Fractures of the Distal Radius - Punjab Orthopaedic Association
Fractures of the Distal Radius - Punjab Orthopaedic Association
Fractures of the Distal Radius - Punjab Orthopaedic Association

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>Fractures</strong> <strong>of</strong> <strong>the</strong> distal radius: Current Concepts<br />
P. P. Kotwal MS, Bhavuk Garg MS<br />
Department <strong>of</strong> <strong>Orthopaedic</strong>s, All India Institute <strong>of</strong> Medical Sciences, New Delhi<br />
34<br />
ractures <strong>of</strong> <strong>the</strong> <strong>Distal</strong> radius account for 14% <strong>of</strong> all<br />
extremity fractures and 17% <strong>of</strong> all fractures treated in<br />
F<strong>the</strong> emergency department. As life expectancy<br />
increases, <strong>the</strong> incidence <strong>of</strong> distal radial fractures can be<br />
1<br />
expected to increase as well .<br />
There appears to be a bimodal distribution <strong>of</strong> distal radial<br />
fractures consisting <strong>of</strong> a younger group who sustains<br />
relatively high-energy trauma to <strong>the</strong> upper extremity and an<br />
elderly group who sustains both high-energy injuries and<br />
insufficiency fractures. In older age groups, more women<br />
have fracture <strong>of</strong> <strong>the</strong> distal radius than men. The relationship<br />
between distal end radius fracture and osteoporosis has been<br />
established. Currently, World health organization advises that<br />
a fracture <strong>of</strong> distal end radius in a postmenopausal woman is<br />
an indication for evaluation <strong>of</strong> bone mineral density (BMD).<br />
As <strong>the</strong> population is aging and also activity level <strong>of</strong> older<br />
population is also on increase, <strong>the</strong> presence <strong>of</strong> osteoporosis or<br />
osteopenia places this population at a much higher risk for<br />
2-4<br />
fractures <strong>of</strong> <strong>the</strong> distal radius .<br />
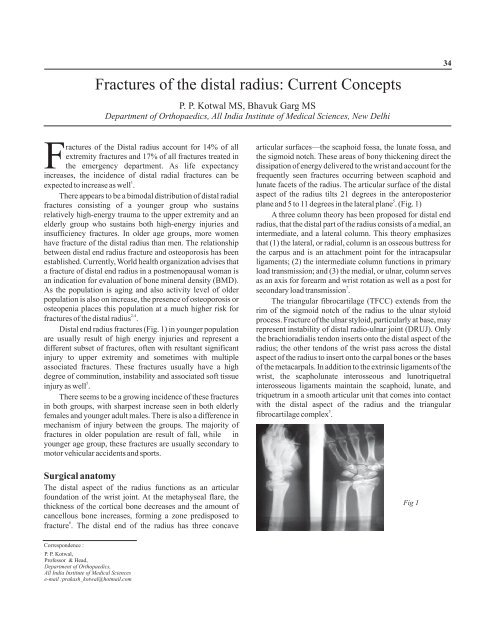
<strong>Distal</strong> end radius fractures (Fig. 1) in younger population<br />
are usually result <strong>of</strong> high energy injuries and represent a<br />
different subset <strong>of</strong> fractures, <strong>of</strong>ten with resultant significant<br />
injury to upper extremity and sometimes with multiple<br />
associated fractures. These fractures usually have a high<br />
degree <strong>of</strong> comminution, instability and associated s<strong>of</strong>t tissue<br />
5<br />
injury as well .<br />
There seems to be a growing incidence <strong>of</strong> <strong>the</strong>se fractures<br />
in both groups, with sharpest increase seen in both elderly<br />
females and younger adult males. There is also a difference in<br />
mechanism <strong>of</strong> injury between <strong>the</strong> groups. The majority <strong>of</strong><br />
fractures in older population are result <strong>of</strong> fall, while in<br />
younger age group, <strong>the</strong>se fractures are usually secondary to<br />
motor vehicular accidents and sports.<br />
Surgical anatomy<br />
The distal aspect <strong>of</strong> <strong>the</strong> radius functions as an articular<br />
foundation <strong>of</strong> <strong>the</strong> wrist joint. At <strong>the</strong> metaphyseal flare, <strong>the</strong><br />
thickness <strong>of</strong> <strong>the</strong> cortical bone decreases and <strong>the</strong> amount <strong>of</strong><br />
cancellous bone increases, forming a zone predisposed to<br />
6<br />
fracture . The distal end <strong>of</strong> <strong>the</strong> radius has three concave<br />
articular surfaces—<strong>the</strong> scaphoid fossa, <strong>the</strong> lunate fossa, and<br />
<strong>the</strong> sigmoid notch. These areas <strong>of</strong> bony thickening direct <strong>the</strong><br />
dissipation <strong>of</strong> energy delivered to <strong>the</strong> wrist and account for <strong>the</strong><br />
frequently seen fractures occurring between scaphoid and<br />
lunate facets <strong>of</strong> <strong>the</strong> radius. The articular surface <strong>of</strong> <strong>the</strong> distal<br />
aspect <strong>of</strong> <strong>the</strong> radius tilts 21 degrees in <strong>the</strong> anteroposterior<br />
5<br />
plane and 5 to 11 degrees in <strong>the</strong> lateral plane . (Fig. 1)<br />
A three column <strong>the</strong>ory has been proposed for distal end<br />
radius, that <strong>the</strong> distal part <strong>of</strong> <strong>the</strong> radius consists <strong>of</strong> a medial, an<br />
intermediate, and a lateral column. This <strong>the</strong>ory emphasizes<br />
that (1) <strong>the</strong> lateral, or radial, column is an osseous buttress for<br />
<strong>the</strong> carpus and is an attachment point for <strong>the</strong> intracapsular<br />
ligaments; (2) <strong>the</strong> intermediate column functions in primary<br />
load transmission; and (3) <strong>the</strong> medial, or ulnar, column serves<br />
as an axis for forearm and wrist rotation as well as a post for<br />
7<br />
secondary load transmission .<br />
The triangular fibrocartilage (TFCC) extends from <strong>the</strong><br />
rim <strong>of</strong> <strong>the</strong> sigmoid notch <strong>of</strong> <strong>the</strong> radius to <strong>the</strong> ulnar styloid<br />
process. Fracture <strong>of</strong> <strong>the</strong> ulnar styloid, particularly at base, may<br />
represent instability <strong>of</strong> distal radio-ulnar joint (DRUJ). Only<br />
<strong>the</strong> brachioradialis tendon inserts onto <strong>the</strong> distal aspect <strong>of</strong> <strong>the</strong><br />
radius; <strong>the</strong> o<strong>the</strong>r tendons <strong>of</strong> <strong>the</strong> wrist pass across <strong>the</strong> distal<br />
aspect <strong>of</strong> <strong>the</strong> radius to insert onto <strong>the</strong> carpal bones or <strong>the</strong> bases<br />
<strong>of</strong> <strong>the</strong> metacarpals. In addition to <strong>the</strong> extrinsic ligaments <strong>of</strong> <strong>the</strong><br />
wrist, <strong>the</strong> scapholunate interosseous and lunotriquetral<br />
interosseous ligaments maintain <strong>the</strong> scaphoid, lunate, and<br />
triquetrum in a smooth articular unit that comes into contact<br />
with <strong>the</strong> distal aspect <strong>of</strong> <strong>the</strong> radius and <strong>the</strong> triangular<br />
5<br />
fibrocartilage complex .<br />
Fig 1<br />
Correspondence :<br />
P. P. Kotwal,<br />
Pr<strong>of</strong>essor & Head,<br />
Department <strong>of</strong> <strong>Orthopaedic</strong>s,<br />
All India Institute <strong>of</strong> Medical Sciences<br />
e-mail :prakash_kotwal@hotmail.com
Pb Journal <strong>of</strong> <strong>Orthopaedic</strong>s Vol-X, No. 1, 2008<br />
<strong>Fractures</strong> <strong>of</strong> <strong>the</strong> <strong>Distal</strong> <strong>Radius</strong>: Current Concepts 35<br />
Classification<br />
A number <strong>of</strong> authors have proposed systems for <strong>the</strong><br />
classification <strong>of</strong> fractures <strong>of</strong> <strong>the</strong> distal aspect <strong>of</strong> <strong>the</strong> radius<br />
including those described by Frykman, Melone, and <strong>the</strong> AO<br />
group. The exact location <strong>of</strong> fracture lines reflected in <strong>the</strong><br />
Frykman classification communicates little useful<br />
information about fracture severity or displacement.<br />
The AO classification is <strong>the</strong> most detailed and inclusive<br />
9<br />
system . AO type-A fractures (extraarticular) are usually<br />
bending injuries through <strong>the</strong> metaphysis, and <strong>the</strong>y do not<br />
affect <strong>the</strong> articular surface <strong>of</strong> ei<strong>the</strong>r <strong>the</strong> radiocarpal or <strong>the</strong><br />
radioulnar joint. AO type-B fractures (partial intraarticular)<br />
result from shear or impaction injuries, causing fractures <strong>of</strong><br />
<strong>the</strong> volar and dorsal rims, fractures <strong>of</strong> <strong>the</strong> radial styloid or<br />
medial corner, or die punch fractures <strong>of</strong> <strong>the</strong> central articular<br />
surface. A portion <strong>of</strong> <strong>the</strong> articular surface remains in<br />
continuity with <strong>the</strong> metaphysis, which adds greatly to <strong>the</strong><br />
stability <strong>of</strong> <strong>the</strong> fracture. AO type-C fractures (complex<br />
articular) are generally high-energy fractures, <strong>of</strong>ten involving<br />
a combination <strong>of</strong> shear and impaction. None <strong>of</strong> <strong>the</strong> articular<br />
surface remains in continuity with <strong>the</strong> metaphysis.<br />
Comminution <strong>of</strong> <strong>the</strong> distal radial metaphysis can be present in<br />
many <strong>of</strong> <strong>the</strong>se injuries. It is defined as involvement <strong>of</strong> >50%<br />
<strong>of</strong> <strong>the</strong> diameter <strong>of</strong> <strong>the</strong> metaphysis as seen on any radiograph,<br />
comminution <strong>of</strong> at least two cortices <strong>of</strong> <strong>the</strong> metaphysis, or<br />
>2.0 mm <strong>of</strong> shortening <strong>of</strong> <strong>the</strong> radius.<br />
5<br />
The Universal Classification <strong>of</strong> distal radial fractures<br />
was proposed in 1990. This system differentiates between<br />
extra-articular and intra-articular fractures, as well as<br />
between stable and unstable fractures; it was created as a<br />
treatment-based algorithm.<br />
Classification Description<br />
I<br />
Nonarticular, nondisplaced<br />
II Nonarticular, displaced<br />
A Reducible, stable<br />
B Reducible, unstable<br />
C Irreducible<br />
III Articular, nondisplaced<br />
IV Articular, displaced<br />
A Reducible, stable<br />
B Reducible, unstable<br />
C Irreducible<br />
D Complex<br />
Table 1: Universal Classification <strong>of</strong> fractures <strong>of</strong> distal end radius<br />
History and Physical Examination<br />
Comprehensive initial evaluation <strong>of</strong> <strong>the</strong> patient who has<br />
sustained a radius fracture is vital to successful treatment. Not<br />
only is <strong>the</strong> mechanism <strong>of</strong> injury important, but <strong>the</strong> patient's<br />
medical and social history also can affect treatment decisions.<br />
A careful physical examination is important as well; <strong>the</strong> initial<br />
evaluator should not be so focused on <strong>the</strong> radius that he or she<br />
underestimates concomitant conditions such as injuries about<br />
<strong>the</strong> elbow or acute neurologic compromise. It is important that<br />
this initial examination includes <strong>the</strong> history <strong>of</strong> <strong>the</strong> injury to<br />
assist in determining <strong>the</strong> degree <strong>of</strong> energy involved. The<br />
carpus should be examined for fractures or fracturedislocations.<br />
Vascular compromise occurs rarely, but<br />
neurological lesions are relatively frequent. Nerve injuries<br />
usually involve <strong>the</strong> median nerve, but can also involve <strong>the</strong><br />
ulnar or radial nerves. If patients do not experience<br />
improvement <strong>of</strong> sensibility after reduction or if sensibility<br />
worsens over serial examinations, one should suspect carpal<br />
tunnel syndrome, investigate accordingly and if confirmed,<br />
5, 10<br />
proceed with an urgent carpal tunnel release .<br />
Radiographic examination<br />
Preoperative planning is <strong>of</strong> vital importance to<br />
successful surgery, and adequate radiographic views <strong>of</strong> <strong>the</strong><br />
wrist are required. Posteroanterior (PA), lateral, and oblique<br />
radiographs <strong>of</strong> <strong>the</strong> injured forearm with wrist should be<br />
obtained. Oblique views reveal intra-articular involvement<br />
that is not apparent on <strong>the</strong> o<strong>the</strong>r views. The semisupinated,<br />
oblique view demonstrates <strong>the</strong> dorsal facet <strong>of</strong> <strong>the</strong> lunate fossa,<br />
whereas <strong>the</strong> partially pronated, oblique PA view allows<br />
5, 11-13<br />
visualization <strong>of</strong> <strong>the</strong> radial styloid .<br />
The fractures <strong>of</strong> <strong>the</strong> distal radius can be associated with<br />
fractures <strong>of</strong> <strong>the</strong> ulna and related ligamentous or bony injuries,<br />
which can be occult, an evaluation <strong>of</strong> <strong>the</strong> s<strong>of</strong>t tissues <strong>of</strong> <strong>the</strong><br />
distal forearm is important. For this assessment, 2 fat planes<br />
on <strong>the</strong> lateral view and 5 fat planes on <strong>the</strong> PA view are useful.<br />
On <strong>the</strong> lateral view, <strong>the</strong> deep fat pad <strong>of</strong> <strong>the</strong> pronator quadratus<br />
and <strong>the</strong> dorsal skin subcutaneous fat line can be seen in<br />
relation to <strong>the</strong> distal radius. The deep fat pad <strong>of</strong> <strong>the</strong> pronator<br />
quadratus forms a slight, ventral concave line. This is<br />
convexly bowed in a ventral direction or completely absent in<br />
pathologic conditions. The dorsal skin subcutaneous fat line is<br />
flat or is a dorsal concave line. It is abnormal when it is convex<br />
in <strong>the</strong> dorsal direction. The PA view shows <strong>the</strong> <strong>the</strong>nar,<br />
hypo<strong>the</strong>nar, pararadial, and paraulnar skin subcutaneous fat<br />
lines and <strong>the</strong> deep, navicular fat pad. Swelling that is not<br />
associated with an observed fracture should initiate a search<br />
for an additional abnormality.
Kotwal et al.<br />
36<br />
Evaluation <strong>of</strong> <strong>the</strong> intra-articular extent <strong>of</strong> <strong>the</strong> fracture is<br />
crucial. Knirk and Jupiter found that 2.0 mm or greater <strong>of</strong><br />
distal radial articular displacement can lead to posttraumatic<br />
14<br />
arthrosis .<br />
Post reduction radiographs help to identify <strong>the</strong> residual<br />
deformity and <strong>the</strong> degree <strong>of</strong> comminution. Standard<br />
posteroanterior traction radiographs help in determining<br />
whe<strong>the</strong>r <strong>the</strong> fracture is intra-articular or extraarticular and<br />
may also demonstrate <strong>the</strong> presence <strong>of</strong> associated<br />
intracapsular or interosseous carpal ligament injuries. The<br />
important radiographic determinations are radial inclination<br />
(23°), radial height (12 mm), volar tilt (11°), reduction <strong>of</strong> <strong>the</strong><br />
distal radioulnar joint, and radial width (normally within 1<br />
11- 13<br />
mm <strong>of</strong> that <strong>of</strong> <strong>the</strong> contralateral side) . Computed<br />
tomography should be performed when conventional<br />
radiographs provide insufficient detail and, specifically, when<br />
a detailed evaluation is needed <strong>of</strong> <strong>the</strong> radiocarpal articular<br />
step-<strong>of</strong>f and gap displacement—factors that are crucial in<br />
predicting <strong>the</strong> development <strong>of</strong> radiocarpal osteoarthritis.<br />
Computerized tomography is also helpful in determining <strong>the</strong><br />
operative approach and <strong>the</strong> fractures <strong>of</strong> <strong>the</strong> lunate facet. CT<br />
scan proves useful in evaluating volar or dorsal displacement<br />
<strong>of</strong> <strong>the</strong> radial styloid process that is not evident on plain<br />
5, 8-9<br />
radiographs, especially if <strong>the</strong> wrist is in a cast.<br />
Management<br />
The fracture pattern, degree <strong>of</strong> displacement <strong>of</strong> <strong>the</strong> fracture<br />
fragments, and stability <strong>of</strong> <strong>the</strong> fracture determine whe<strong>the</strong>r<br />
surgical treatment ra<strong>the</strong>r than immobilization in a cast is<br />
15 16<br />
needed. Trumble et al and Fernandez et al showed that even<br />
step-<strong>of</strong>fs or gaps <strong>of</strong> 1 mm affected outcome. In selecting<br />
treatment, <strong>the</strong>refore, a technique should be used which makes<br />
alignment <strong>of</strong> articular surfaces a priority.<br />
Although restoration <strong>of</strong> palmar tilt to preoperative values is<br />
not critical, restoration to neutral is advised for a number <strong>of</strong><br />
reasons. First, this will more adequately restore radial length<br />
and avoid ulnar impaction or distal radioulnar joint<br />
incongruity. Second, it will prevent subsequent problems with<br />
midcarpal instability. Similarly, correction <strong>of</strong> radial tilt,<br />
although not absolutely critical, will restore more normal<br />
joint mechanics. Radioulnar length, however, must be<br />
restored with little compromise because limitation in<br />
pronation and supination and ulnar impaction are late causes<br />
17-18<br />
<strong>of</strong> pain and impairment .<br />
Closed reduction versus open reduction<br />
<strong>Fractures</strong> with loss <strong>of</strong> 2 mm <strong>of</strong> radial height, change in radial<br />
inclination <strong>of</strong> 5°, loss <strong>of</strong> volar tilt <strong>of</strong> 10°, loss <strong>of</strong> reduction<br />
<strong>of</strong> <strong>the</strong> distal radioulnar joint, and/or those with >1 to 2 mm <strong>of</strong><br />
intra-articular step-<strong>of</strong>f should be reduced. Surgical<br />
intervention is considered when an acceptable reduction<br />
cannot be achieved or maintained by closed means in addition<br />
to achieving an anatomic reduction, establishing stable<br />
fixation to allow early motion and rehabilitation should be <strong>the</strong><br />
5, 8-9<br />
goal .<br />
It is critical that intercarpal intervals and relationships,<br />
<strong>the</strong> carpal bones <strong>the</strong>mselves, and <strong>the</strong> distal radioulnar joint be<br />
assessed on preoperative radiographs and by physical<br />
examination when distal radius fractures are treated.<br />
Scaphoid fractures require internal fixation, if <strong>the</strong><br />
displacement exceeds 1 mm, and scapholunate dissociation<br />
must be anatomically reduced and pinned. <strong>Distal</strong> radioulnar<br />
joint subluxation should not be attributed to radiograph<br />
projection, and its stability must be assessed clinically. If<br />
associated with a displaced ulnar styloid fracture, reduction<br />
and fixation may be necessary to restore stability by <strong>the</strong><br />
insertion <strong>of</strong> <strong>the</strong> triangular fibrocartilage complex (TFCC).<br />
Intercarpal ligamentous injury is common with both<br />
extraarticular and intraarticular distal radius fractures, but in<br />
most cases, <strong>the</strong>se will heal. If intercarpal or ulnar wrist pain<br />
persists after fracture union, however, arthroscopy and/or<br />
magnetic resonance (MR) imaging may be indicated.<br />
A balance <strong>the</strong>n between achieving anatomic reduction,<br />
securing stable fixation, minimizing s<strong>of</strong>t-tissue disruption,<br />
and allowing early rehabilitation should be <strong>the</strong> rationale for<br />
choosing between closed reduction and open reduction.<br />
5, 8-9<br />
Closed reduction<br />
Closed reduction and cast immobilization (Fig 2) is still<br />
<strong>the</strong> mainstay <strong>of</strong> treatment for nondisplaced, stable fractures.<br />
In an attempt to prevent displacement <strong>of</strong> <strong>the</strong> reduced fracture<br />
during immobilization in a splint or plaster cast, placement <strong>of</strong><br />
<strong>the</strong> wrist in <strong>the</strong> extremes <strong>of</strong> positions has been used in <strong>the</strong> past.<br />
This can lead to median nerve compression and stiffness <strong>of</strong><br />
<strong>the</strong> fingers and wrist.<br />
Theoretically, a long arm thumb spica splint with <strong>the</strong><br />
forearm in supination and <strong>the</strong> thumb interphalangeal joint free<br />
is used for <strong>the</strong> first week and changed to a circular cast <strong>the</strong><br />
second and third week. The forearm is supinated to overcome<br />
<strong>the</strong> pull <strong>of</strong> brachioradialis and a thumb spica is worn to<br />
prevent <strong>the</strong> irritation <strong>of</strong> <strong>the</strong> radial sensory nerve by <strong>the</strong> leading<br />
edges <strong>of</strong> <strong>the</strong> cast that do not include <strong>the</strong> thumb. However, in<br />
our practice, thumb spica is not given and we have not seen<br />
any complication related to it. The wrist is maintained in a<br />
neutral position through out treatment. A short arm cast is<br />
worn during weeks 3 through 6. If closed treatment is chosen,<br />
weekly or biweekly radiographs are imperative.
Pb Journal <strong>of</strong> <strong>Orthopaedic</strong>s Vol-X, No. 1, 2008<br />
<strong>Fractures</strong> <strong>of</strong> <strong>the</strong> <strong>Distal</strong> <strong>Radius</strong>: Current Concepts<br />
37<br />
The pins-and-plaster technique, although appealing in<br />
concept, it is <strong>of</strong>ten difficult in practice. Application <strong>of</strong> <strong>the</strong><br />
plaster around <strong>the</strong> pins may prolong <strong>the</strong> procedure<br />
sufficiently to prevent adequate molding <strong>of</strong> <strong>the</strong> cast.<br />
Subsequent dorsal redisplacement and angulation <strong>of</strong> <strong>the</strong> distal<br />
fragment has been one reason that <strong>the</strong> pins-and-plaster<br />
19-22<br />
technique is now infrequently used .<br />
23-28<br />
Percutaneous pinning<br />
Various configurations <strong>of</strong> percutaneously placed pins<br />
have been advocated for <strong>the</strong> stabilization <strong>of</strong> distal radius<br />
fractures. This technique has been used for displaced extraarticular<br />
fractures with or without dorsal comminution, early<br />
loss <strong>of</strong> reduction after closed manipulation, and comminuted<br />
intra-articular fractures when adequate closed reduction is<br />
able to be obtained but likely not maintained without<br />
additional support.<br />
Percutaneous pin fixation is an excellent technique (Fig<br />
2), provided that <strong>the</strong> distal aspect <strong>of</strong> <strong>the</strong> radius is not severely<br />
comminuted or osteoporotic, because <strong>the</strong> trabecular bone <strong>of</strong><br />
<strong>the</strong> metaphysis provides little inherent stability. A variety <strong>of</strong><br />
different techniques have been described in <strong>the</strong> literature.<br />
Kirschner wires can be placed through <strong>the</strong> radial styloid<br />
(trans-styloid), within <strong>the</strong> fracture site (intrafocal), into distal<br />
fragments to aid in reduction, and across <strong>the</strong> distal radioulnar<br />
joint for treatment <strong>of</strong> gross instability <strong>of</strong> <strong>the</strong> distal radioulnar<br />
joint. Ano<strong>the</strong>r method <strong>of</strong> percutaneous pin fixation is <strong>the</strong><br />
intrafocal pin technique <strong>of</strong> Kapandji, which is best reserved<br />
for noncomminuted extraarticular fractures In this technique,<br />
<strong>the</strong> Kirschner wires are introduced into <strong>the</strong> fracture site itself,<br />
ra<strong>the</strong>r than through <strong>the</strong> distal fracture fragment. With severe<br />
comminution in both <strong>the</strong> articular and <strong>the</strong> metaphyseal<br />
region, a combination <strong>of</strong> percutaneous pins, internal fixation,<br />
and external fixation is frequently required in order to<br />
maintain reduction. (Fig 3)<br />
Pins that are used for less than 6 weeks are left protruding<br />
from <strong>the</strong> skin. Pins that are to be left in place longer than 6<br />
5<br />
weeks are buried .<br />
Fig. 3<br />
Fig. 4<br />
Fig. 2<br />
29-39<br />
External Fixation<br />
An external fixation device is <strong>of</strong>ten an important part <strong>of</strong> <strong>the</strong><br />
treatment <strong>of</strong> fractures <strong>of</strong> <strong>the</strong> distal radius. In many instances <strong>of</strong><br />
severe comminution <strong>of</strong> <strong>the</strong> metaphysis, <strong>the</strong> surgeon can<br />
reconstruct <strong>the</strong> articular surface but cannot stabilize it to <strong>the</strong><br />
shaft <strong>of</strong> <strong>the</strong> radius. An external fixation device can allow
Kotwal et al.<br />
38<br />
alignment <strong>of</strong> <strong>the</strong> articular surface with <strong>the</strong><br />
shaft without reliance on support from <strong>the</strong> metaphysis.<br />
External fixation devices are an excellent means <strong>of</strong><br />
overcoming <strong>the</strong> displacing forces <strong>of</strong> <strong>the</strong> forearm muscles that<br />
can pull comminuted distal radial fractures into a collapsed,<br />
shortened position.<br />
Indications for external fixation include:<br />
1. Longitudinal traction for extra-articular fractures<br />
with an unstable metaphysis<br />
2. An indirect reduction assistant during ORIF<br />
3. An adjunct to percutaneous pinning<br />
4. Spanning open fractures<br />
A large variety <strong>of</strong> devices are available for external fixation <strong>of</strong><br />
fractures <strong>of</strong> <strong>the</strong> distal aspect <strong>of</strong> <strong>the</strong> radius. All involve<br />
distraction across <strong>the</strong> wrist joint with placement <strong>of</strong> pins in <strong>the</strong><br />
radius and <strong>the</strong> metacarpals (fig 4). Excessive flexion or ulnar<br />
deviation must be avoided, as ei<strong>the</strong>r position increases <strong>the</strong> risk<br />
<strong>of</strong> compression <strong>of</strong> <strong>the</strong> median nerve, reflex sympa<strong>the</strong>tic<br />
dystrophy, and extrinsic tightness, causing stiffness <strong>of</strong> <strong>the</strong><br />
finger. The ability to position and adjust <strong>the</strong> amount <strong>of</strong> palmar<br />
translation across <strong>the</strong> fracture site with use <strong>of</strong> more<br />
sophisticated external fixation devices provides improved<br />
reduction and allows <strong>the</strong> wrist to be placed in <strong>the</strong> optimal<br />
physiologic position <strong>of</strong> extension. Over distraction is<br />
assessed by observing <strong>the</strong> distance between <strong>the</strong> capitate and<br />
<strong>the</strong> lunate. A gap that is >2 mm indicates that too much force is<br />
being used. Also, <strong>the</strong> fingers should be able to be passively<br />
flexed with ease.<br />
Kirschner-wire augmentation (Fig 3) can substantially<br />
improve stability <strong>of</strong> an unstable extra-articular fracture <strong>of</strong> <strong>the</strong><br />
distal radius regardless <strong>of</strong> <strong>the</strong> type <strong>of</strong> external fixator used.<br />
The addition <strong>of</strong> a dorsal pin in combination with an external<br />
fixation device can easily correct <strong>the</strong> dorsal tilt found in many<br />
fractures <strong>of</strong> <strong>the</strong> distal radius.<br />
Operative Approaches to <strong>Distal</strong> <strong>Radius</strong><br />
Three approaches, two volar and one dorsal, are used most<br />
15<br />
frequently for exposure and fixation <strong>of</strong> <strong>the</strong> distal radius . The<br />
approach chosen is based on <strong>the</strong> configuration <strong>of</strong> <strong>the</strong> fracture<br />
and <strong>the</strong> planned placement <strong>of</strong> fixation.<br />
40-51<br />
Plate fixation<br />
Internal fixation devices and techniques have improved<br />
substantially. The need to fix both large extra-articular<br />
fragments as well as smaller intra-articular fragments is<br />
necessary in many complex fractures. Buttress plates (Fig 5)<br />
have been shown to provide excellent stability for an unstable<br />
fracture with ei<strong>the</strong>r dorsal or volar metaphyseal<br />
comminution. Some designs also provide smaller screws or<br />
pins in <strong>the</strong> transverse distal segment <strong>of</strong> <strong>the</strong> plate, which<br />
facilitates fixation <strong>of</strong> smaller articular fragments. Dorsal<br />
buttress plating was introduced in an attempt to achieve better<br />
control <strong>of</strong> articular reduction and improve stability. Because<br />
most distal radius fractures tend to collapse dorsally, this<br />
technique relies on <strong>the</strong> buttress effect. A disadvantage is that<br />
dorsal plate application alters <strong>the</strong> normal tendon-to-bone<br />
relationship <strong>of</strong> <strong>the</strong> extensors and subjects <strong>the</strong> dorsal tendons<br />
to hardware friction.<br />
Fig 5<br />
S<strong>of</strong>t-tissue complications associated with a dorsal plate,<br />
including extensor tendon irritation and late rupture, have<br />
been attributed to <strong>the</strong> prominence <strong>of</strong> <strong>the</strong> plate and/or screw<br />
heads. Newer designs have minimized <strong>the</strong>se complications<br />
because <strong>the</strong>y incorporate precontouring by <strong>the</strong> manufacturer,<br />
allow ease <strong>of</strong> fur<strong>the</strong>r contouring by <strong>the</strong> surgeon, and use a<br />
plate and screw heads with a low pr<strong>of</strong>ile.<br />
There is a correlation between <strong>the</strong> functional outcome<br />
following a distal radial fracture and <strong>the</strong> restoration <strong>of</strong> both<br />
<strong>the</strong> radiocarpal and <strong>the</strong> radioulnar relationships. However,<br />
<strong>the</strong>y are frequently difficult to restore in osteopenic and
Pb Journal <strong>of</strong> <strong>Orthopaedic</strong>s Vol-X, No. 1, 2008<br />
<strong>Fractures</strong> <strong>of</strong> <strong>the</strong> <strong>Distal</strong> <strong>Radius</strong>: Current Concepts<br />
39<br />
unstable fractures. The development <strong>of</strong> angular stable<br />
fixation techniques with use <strong>of</strong> implants designed specifically<br />
for <strong>the</strong> anatomy <strong>of</strong> <strong>the</strong> distal end <strong>of</strong> <strong>the</strong> radius improves our<br />
ability to manage <strong>the</strong>se problems. In <strong>the</strong>se implants, stability<br />
is not achieved by <strong>the</strong> creation <strong>of</strong> friction between <strong>the</strong> plate<br />
and bone as in traditional screw-plate fixation, but ra<strong>the</strong>r<br />
mechanical bridging <strong>of</strong> <strong>the</strong> bone and load-bearing are allowed<br />
through <strong>the</strong> locked screw-plate construct (Fig 6). Lockinghead<br />
screws do not rely on <strong>the</strong> bone thread for purchase; and<br />
screws that lock into <strong>the</strong> plate prevent loosening within <strong>the</strong><br />
implant, so early failure <strong>of</strong> fixation with an angular stable<br />
implant will occur only if <strong>the</strong> entire screw-plate construct<br />
pulls out from <strong>the</strong> bone or <strong>the</strong>re is material failure <strong>of</strong> <strong>the</strong><br />
implant.<br />
stopped, but before <strong>the</strong> hematoma has consolidated. The<br />
greatest value <strong>of</strong> arthroscopy may be an improved ability to<br />
assess how successful articular restoration has been because it<br />
is becoming increasingly clear that plain radiographs and<br />
fluoroscopy are not always reliable in assessing small<br />
displacements.<br />
Bone graft<br />
During <strong>the</strong> healing process, collapse <strong>of</strong> <strong>the</strong> distal fragments<br />
into <strong>the</strong> cancellous defects in <strong>the</strong> metaphyseal and<br />
subchondral regions can lead to secondary displacement and<br />
55<br />
loss <strong>of</strong> reduction .<br />
Bone graft or bone substitutes are frequently used to fill<br />
<strong>the</strong> metaphyseal void for added support <strong>of</strong> <strong>the</strong> articular<br />
surface during healing. Autogenous bone graft is <strong>the</strong> gold<br />
55<br />
standard , however morbidity associated with harvesting <strong>of</strong><br />
this, has led to use <strong>of</strong> allograft and various bone substitutes.<br />
This area <strong>of</strong> molecular orthopaedics is burgeoning, and<br />
fur<strong>the</strong>r objective, comparative and longer term studies are<br />
required to assist in decision making and finding <strong>the</strong> optimum<br />
bone substitute.<br />
Fig. 6<br />
Biomechanical studies have emphasized <strong>the</strong> need for<br />
placement <strong>of</strong> <strong>the</strong> distal most screws or pegs just beneath <strong>the</strong><br />
subchondral bone <strong>of</strong> <strong>the</strong> articular surface to achieve <strong>the</strong><br />
maximum benefit <strong>of</strong> volar fixed-angle plate fixation.<br />
52-54<br />
Arthroscopic assisted reduction<br />
Advances in arthroscopic technique have added<br />
significantly to our armamentarium for <strong>the</strong> treatment <strong>of</strong> distal<br />
radius fracture. Arthroscopic visualization and reduction<br />
techniques are particularly helpful, for example, in restoring<br />
an incongruous joint surface in <strong>the</strong> setting <strong>of</strong> a single, large,<br />
depressed, radial, styloid fragment. Arthroscopically assisted<br />
reduction and fixation require traction and adequate<br />
visualization. It is advisable; <strong>the</strong>refore, to use this technique<br />
between 4 and 7 days after fracture when bleeding has<br />
5<br />
High energy injuries<br />
High energy trauma to distal radius results in usually a<br />
comminuted fracture pattern and may require a combined<br />
dorsal and volar approach, needing expertise care. These<br />
injuries may result in open fractures and are dealt with<br />
aggressive debridement and stabilization with internal or<br />
external fixation. Ideally s<strong>of</strong>t tissue coverage should be<br />
restored within 1 week <strong>of</strong> injury and bone grafting is done<br />
when s<strong>of</strong>t tissues have healed.<br />
In case <strong>of</strong> closed fractures associated with significant<br />
swelling, it is prudent to wait for <strong>the</strong> swelling to subside and to<br />
delay <strong>the</strong> procedure.<br />
5, 8-9<br />
Associated Injuries<br />
Injuries to distal radioulnar joint (DRUJ) and fracture <strong>of</strong><br />
ulnar styloid are frequently associated with distal radius<br />
fractures. Evaluating <strong>the</strong> stability <strong>of</strong> DRUJ is essential in <strong>the</strong><br />
treatment <strong>of</strong> wrist fractures. If <strong>the</strong> DRUJ is stable, <strong>the</strong> ulnar<br />
head is reduced and is stabilized with K –wires. Associated<br />
fractures <strong>of</strong> ulna also need stabilization. Small avulsion<br />
fractures <strong>of</strong> <strong>the</strong> ulnar styloid process do not necessitate<br />
additional treatment. However, fractures near <strong>the</strong> base <strong>of</strong> <strong>the</strong><br />
ulnar styloid process include <strong>the</strong> entire insertion <strong>of</strong> <strong>the</strong> ulnar<br />
border <strong>of</strong> <strong>the</strong> triangular fibrocartilage complex and need<br />
fixation. Options for fixation include K wires, tension band
Kotwal et al.<br />
40<br />
wiring, mini-screws or Herbert screw fixation.<br />
Intercarpal injuries have also been identified most frequently<br />
in association with fractures involving <strong>the</strong> lunate facet <strong>of</strong> <strong>the</strong><br />
distal articular surface <strong>of</strong> <strong>the</strong> radius. High energy injuries,<br />
especially those involving shearing or avulsion <strong>of</strong> <strong>the</strong> radial<br />
styloid, is frequently associated with Scapho-lunate injuries<br />
and should be treated with pin fixation at least or repaired as<br />
part <strong>of</strong> any open procedure.<br />
Postoperative care and rehabilitation<br />
The goal <strong>of</strong> rehabilitation <strong>the</strong>rapy should be to start patients<br />
on a program <strong>of</strong> active and passive motion <strong>of</strong> <strong>the</strong> digits, elbow,<br />
shoulder, and rotation <strong>of</strong> <strong>the</strong> forearm within twenty-four<br />
hours following surgery. Early motion decreases tendon<br />
adhesions and reduces s<strong>of</strong>t-tissue swelling. Splints and casts<br />
must allow full range <strong>of</strong> motion <strong>of</strong> <strong>the</strong> metacarpophalangeal<br />
joints by not extending beyond <strong>the</strong> distal palmar crease. If<br />
plate fixation is able to provide stable fixation, treatment<br />
involves a short arm cast or splint, and active range-<strong>of</strong> motion<br />
exercises <strong>of</strong> <strong>the</strong> wrist are begun four to six weeks<br />
postoperatively.<br />
5, 8-9<br />
Complications<br />
<strong>Distal</strong> radial fractures are <strong>of</strong>ten associated with poor results<br />
and high complication rates. High-energy fractures,<br />
especially those involving an intra-articular component, are<br />
especially susceptible to poor outcomes. Complications <strong>of</strong><br />
distal radial fractures include compressive neuropathy,<br />
malunion, tendon rupture, radioulnar and radiocarpal<br />
arthrosis, and finger stiffness. Mild forms <strong>of</strong> reflex<br />
sympa<strong>the</strong>tic dystrophy are quite common with distal radial<br />
fractures. Tendon ruptures due to irritation over a plate occur,<br />
but <strong>the</strong>y are infrequent. The extensor pollicis longus and<br />
49<br />
common extensor tendons are most commonly affected . A<br />
prominent dorsal plate and screws cause irritation and<br />
synovitis, which leads to late rupture. O<strong>the</strong>r complications<br />
include flexor or extensor tendon entrapment in <strong>the</strong> fracture or<br />
<strong>the</strong> distal radioulnar joint and <strong>the</strong> development <strong>of</strong> palmar<br />
fascial nodules.<br />
Summary<br />
Intra-articular fractures <strong>of</strong> <strong>the</strong> distal aspect <strong>of</strong> <strong>the</strong> radius are a<br />
heterogeneous group <strong>of</strong> injuries with different fracture<br />
patterns. Treatment <strong>of</strong> displaced fractures <strong>of</strong> <strong>the</strong> distal end <strong>of</strong><br />
<strong>the</strong> radius has changed over <strong>the</strong> course <strong>of</strong> time. Over <strong>the</strong> past<br />
twenty years, more sophisticated internal and external<br />
fixation techniques and devices for <strong>the</strong> treatment <strong>of</strong> displaced<br />
fractures <strong>of</strong> <strong>the</strong> distal end <strong>of</strong> <strong>the</strong> radius have been developed.<br />
The use <strong>of</strong> percutaneous pin fixation; external fixation<br />
devices that permit distraction and palmar translation; lowpr<strong>of</strong>ile<br />
internal fixation plates and implants; arthroscopically<br />
assisted reduction; and bone-grafting techniques, including<br />
bone-graft substitutes, all have contributed to improved<br />
fracture stability and outcome.<br />
We recommend conservative management for<br />
nonarticular, non-displaced fractures. Percutaneous pinning<br />
or ORIF with plate fixation is appropriate for irreducible,<br />
displaced extraarticular fractures. ORIF with buttress plate<br />
fixation remains treatment <strong>of</strong> choice for partial articular<br />
fractures like Barton's fracture. ORIF with locking plate<br />
remains treatment <strong>of</strong> choice for comminuted articular distal<br />
end radius fractures. The accuracy <strong>of</strong> <strong>the</strong> reconstruction <strong>of</strong> <strong>the</strong><br />
articular surface, with <strong>the</strong> goal <strong>of</strong> establishing congruency to<br />
within 1.0 millimeter, is also important in order to minimize<br />
<strong>the</strong> risk <strong>of</strong> late osteoarthritis. Arthroscopic facilities, if<br />
available should be utilized for assessing articular surface<br />
reduction. External fixation remains a useful adjunct for <strong>the</strong><br />
management <strong>of</strong> open fractures and also for indirect reduction<br />
techniques.<br />
Notwithstanding <strong>the</strong> value <strong>of</strong> new devices, however,<br />
appropriate judgment remains critical, especially in choosing<br />
between operative and nonoperative treatment. Indeed, it is<br />
worthwhile acknowledging again <strong>the</strong> relative importance <strong>of</strong><br />
restoring radial length and articular congruity, and yet <strong>the</strong><br />
observation that functional outcome may not correlate with<br />
radiographic appearance.<br />
References:<br />
1. Gellman H. Fracture <strong>of</strong> <strong>the</strong> distal radius. American academy <strong>of</strong><br />
<strong>Orthopaedic</strong> surgeons monograph series. Rosemont. IL, American<br />
academy <strong>of</strong> <strong>Orthopaedic</strong> surgeons, 1998.<br />
2. Cummings SR, Nevitt MC, Browner WS, Stone K, Fox KM, Ensrud<br />
KE, CauleyJ, Black D, Vogt TM. Risk factors for hip fracture in white<br />
women. Study <strong>of</strong> Osteoporotic <strong>Fractures</strong> Research Group. N Engl J<br />
Med. 1995;332:767-73.<br />
3. Schousboe JT, Fink HA, Taylor BC, Stone KL, Hillier TA, Nevitt MC,<br />
Ensrud KE. <strong>Association</strong> between self-reported prior wrist fractures and<br />
risk <strong>of</strong> subsequent hip and radiographic vertebral fractures in older<br />
women: a prospective study. J Bone Miner Res. 2005;20:100-6.<br />
4. Nevitt MC, Cummings SR, Stone KL, Palermo L, Black DM, Bauer<br />
DC, Genant HK, Hochberg MC, Ensrud KE, Hillier TA, Cauley JA.<br />
Risk factors for a first-incident radiographic vertebral fracture in<br />
women > or = 65 years <strong>of</strong> age: <strong>the</strong> study <strong>of</strong> osteoporotic fractures. J<br />
Bone Miner Res. 2005; 20:131-40<br />
5. Hanel DP, Jones MD, Trumble TE. Wrist fractures. Orth clin North Am.<br />
2002; 33: 35-57<br />
6. Dobyns JH, Linscheid RL. <strong>Fractures</strong> and dislocations <strong>of</strong> <strong>the</strong> wrist. In:<br />
Rockwood CA Jr, Green DP, editors. <strong>Fractures</strong> in adults. 2nd ed, volume<br />
1. Philadelphia: JB Lippincott; 1984. p 411-509.<br />
7. Rikli DA, Regazzoni P. <strong>Fractures</strong> <strong>of</strong> <strong>the</strong> distal end <strong>of</strong> <strong>the</strong> radius treated<br />
by internal fixation and early function. A preliminary report <strong>of</strong> 20 cases.<br />
J Bone Joint Surg Br. 1996;78:588-92.
Pb Journal <strong>of</strong> <strong>Orthopaedic</strong>s Vol-X, No. 1, 2008<br />
<strong>Fractures</strong> <strong>of</strong> <strong>the</strong> <strong>Distal</strong> <strong>Radius</strong>: Current Concepts<br />
41<br />
8. Neal C. Chen and Jesse B. Jupiter. Management <strong>of</strong> <strong>Distal</strong> Radial<br />
<strong>Fractures</strong>. J Bone Joint Surg Am. 2007; 89:2051-2062<br />
9. Simic PM and Weiland AJ. <strong>Fractures</strong> <strong>of</strong> <strong>the</strong> <strong>Distal</strong> Aspect <strong>of</strong> <strong>the</strong> <strong>Radius</strong>:<br />
Changes in Treatment over <strong>the</strong> Past Two Decades. J Bone Joint Surg<br />
Am. 2003;85:552-564<br />
10. Cooney WP 3rd, Dobyns JH, Linscheid RL. Complications <strong>of</strong> Colles'<br />
fractures. J Bone Joint Surg Am. 1980;62:613-9<br />
11. Wood MB, Berquist TH. The hand and wrist. In: Berquist TH.<br />
Imaging <strong>of</strong> Orthopedic Trauma. New York, NY: Raven Press;<br />
1992:749-870<br />
12. . Keats TE, Sistrom C. Atlas <strong>of</strong> Radiologic Measurement. 7th ed.<br />
Philadelphia, Pa: Harcourt Health Sciences; 2001:186-99.<br />
13. Greenspan A. Orthopedic Radiology: A Practical Approach.<br />
Philadelphia, Pa: JB Lippincott; 1988:4.3-4.12.<br />
14. Knirk JL, Jupiter JB. Intra-articular fractures <strong>of</strong> <strong>the</strong> distal end <strong>of</strong> <strong>the</strong><br />
radius in young adults. J Bone Joint Surg Am. 1986; 68:647-59.<br />
15. Trumble TE, Culp RW, Hanel DP, Geissler WB, Berger RA. Intraarticular<br />
fractures <strong>of</strong> <strong>the</strong> distal aspect <strong>of</strong> <strong>the</strong> radius. Instr Course Lect.<br />
1999; 48:465-80.<br />
16. Fernandez DL, Geissler WB. Treatment <strong>of</strong> displaced articular<br />
fractures <strong>of</strong> <strong>the</strong> radius. J Hand Surg [Am]. 1991;16:375-84.<br />
17. Taleisnik J, Watson HK: Midcarpal instability caused by Malunited<br />
fractures <strong>of</strong> <strong>the</strong> distal radius. J Hand Surg Am 9:350-257, 1984<br />
18. Pogue DJ, Viegas SF, Patterson RM, et ah Effects <strong>of</strong> distal radius<br />
fracture malunion on wrist joint mechanics. J Hand Surg Am 15:721-<br />
727, 1990<br />
19. Cole JM, Obletz BE. Comminuted fractures <strong>of</strong> <strong>the</strong> distal end <strong>of</strong> <strong>the</strong><br />
radius treated by skeletal transfixion in plaster cast. An end-result study<br />
<strong>of</strong> thirty-three cases. J Bone Joint Surg Am. 1966; 48:931-45.<br />
20. Carrozzella J, Stern PJ. Treatment <strong>of</strong> comminuted distal radius fractures<br />
with pins and plaster. Hand Clin. 1988;4:391-7.<br />
21. Chapman DR, Bennett JB, Bryan WJ, Tullos HS. Complications <strong>of</strong><br />
distal radial fractures: pins and plaster treatment. J Hand Surg [Am].<br />
1982;7:509-12.<br />
22. Green DP. Pins and plaster treatment <strong>of</strong> comminuted fractures <strong>of</strong> <strong>the</strong><br />
distal end <strong>of</strong> <strong>the</strong> radius. J Bone Joint Surg Am. 1975;57:304-10.<br />
23. Habernek H, Weinstabl R, Fialka C, Schmid L. Unstable distal radius<br />
fractures treated by modified Kirschner wire pinning: anatomic<br />
considerations, technique, and results. J Trauma. 1994;36:83-8.<br />
24. Munson GO, Gainor BJ. Percutaneous pinning <strong>of</strong> distal radius<br />
fractures. J Trauma. 1981;21: 1032-5.<br />
25. Naidu SH, Capo JT, Moulton M, Ciccone W 2nd, Radin A.<br />
Percutaneous pinning <strong>of</strong> distal radius fractures: a biomechanical study.<br />
J Hand Surg [Am]. 1997;22:252-7.<br />
26. Rayhack JM. The history and evolution <strong>of</strong> percutaneous pinning <strong>of</strong><br />
displaced distal radius fractures. Orthop Clin North Am. 1993;24:287-<br />
300.<br />
27. Ring D, Jupiter JB. Percutaneous and limited open fixation <strong>of</strong> fractures<br />
<strong>of</strong> <strong>the</strong> distal radius. Clin Orthop. 2000;375:105-15.<br />
28. Rodriguez-Merchan EC. Plaster cast versus percutaneous pin fixation<br />
for comminuted fractures <strong>of</strong> <strong>the</strong> distal radius in patients between 46 and<br />
65 years <strong>of</strong> age. J Orthop Trauma. 1997;11:212-7.<br />
29. Graff S, Jupiter J. Fracture <strong>of</strong> <strong>the</strong> distal radius: classification <strong>of</strong><br />
treatment and indications for external fixation. Injury. 1994;25 Suppl 4:<br />
S-D14-25.<br />
30. Huch K, Hunerbein M, Meeder PJ. External fixation <strong>of</strong> intra-articular<br />
fracture <strong>of</strong> <strong>the</strong> distal radius in young and old adults. Arch Orthop<br />
Trauma Surg. 1996;115:38-42.<br />
31. Jakim I, Pieterse HS, Sweet MB. External fixation for intra-articular<br />
fractures <strong>of</strong> <strong>the</strong> distal radius. J Bone Joint Surg Br. 1991;73:302-6.<br />
32. Pennig D, Gausepohl T. External fixation <strong>of</strong> <strong>the</strong> wrist. Injury.<br />
1996;27:1-15.<br />
33. Riggs SA Jr, Cooney WP 3rd. External fixation <strong>of</strong> complex hand and<br />
wrist fractures. J Trauma.1983;23:332-6.<br />
34. Rikli DA, Kupfer K, Bodoky A. Long-term results <strong>of</strong> <strong>the</strong> external<br />
fixation <strong>of</strong> distal radius fractures. J Trauma. 1998; 44:970-6.<br />
35. Schuind F, Donkerwolcke M, Rasquin C, Burny F. External fixation <strong>of</strong><br />
fractures <strong>of</strong> <strong>the</strong> distal radius: a study <strong>of</strong> 225 cases. J Hand Surg [Am].<br />
1989;14:404-7.<br />
36. Seitz WH Jr, Froimson AI, Leb R, Shapiro JD. Augmented external<br />
fixation <strong>of</strong> unstable distal radius fractures. J Hand Surg [Am].<br />
1991;16:1010-6.<br />
37. Seitz WH Jr. External fixation <strong>of</strong> distal radius fractures. Indications and<br />
technical principles. Orthop Clin North Am. 1993;24:255-64.<br />
38. Simpson NS, Wilkinson R, Barbenel JC, Kinninmonth AW. External<br />
fixation <strong>of</strong> <strong>the</strong> distal radius. A biomechanical study. J Hand Surg [Br].<br />
1994; 19:188-92.<br />
39. Weiland AJ. External fixation, not ORIF, as <strong>the</strong> treatment <strong>of</strong> choice for<br />
fractures <strong>of</strong> <strong>the</strong> distal radius. J Orthop Trauma. 1999;13:570-2.<br />
40. Jupiter JB, Fernandez DL, Toh CL, Fellman T, Ring D. Operative<br />
treatment <strong>of</strong> volar intraarticular fractures <strong>of</strong> <strong>the</strong> distal end <strong>of</strong> <strong>the</strong> radius.<br />
J Bone Joint Surg Am. 1996;78:1817-28.<br />
41. Grewal R, Perey B, Wilmink M, Sto<strong>the</strong>rs K. A randomized prospective<br />
study on <strong>the</strong> treatment <strong>of</strong> intra-articular distal radius fractures: open<br />
reduction and internal fixation with dorsal plating versus mini open<br />
reduction, percutaneous fixation, and external fixation. J Hand Surg<br />
[Am]. 2005;30:764-72.<br />
42. Kreder HJ, Hanel DP, Agel J, McKee M, Schemitsch EH, Trumble TE,<br />
Stephen D. Indirect reduction and percutaneous fixation versus open<br />
reduction and internal fixation for displaced intra-articular fractures <strong>of</strong><br />
<strong>the</strong> distal radius: a randomised, controlled trial. J Bone Joint Surg Br.<br />
2005;87:829-36.<br />
43. Wright TW, Horodyski M, Smith DW. Functional outcome <strong>of</strong> unstable<br />
distal radius fractures: ORIF with a volar fixed-angle tine plate versus<br />
external fixation. J Hand Surg [Am]. 2005;30:289-99.<br />
44. Osada D, Viegas SF, Shah MA, Morris RP, Patterson RM. Comparison<br />
<strong>of</strong> different distal radius dorsal and volar fracture fixation plates: a<br />
biomechanical study. J Hand Surg Am. 2003;28:94-104.<br />
45. Liporace FA, Gupta S, Jeong GK, Stracher M, Kummer F, Egol KA,<br />
Koval KJ. A biomechanical comparison <strong>of</strong> a dorsal 3.5-mm T-plate and<br />
a volar fixed-angle plate in a model <strong>of</strong> dorsally unstable distal radius<br />
fractures. J Orthop Trauma. 2005;19:187-91.<br />
46. Taylor KF, Parks BG, Segalman KA. Biomechanical stability <strong>of</strong> a fixedangle<br />
volar plate versus fragment-specific fixation system: cyclic<br />
testing in a C2-type distal radius cadaver fracture model. J Hand Surg<br />
[Am]. 2006;31:373-81.<br />
47. Kozin SH, Wood MB. Early s<strong>of</strong>t-tissue complications after distal radius<br />
fractures. Instr Course Lect. 1993;42:89-98.<br />
48. Rozental TD, Blazar PE. Functional outcome and complications after<br />
volar plating for dorsally displaced, unstable fractures <strong>of</strong> <strong>the</strong> distal<br />
radius. J Hand Surg [Am]. 2006;31:359-65.<br />
49. Benson EC, DeCarvalho A, Mikola EA, Veitch JM, Moneim MS. Two<br />
potential causes <strong>of</strong> EPL rupture after distal radius volar plate fixation.<br />
Clin Orthop Relat Res. 2006;451:218-22.<br />
50. Kamath AF, Zurakowski D, Day CS. Low-pr<strong>of</strong>ile dorsal plating for<br />
dorsally angulated distal radius fractures: an outcomes study. J Hand<br />
Surg [Am]. 2006; 31:1061-7.<br />
51. Simic PM, Robison J, Gardner MJ, Gelberman RH, Weiland AJ, Boyer<br />
MI. Treatment <strong>of</strong> distal radius fractures with a low-pr<strong>of</strong>ile dorsal plating<br />
system: an outcomes assessment. J Hand Surg [Am]. 2006;31:382-6<br />
52. Geissler WB, Freeland AE. Arthroscopic management <strong>of</strong> intra-articular<br />
distal radius fractures. Hand Clin. 1999;15:455-65<br />
53. Hanker GJ. Diagnostic and operative arthroscopy <strong>of</strong> <strong>the</strong> wrist. Clin<br />
Orthop. 1991; 263:165-74.<br />
54. Wolfe SW, Easterling KJ, Yoo HH. Arthroscopic assisted reduction <strong>of</strong><br />
distal radius fractures. Arthroscopy. 1995; 11:706-14.<br />
55. Ladd AL, Pliam NB. The role <strong>of</strong> bone graft and alternatives in unstable<br />
distal radius fracture treatment. Orthop Clin North Am. 2001; 32:337-<br />
51