Cases Caries Cervical Spine (C1-C2) - Punjab Orthopaedic ...
Cases Caries Cervical Spine (C1-C2) - Punjab Orthopaedic ...
Cases Caries Cervical Spine (C1-C2) - Punjab Orthopaedic ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>Cases</strong> <strong>Caries</strong> <strong>Cervical</strong> <strong>Spine</strong> (<strong>C1</strong>-<strong>C2</strong>) - A Case Report<br />
Jaswinder Pal Singh Walia MS* , Ravinder Pal Kaur MD**, Rakesh Kumar MBBS***,<br />
Sonam Kaur Walia MBBS**** Sargun Singh*****<br />
*Professor, **Ex. Professor, ***Junior Resident, ****Intern, *****Undergdatuate Student<br />
Department of Radio Diagnosis<br />
Government Medical College and Rajendera Hospital, Patiala<br />
Department of <strong>Orthopaedic</strong>s,<br />
Government Medical College and Rajendera Hospital, Patiala<br />
ABSTRACT<br />
Osteoarticular tuberculosis is not a public health problem in most of developed countries, however, in<br />
developing countries it continues to pose one of the major health problems. Vertebral tuberculosis is the most<br />
common form of skeletal tuberculosis and constitutes about 50% of all cases. In the present report, we discuss<br />
the clinical features, diagnostic modes, treatment options and follow-up of upper cervical spine tuberculosis<br />
in a 42 year old male patient.<br />
Keywords: Tuberculosis, <strong>Cervical</strong> spine, Anti Tubercular Therapy<br />
INTRODUCTION<br />
Osteoarticular tuberculosis with all its antecedent complications<br />
continues to pose one of the major health threats in the<br />
developing world. Vertebral tuberculosis is the most common<br />
form of skeletal tuberculosis and constitutes about 50% of all<br />
cases.<br />
While most cases are localized to the dorsal and the lumbar<br />
spine, the involvement of cervical spine accounts for about<br />
12% of the cases and even out of that, involvement of upper<br />
cervical spine is extremely rare. However upper cervical<br />
involvement gains importance because of its potential fatal<br />
consequences if not treated adequately and timely 1 .<br />
CASE SUMMARY<br />
A 36 years old man, college lecturer by profession,<br />
presented to us with complaint of neck pain and stiffness;<br />
with pain radiating to right upper limb. The pain and<br />
stiffness were progressing in spite of him taking analgesics.<br />
Examination revealed mild tenderness over upper cervical<br />
spine; along with painful restriction of cervical movements at<br />
the extremes.<br />
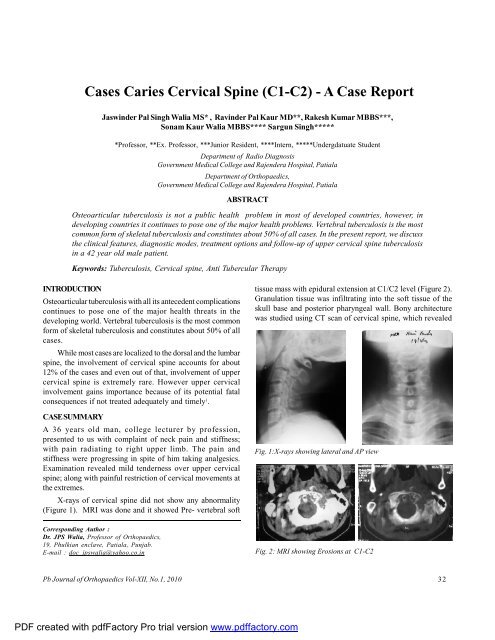
X-rays of cervical spine did not show any abnormality<br />
(Figure 1). MRI was done and it showed Pre- vertebral soft<br />
Corresponding Author :<br />
Dr. JPS Walia, Professor of <strong>Orthopaedic</strong>s,<br />
19, Phulkian enclave, Patiala, <strong>Punjab</strong>.<br />
E-mail : doc_jpswalia@yahoo.co.in<br />
tissue mass with epidural extension at <strong>C1</strong>/<strong>C2</strong> level (Figure 2).<br />
Granulation tissue was infiltrating into the soft tissue of the<br />
skull base and posterior pharyngeal wall. Bony architecture<br />
was studied using CT scan of cervical spine, which revealed<br />
Fig. 1:X-rays showing lateral and AP view<br />
Fig. 2: MRI showing Erosions at <strong>C1</strong>-<strong>C2</strong><br />
Pb Journal of <strong>Orthopaedic</strong>s Vol-XII, No.1, 2010<br />
32<br />
PDF created with pdfFactory Pro trial version www.pdffactory.com
Walia et al<br />
erosion of the dens, left occipital condyle, left lateral mass of<br />
Atlas and articular facet of Axis. ESR was 100 mm at end of 1st<br />
hour and ELISA for tuberculosis was positive.<br />
Patient was diagnosed as a case of caries spine <strong>C1</strong>-2 and<br />
was started anti-tubercular therapy which was continued for<br />
18 months. <strong>Cervical</strong> traction with 5 kg for two months was<br />
given to immobilize the cervical spine; this was followed by<br />
cervical collar to facilitate mobilization of patient.<br />
Patient responded well with Anti-Tubercular Therapy.<br />
The follow-up MRI after 1 year of follow-up showed<br />
complete resolution of pre-vertebral abscess and no<br />
compression of thecal sac or cord displacement was seen at<br />
the end of 1 year (Figure 3).<br />
Fig. 3: Follow-up MRI showing consoilation achieved at <strong>C1</strong>-<strong>C2</strong> with<br />
ATT<br />
DISCUSSION<br />
Vertebral tuberculosis is the commonest form of skeletal<br />
tuberculosis. It is most common during first three decades of<br />
life. Pain and stiffness are earliest complaints. Neck rigidity<br />
and torticollis are seen in severe cases, pain over vertebrae<br />
referred to occiput or arms aggravated by pressure on top of<br />
head, loss of normal lordosis, paralysis of arms and other<br />
neurological symptoms due to compression are seen in all the<br />
cases. <strong>Cervical</strong> tuberculosis has high complication rate. Hsu<br />
and Leong reported 42.5% spinal cord compression rate in 40<br />
patients 2 . In extreme cases, death may occur due to C 1-2<br />
dislocation 3 .<br />
There is no clear-cut consensus regarding conservative<br />
or operative treatment. Lifeso recommended various treatments<br />
for three different stages of <strong>C1</strong>-2 tubercular infection: Stage I<br />
with minimal bone and ligamentous destruction is treated by<br />
trans-oral decompression and immobilization; Stage II with<br />
moderate involvement requires reduction by halo traction<br />
followed by <strong>C1</strong>-2 posterior fusion; and Stage IIII with severe<br />
involvement is treated by posterior fusion of occiput to C3 4 .<br />
Certain authors recommend surgery for both diagnostic<br />
and therapeutic purposes. It enables not only bacteriological<br />
sampling but also medulla decompression and spinal<br />
stabilization, thereby optimizing neurologic and functional<br />
recovery. Surgery enhances local access for antibiotics, by<br />
removing a fibrous barrier 5,6 [9] A.K. Jain, Treatment of<br />
tuberculosis of the spine with neurologic complications, Clin<br />
Orthop Relat Res 398 (2002), pp. 75–84. View Record in Scopus<br />
| Cited By in Scopus (33). Gupta et al. concluded that the<br />
surgery was not necessary, even in patients with advanced<br />
stage of disease (retropharyngeal abscess with or without<br />
Atlanto-Axial Dislocation, gross bony destruction or<br />
angulation) on the basis of their experience of more than 3<br />
decades 7 . Chadha et al. studied craniovertebral tuberculosis<br />
patients managed non-operatively and found that<br />
consolidation was achieved in all cases, without neurologic<br />
deterioration, with anti-tubercular therapy 8 .<br />
In our patient also, good results were seen after nonoperative<br />
treatment. We conclude that Anti Tubercular<br />
Therapy combined with cervical immobilization without need<br />
for surgical intervention is suitable for patients without neural<br />
deficit.<br />
REFERENCES<br />
1. Tuberculosis of the skeletal system. Tuli SM. J.P. Brothers. 3 rd<br />
edition;2004.<br />
2. Hsu LCS, Leong JCY. Tuberculosis of lower cervical spine: a report<br />
of 40 cases. J Bone Joint Surg 1984;66B:1.<br />
3. <strong>Orthopaedic</strong>s. Turek Samuel L. J.P. Brothers, 4 th edition; 1984.<br />
4. Lifeso R. Atlanto-axial tuberculosis in adults. J Bone Joint Surg<br />
1987;69B:183.<br />
5. George W, Wood II, Campbell’s operative orthopaedics. Mosby,<br />
New York 10 th edition; 2003.<br />
6. A.K. Jain, Treatment of tuberculosis of the spine with neurologic<br />
complications, Clin Orthop 398 (2002), 75–84.<br />
7. S.K. Gupta, S. Mohindra, B.S. Sharma, R. Gupta, R. Chhabra and<br />
K.K. Mukherjee et al., Tuberculosis of the craniovertebral junction:<br />
is surgery necessary, Neurosurgery 58 (2006), 1144–1150.<br />
8. M. Chadha, A. Agarwal and A. Pal Singh, Craniovertebral<br />
tuberculosis. A retrospective review of 13 cases managed<br />
conservatively, <strong>Spine</strong> 32 (2007), 1629–1634.<br />
Pb Journal of <strong>Orthopaedic</strong>s Vol-XII, No.1, 2010<br />
33<br />
PDF created with pdfFactory Pro trial version www.pdffactory.com