurse and Consultant with support from <strong>the</strong> infection controlclinical champions start <strong>the</strong> Root Cause Analysis investigation within 12hours and complete this and <strong>the</strong> action plan within 5 day hours <strong>of</strong>notification <strong>of</strong> bacteraemia using <strong>the</strong> pr<strong>of</strong>ormas and guidance at Appendix3 and 4. As a minimum this investigation should include <strong>the</strong> Lead Nurse,Consultant, a member <strong>of</strong> <strong>the</strong> ICT, and an individual trained in Root CauseAnalysis. The Infection Control clinical champions should be involvedwhere possible. O<strong>the</strong>r staff must be involved e.g. if <strong>the</strong> patient has been ino<strong>the</strong>r wards and departments.
4. The root cause analysis should be used to indicated whe<strong>the</strong>r <strong>the</strong> infectionwas avoidable and if <strong>the</strong>re were any contributory factors. These should beclearly identified on <strong>the</strong> RCAs5. The Matron and Medical Service Head are responsible for ensuring <strong>the</strong>RCA and action plan is completed in <strong>the</strong> timescales.6. The RCA and action plan should be sent immediately to <strong>the</strong> NursingDirector/ Director <strong>of</strong> Infection Prevention and Control and <strong>the</strong> ConsultantMicrobiologist for onward reporting.7. The action plan addressing <strong>the</strong> main findings, <strong>the</strong>mes and lessons learnedshould be implemented8. The RCA and action plan should be presented to <strong>the</strong> Clinical UnitManagement Team by <strong>the</strong> consultant and lead nurse and reported to <strong>the</strong>following at <strong>the</strong> next available meetings:a. Infection Control Committee – presented by <strong>the</strong> Clinical Championsb. The Patient Safety Committee – presented by <strong>the</strong> Matron andMedical Service Headc. The Integrated Governance committee – as part <strong>of</strong> <strong>the</strong> PatientSafety report at <strong>the</strong> next meetingd. <strong>Trust</strong> Board – by <strong>the</strong> Director <strong>of</strong> Infection Prevention and Control(DIPC) / Governance Lead at <strong>the</strong> next meetinge. PCT / Strategic HA – by <strong>the</strong> DIPC by 15 th <strong>of</strong> each month.f. As part <strong>of</strong> MESS data – by <strong>the</strong> Consultant Microbiologist9. The Medical Service Head and Matron are accountable for <strong>the</strong> MRSAbacteraemias in <strong>the</strong> clinical unit and are responsible for monitoring <strong>the</strong>implementation <strong>of</strong> <strong>the</strong> action plan and for reporting through <strong>the</strong> GovernanceStructure to <strong>the</strong> Integrated Governance Committee.10. Where a MRSA bacteraemia is noted to be a pre-48 hour infection (patientis clinically symptomatic and tests +ve within <strong>the</strong> first 48 hours <strong>of</strong>admission) in addition to <strong>the</strong> abovea. The DIPC will notify <strong>the</strong> Clinical Governance Lead/ Director <strong>of</strong>Performance and Quality for <strong>the</strong> relevant PCT.b. <strong>Trust</strong> staff will work with <strong>the</strong> Commissioning PCT whoseresponsibility it is to undertake a more in-depth investigation into <strong>the</strong>causative factors.11. The Nursing Director/ DIPC, Chief Executive, Medical Director and Director<strong>of</strong> Operations will meet on a weekly basis to review all matters related toMRSA bacteraemias.12. The Nursing Director and Consultant will ensure <strong>the</strong> Chief Executive isassured that all data submitted to MESS (Mandatory Enhanced MRSAsurveillance) is accurate and timelyInvestigation <strong>of</strong> O<strong>the</strong>r infectionsRoot Cause Analysis following <strong>the</strong> <strong>Trust</strong>’s general procedure should beundertaken• Infection control ward outbreaks – MRSA, Clostridium difficile, o<strong>the</strong>rorganisms on advice <strong>of</strong> <strong>the</strong> ICT• Serious Infections related to invasive devices• Serious infection on advice <strong>of</strong> ICT
THE DUDLEY GROUP OF HOSPITALS NHS TRUSTMRSA BACTERAEMIA ROOT CAUSE ANALYSIS INITIAL ACTIONSCHECK LISTPatients nameReason for AdmissionConsultantDate <strong>of</strong> admissionWardUse <strong>the</strong> MRSA pathways on <strong>Care</strong>net as a guideActionYes / No - add reasonCheck was <strong>the</strong> patient a high risk?Was <strong>the</strong> patient screened?If yes, what was <strong>the</strong> result?Was result documented?If positive resultWas treatment started?Was this documented?Does <strong>the</strong> patient have an invasivedevice?Central line, peripheral cannula, urinaryca<strong>the</strong>ter, PEG, plural drain, o<strong>the</strong>r (specify)Does <strong>the</strong> patient have a wound/lesionYes / No add sites & dateResult and date availableYes/ No – add whereYes/No/ DateYes / NoYes / No- add typeYes / no =describe type andlocationWere blood cultures taken?Was <strong>the</strong> blood culture taken within 48hours <strong>of</strong> admission?If yesYes/ No - Add dateYes /NoPlease email thisinformation to Ann Close –Nursing Directorann.close@dgoh.<strong>nhs</strong>.ukForm Completed by:NameGradeSignature
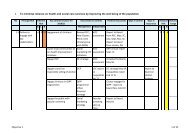
ACTION PLANPROBLEM DISCUSSION CONCLUSION ACTION LEADPERSONTIME SCALEREVIEW