EF summer 08.indd - National Association of Professional Allstate ...
EF summer 08.indd - National Association of Professional Allstate ...
EF summer 08.indd - National Association of Professional Allstate ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
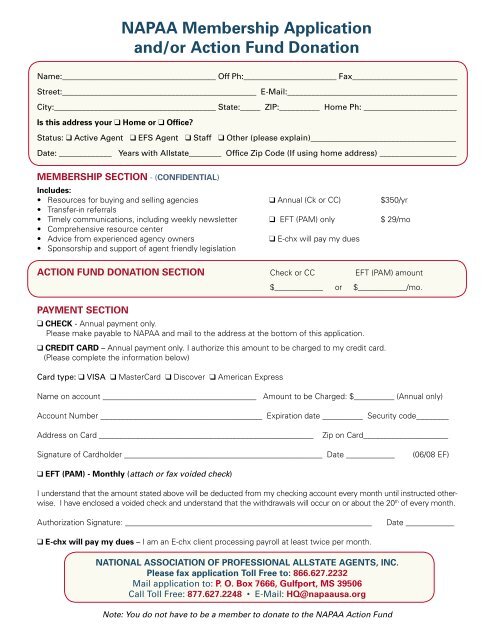
NAPAA Membership Application<br />
and/or Action Fund Donation<br />
Name:______________________________________ Off Ph:_______________________ Fax__________________________<br />
Street:________________________________________________ E-Mail:__________________________________________<br />
City:________________________________________ State:_____ ZIP:__________ Home Ph: _______________________<br />
Is this address your ❑ Home or ❑ Office<br />
Status: ❑ Active Agent ❑ <strong>EF</strong>S Agent ❑ Staff ❑ Other (please explain)____________________________________<br />
Date: _____________ Years with <strong>Allstate</strong>________ Office Zip Code (If using home address) ___________________<br />
MEMBERSHIP SECTION - (CONFIDENTIAL)<br />
Includes:<br />
• Resources for buying and selling agencies ❑ Annual (Ck or CC) $350/yr<br />
• Transfer-in referrals<br />
• Timely communications, including weekly newsletter ❑ <strong>EF</strong>T (PAM) only $ 29/mo<br />
• Comprehensive resource center<br />
• Advice from experienced agency owners<br />
❑ E-chx will pay my dues<br />
• Sponsorship and support <strong>of</strong> agent friendly legislation<br />
ACTION FUND DONATION SECTION Check or CC <strong>EF</strong>T (PAM) amount<br />
PAYMENT SECTION<br />
$____________ or $____________/mo.<br />
❑ CHECK - Annual payment only.<br />
Please make payable to NAPAA and mail to the address at the bottom <strong>of</strong> this application.<br />
❑ CREDIT CARD – Annual payment only. I authorize this amount to be charged to my credit card.<br />
(Please complete the information below)<br />
Card type: ❑ VISA ❑ MasterCard ❑ Discover ❑ American Express<br />
Name on account ______________________________________ Amount to be Charged: $__________ (Annual only)<br />
Account Number ________________________________________ Expiration date __________ Security code________<br />
Address on Card _____________________________________________________<br />
Zip on Card_____________________<br />
Signature <strong>of</strong> Cardholder _________________________________________________ Date ____________<br />
(06/08 <strong>EF</strong>)<br />
❑ <strong>EF</strong>T (PAM) - Monthly (attach or fax voided check)<br />
I understand that the amount stated above will be deducted from my checking account every month until instructed otherwise.<br />
I have enclosed a voided check and understand that the withdrawals will occur on or about the 20 th <strong>of</strong> every month.<br />
Authorization Signature: _____________________________________________________________<br />
Date ____________<br />
❑ E-chx will pay my dues – I am an E-chx client processing payroll at least twice per month.<br />
NATIONAL ASSOCIATION OF PROFESSIONAL ALLSTATE AGENTS, INC.<br />
Please fax application Toll Free to: 866.627.2232<br />
Mail application to: P. O. Box 7666, Gulfport, MS 39506<br />
Call Toll Free: 877.627.2248 • E-Mail: HQ@napaausa.org<br />
Note: You do not have to be a member to donate to the NAPAA Action Fund