A comparative study of tension band wiring and reconstruction ...
A comparative study of tension band wiring and reconstruction ...
A comparative study of tension band wiring and reconstruction ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Original Article<br />
A <strong>comparative</strong> <strong>study</strong> <strong>of</strong> <strong>tension</strong> <strong>b<strong>and</strong></strong> <strong>wiring</strong> <strong>and</strong><br />
<strong>reconstruction</strong> plating in olecranon fractures<br />
Gagan Khanna # , H S Sohal*, R S Boparai**, Devinderpal Singh***<br />
# Assistant Pr<strong>of</strong>essor<br />
Department <strong>of</strong> Orthopedics, Sri Guru Ram Das Institute <strong>of</strong> Medical Sciences, Amritsar<br />
*Pr<strong>of</strong>essor & Head Orthopaedics, ** Pr<strong>of</strong>essor<br />
Department <strong>of</strong> Orthopaedics, GMC, Amritsar<br />
*** Orthopaedic Specialist Officer<br />
Department <strong>of</strong> Orthopaedics, Civil Hospital, Amritsar<br />
ABSTRACT<br />
Olecranon fractures occupy a special role in orthopedic management asthey require accurate reduction <strong>of</strong><br />
fracture <strong>and</strong> a short period <strong>of</strong> immobilization.We present a prospective <strong>study</strong> <strong>of</strong> 30 cases <strong>of</strong> Olecranon<br />
fractures which were divided in two groups. One group was managed by open reduction <strong>and</strong> internal fixation<br />
(ORIF) with <strong>tension</strong> <strong>b<strong>and</strong></strong> <strong>wiring</strong> (TBW) while the second was treated by ORIF with 3.5 mm <strong>reconstruction</strong><br />
plate. Patients <strong>of</strong> each group were graded during their followup for clinical <strong>and</strong> radiological results as per<br />
criteria laid by Rogers et al. The cost effectiveness <strong>of</strong> <strong>tension</strong> <strong>b<strong>and</strong></strong> <strong>wiring</strong> is better to 3.5 mm <strong>reconstruction</strong><br />
plate but comparing the clinical <strong>and</strong> radiological results <strong>of</strong> both the groups the 3.5 mm <strong>reconstruction</strong> plate<br />
shows better clinical <strong>and</strong> radiological statistics than TBW.<br />
Keywords: Olecranon fracture,Tension <strong>b<strong>and</strong></strong> <strong>wiring</strong>, Reconstruction plate<br />
INTRODUCTION<br />
The fracture involving the joint surfaces have always occupied<br />
a special role in orthopedic management since they require an<br />
accurate reduction.Fracture <strong>of</strong> olecranon occurs either as a<br />
direct trauma by theforceful impact at the posterior surface <strong>of</strong><br />
the elbow, or as an indirect trauma due to falling on partially<br />
flexed elbow resulting in avulsion <strong>of</strong> proximal fragment <strong>of</strong> the<br />
olecranondue to the pull <strong>of</strong> triceps muscle. 1<br />
Tension <strong>b<strong>and</strong></strong> <strong>wiring</strong> is a technique developed by AO Group<br />
which is based upon the principle <strong>of</strong> counteracting the tensile<br />
forces acting across the fracture site <strong>and</strong> then converting them<br />
into compressive forces. Two parallel Kirschner wires (K-wires)<br />
across the fracture site before applying the <strong>tension</strong> <strong>b<strong>and</strong></strong> wire<br />
Corresponding Author :<br />
Dr. Gagan Khanna<br />
Department <strong>of</strong> Orthopedics,<br />
Sri Guru Ram Das Institute <strong>of</strong> Medical Sciences,<br />
Vallah, Amritsar-143001.<br />
Email: drgk75@gmail.com<br />
(TBW) improves alignment, prevents rotation <strong>and</strong><br />
provides greater stability. Figure <strong>of</strong> eight wire placed on<br />
posterior surface across the fracture site will produce<br />
compression 2 .Problems <strong>of</strong> wire protrusion <strong>and</strong> pain after TBW<br />
have been reported even without proximal migration <strong>of</strong> the<br />
pins 3,4 .Reconstruction plate is very useful in comminuted or<br />
oblique longitudinal fractures. Tension <strong>b<strong>and</strong></strong> <strong>wiring</strong> in these<br />
fractures results in shortening <strong>of</strong> the olecranon which effects<br />
the articulation with loss <strong>of</strong> motion or impingement. Plate<br />
provides adequate rigidity <strong>and</strong> can be contoured according to<br />
the specific needs <strong>of</strong> fracture configuration which provides<br />
greater strength <strong>and</strong> rigid fixation across the fracture site<br />
permitting early motion <strong>of</strong> joint 5 .<br />
MATERIAL AND METHODS<br />
In this prospective <strong>study</strong>, 30 skeletally mature patients with<br />
closed olecranon fractures were taken who were distributed<br />
alternatively to two groups as<br />
Group A; treated by ORIF with <strong>tension</strong> <strong>b<strong>and</strong></strong> <strong>wiring</strong>.<br />
Group B; treated by ORIF with 3.5 mm <strong>reconstruction</strong><br />
plate.<br />
Pb Journal <strong>of</strong> Orthopaedics Vol-XIII, No.1, 2012<br />
57
Khanna et al<br />
Severely comminuted fractures were given preference for<br />
internal fixation with plate. Cases were classified as per Horne<br />
<strong>and</strong> Tanzer’s Classification 6 (Table-1)<br />
Type-1<br />
Type-2<br />
Type-3<br />
Table 1<br />
Showing the classification <strong>of</strong> Olecranon<br />
Transverse intra-articular fractures on the proximal third<br />
<strong>of</strong> the articular surface <strong>of</strong> the olecranon fossa or oblique<br />
extra-articular fracture <strong>of</strong> the olecranon<br />
Oblique or transverse fractures on the middle third <strong>of</strong> the<br />
articular surface <strong>of</strong> the olecranon fossa.<br />
Oblique or transverse fractures on the middle third<strong>of</strong> the<br />
articular surface <strong>of</strong> the olecranon fossa.<br />
Transverse or oblique fractures on the distal third <strong>of</strong>the<br />
olecranon fossa.<br />
3 rd generation cephalosporins plus aminoglycosides were given<br />
for 72 hours.X-rays were taken on 1 st post-operative dayto<br />
confirm the fixation <strong>and</strong> reduction. Wound site was checked<br />
on 3 rd post-op day. Stitches were removed on 12th post-op<br />
day.<br />
The patients were examined on 3rd, 6th, 9th, 12th week<br />
<strong>and</strong> at six weekly intervals after that. On every visit patients<br />
were examined clinically <strong>and</strong> X-rays <strong>of</strong> the elbow taken in<br />
anteroposterior <strong>and</strong> lateral view. Movements <strong>of</strong> elbow were<br />
recorded. During the period <strong>of</strong> follow up, only active exercises<br />
in physiotherapy centre or at home were advocated.<br />
Every patient <strong>of</strong> each group then is graded during his<br />
follow-up for clinical <strong>and</strong> radiological results as per criteria laid<br />
by Rogers et al 8 . (Table-2)<br />
Surgical steps:<br />
Exposure: General Anesthesia or brachial block was preferred<br />
<strong>and</strong> tourniquet was used in all cases. Posterior midline incision,<br />
extending 2.5 cm proximal <strong>and</strong> 10 cm distal to the olecranon<br />
was usedfor both groups <strong>and</strong> fracture site was exposed 7 .<br />
ORIF with TBW: A hole was drilled transversely in the ulna<br />
about 5-7 cm distal to fracture site. A Stainless steel wire No.20<br />
was passed through this hole. Two parallel 2.00 mm K-wires<br />
were drilled from the tip <strong>of</strong> the olecranon through the proximal<br />
fragment in slight oblique anterior direction to engage the<br />
anterior cortex <strong>of</strong> the distal fragment <strong>of</strong> ulna. The loop <strong>of</strong> wire<br />
was crossed over the posterior surface <strong>of</strong> the olecranon in<br />
figure <strong>of</strong> eight fashion <strong>and</strong> passed around the protruded K-<br />
wires under the triceps tendon. The wire was tightened <strong>and</strong><br />
secured with a twist. Range <strong>of</strong> movements checked. K-wires<br />
were cut <strong>and</strong> bended end was rotated posteriorly <strong>and</strong> impacted<br />
in the olecranon under the triceps. Wound was stitched in<br />
layers <strong>and</strong> was sealed <strong>and</strong> compression <strong>b<strong>and</strong></strong>age applied.<br />
ORIF with 3.5 mm Reconstruction plate: After reduction<br />
<strong>of</strong> fragments, the fracture was temporarily fixed <strong>and</strong> aligned<br />
with 2.00 mm K-wire passed from the tip into the medullary<br />
canal <strong>of</strong> distal ulna. After necessary contouring <strong>of</strong> the plate, it<br />
was applied subperiosteally on the posterior or posteromedial<br />
surface <strong>of</strong> ulna, using 3.5mm cortical <strong>and</strong> 4.0mm cancellous<br />
screws. K-wire was not removed in some cases so as to maintain<br />
the fixation <strong>and</strong> alignment. Wound was closed in layers <strong>and</strong><br />
dressing was applied.<br />
POSTOPERATIVE MANAGEMENT & FOLLOW UP<br />
The operated limb was kept elevated for 48 hours. Intravenous<br />
RESULTS<br />
Table 2<br />
SHOWING BASIS OF GRADING<br />
Grade Loss <strong>of</strong> Loss <strong>of</strong> Union<br />
movement supination <strong>and</strong><br />
at elbow pronation<br />
Excellent
A <strong>comparative</strong> <strong>study</strong> <strong>of</strong> <strong>tension</strong> <strong>b<strong>and</strong></strong> <strong>wiring</strong> <strong>and</strong><br />
<strong>reconstruction</strong> plating in olecranon fractures<br />
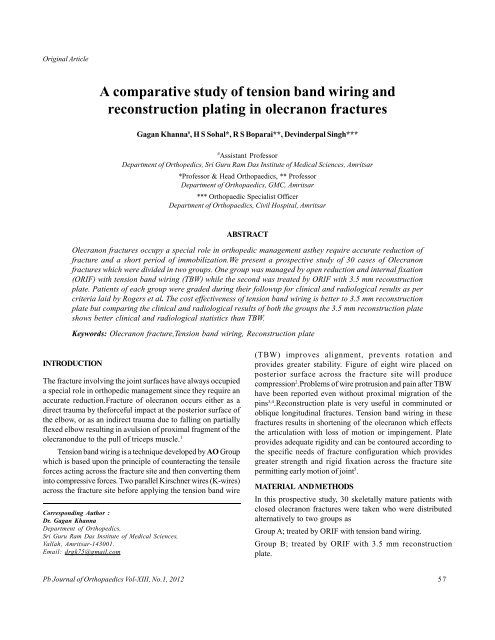
Fig 1. Showing results <strong>of</strong> Group B<br />
Table 3<br />
Showing Complications<br />
Complications Group A Group B<br />
No. <strong>of</strong> cases %age No. <strong>of</strong> cases %age<br />
Superficial infection 2 13.3 1 6.7 3 10.0<br />
Deep infection 1 6.7 - - 1 3.4<br />
Delayed union - - 1 6.7 1 3.4<br />
Non union - - - - - -<br />
Symptomatic metal skin impingement 5 33.3 1 6.7 6 20.0<br />
Implant loosening (plate loosening/ proximal migration) 2 13.3 - - 2 6.7<br />
Implant exposure - - - - - -<br />
Implant failure - - - - - -<br />
Pb Journal <strong>of</strong> Orthopaedics Vol-XIII, No.1, 2012<br />
59
Khanna et al<br />
In group A 2(13.3%) cases had superficial infection as<br />
compare to one (6.6%) case in group B. Group A had 1(6.6%)<br />
deep infection which resulted in loosening <strong>of</strong> K-wires <strong>and</strong> its<br />
proximal migration. This patient was treated with implant removal<br />
after the bone healed, along with I/V antibiotics resulting in<br />
resolution <strong>of</strong> infection. Proximal migration <strong>of</strong> K-wires was<br />
present in two patients, both <strong>of</strong> them belonged to group A.<br />
(Fig 2).<br />
In the present <strong>study</strong> 13 cases (86%) showed excellent <strong>and</strong><br />
good results while 2 cases (13.3%) had unsatisfactory outcome<br />
in group A with TBW as compare to 14 cases (93.3%) showed<br />
excellent <strong>and</strong> good results while only 1 case (6.7%) had<br />
unsatisfactory outcome in with 3.5 mm <strong>reconstruction</strong> plate<br />
fixation (group B). In both the groups, none <strong>of</strong> the patient<br />
showed poor outcome (Table-4).Doursounian et al 13 in 1994<br />
reported 87% cases had good functional results <strong>and</strong> 13% fair<br />
functional results after <strong>tension</strong> <strong>b<strong>and</strong></strong> <strong>wiring</strong> <strong>of</strong> the olecranon<br />
fractures. Hume <strong>and</strong> Wiss 11 showed 79% good <strong>and</strong> fair<br />
results with TBW <strong>and</strong> 91% good <strong>and</strong> fair results with plate<br />
fixation.<br />
Bailey in 2001 reported 88% excellent or good results<br />
after plate fixation <strong>of</strong> displaced fracture <strong>of</strong> the olecranon 14 .<br />
Other studies reported results similar to the present<br />
<strong>study</strong> 15,16,17 .<br />
Fig 2. Showing results in Group A<br />
CONCLUSION<br />
In this <strong>comparative</strong> <strong>study</strong>, radiographic union occurred within<br />
9 to 26 weeks <strong>of</strong> follow-up with no statistical difference in the<br />
average union time in the groups treated with TBW <strong>and</strong> 3.5 mm<br />
<strong>reconstruction</strong> plate at the final follow-up.<br />
Ten patients incurred 13 complications. Patients were<br />
significantly more likely to develop symptomatic metal<br />
prominence after <strong>tension</strong> <strong>b<strong>and</strong></strong> <strong>wiring</strong> then after plate fixation.<br />
Superficial <strong>and</strong> deepinfection was also more common in <strong>tension</strong><br />
Table 4<br />
Showing clinical results according to roger's criteria<br />
Results Group A Group B<br />
No. <strong>of</strong> cases %age No. <strong>of</strong> cases %age<br />
Excellent 8 53.3 10 66.6 19 63.3<br />
Good 5 33.3 4 26.7 9 30.0<br />
Unsatisfactory 2 13.3 1 6.7 2 6.7<br />
Failure - - - -<br />
Total 15 100.0 15 100.0 30 100.0<br />
Pb Journal <strong>of</strong> Orthopaedics Vol-XIII, No.1, 2012<br />
60
A <strong>comparative</strong> <strong>study</strong> <strong>of</strong> <strong>tension</strong> <strong>b<strong>and</strong></strong> <strong>wiring</strong> <strong>and</strong><br />
<strong>reconstruction</strong> plating in olecranon fractures<br />
<strong>b<strong>and</strong></strong> <strong>wiring</strong> then plate fixation. Pin loosening <strong>and</strong> proximal<br />
migration <strong>of</strong> K-wire was also more common with <strong>tension</strong> <strong>b<strong>and</strong></strong><br />
<strong>wiring</strong>. There was no case <strong>of</strong> non-union or failure <strong>of</strong> fixation in<br />
the present <strong>study</strong> in either group. The cost effectiveness <strong>of</strong><br />
<strong>tension</strong> <strong>b<strong>and</strong></strong> <strong>wiring</strong> is better to 3.5 mm <strong>reconstruction</strong> plate<br />
but comparing the clinical <strong>and</strong> radiological results <strong>of</strong> both the<br />
groups the 3.5 mm <strong>reconstruction</strong> plate shows better clinical<br />
<strong>and</strong> radiological statistics than TBW.<br />
REFERENCES<br />
1. Canale ST <strong>and</strong>Beaty JH: Fracture <strong>of</strong> olecranon; Campbell’s<br />
Operative Orthopaedics, 11th editon, 2007;Ch.54.<br />
2. Muller ME, Allgower M, Schneider R <strong>and</strong> Willenegger H. Manual <strong>of</strong><br />
internal fixation, 2 nd Ed., New York, Springer-Verlag, 1970.<br />
3. Wolfgang G, Burke F, Bush D, Parenti J, Perry J <strong>and</strong> LaFolleHe B.<br />
Surgical treatment <strong>of</strong> displaced olecranon fractures by <strong>tension</strong> <strong>b<strong>and</strong></strong><br />
<strong>wiring</strong> technique. J Clin Ortho 1987; 2245, 192-204.<br />
4. Romero JM, Miran A, Jensen CH. Complications <strong>and</strong> re-operation<br />
rate after <strong>tension</strong>-<strong>b<strong>and</strong></strong> <strong>wiring</strong> <strong>of</strong> olecranon fractures. J OrthopSci<br />
2000; 5(4):318-20.<br />
5. King GJ, Lammens HN, Milne AD, Roth JH, Johnson JA. Plate<br />
fixation <strong>of</strong> comminuted olecranon fractures: an invitro<br />
biomechanical <strong>study</strong>. J Shoulder Elbow Surg 1996; 5 (6): 437-41.<br />
6. Horne JG <strong>and</strong> Tanzer TL. Olecranon fractures: A review <strong>of</strong> 100<br />
cases. J Trauma 1981; 21: 469-72.<br />
7. Taylor TKF <strong>and</strong> Scham SM. A posteromedial approach to the<br />
proximal end <strong>of</strong> the ulna for the internal fixation <strong>of</strong> olecranon<br />
fractures. J Trauma 1969; 9: 594-602.<br />
8. Rogers JS, Bennett JB <strong>and</strong> Tullos, HS. Management <strong>of</strong> concomitant<br />
ipsilateral fractures <strong>of</strong> the humerus <strong>and</strong> forearm. J Bone <strong>and</strong> Joint<br />
Surg 1984; 66-A (4): 552.<br />
9. Ring D, Jupiter JB, S<strong>and</strong>ers RW, Mast J, Simpson NS. Transolecranon<br />
fracture-dislocation <strong>of</strong> the elbow. J Orthop Trauma 1997;<br />
11(8):545-50.<br />
10. Baruha RK. Displaced olecranon fractures results <strong>of</strong> TBW without<br />
K-wires. IndOrthop J 1998; 32 (4): 263-65.<br />
11. Hume MC, Wiss DA. Olecranon fractures. A clinical <strong>and</strong> radiographic<br />
comparison <strong>of</strong> <strong>tension</strong> <strong>b<strong>and</strong></strong> <strong>wiring</strong> <strong>and</strong> plate fixation. ClinOrthop<br />
1992; (285):229-35.<br />
12. Fan GF, Wu CC, Shin CH. Olecranon fractures treated with <strong>tension</strong><br />
<strong>b<strong>and</strong></strong> <strong>wiring</strong> techniques—comparisons among three different<br />
configurations. Changgeng Yi XueZaZhi 1993; 16(4):231-8.<br />
13. Doursounian L, Prenot O, Touzard RC. Osteosynthesis by <strong>tension</strong><br />
<strong>b<strong>and</strong></strong> <strong>wiring</strong> <strong>of</strong> displaced fracture <strong>of</strong> the olecranon. Ann Chir 1994;<br />
48 (2): 169-77.<br />
14. Bailey CS, MacDermid J, Patterson SD, King GJ. Outcome <strong>of</strong> plate<br />
fixation <strong>of</strong> olecranon fractures. J Orthop Trauma 2001; 15(8):<br />
542-8.<br />
15. Konig S, Kilga M, Kwasny O. Results <strong>of</strong> plate osteosynthesis in<br />
comminuted fracture <strong>of</strong> the olecranon Unfallchirurg 1990;<br />
93(5):216-20.<br />
16. Akman S, Erturer RE, Tezer M, Tekesin M, Kuzgun U. Long term<br />
results <strong>of</strong> olecranon fracture treated with <strong>tension</strong> <strong>b<strong>and</strong></strong> <strong>wiring</strong><br />
technique. ActaOrthopTraumatolTurc 2002; 36 (5): 401-7.<br />
17. Karlsson MK, Hasserius R, Besjakov J, Karlsson C, Josefsson PO.<br />
Fracture <strong>of</strong> the olecranon: 15-25 years followup <strong>of</strong> 73 patients.<br />
ClinOrthop 2002; 403: 205-12<br />
Pb Journal <strong>of</strong> Orthopaedics Vol-XIII, No.1, 2012<br />
61