Editorial - Punjab Orthopaedic Association
Editorial - Punjab Orthopaedic Association
Editorial - Punjab Orthopaedic Association

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
PUNJAB JOURNAL OF ORTHOPAEDICS(An Official Organ of <strong>Punjab</strong> <strong>Orthopaedic</strong> <strong>Association</strong>Vol. XII, No. - I, December 2011EditorsDr. Ravinder SinghProf. & HeadDeptt. of <strong>Orthopaedic</strong>sGain Sagar Medical College& Hospital, BanurDr. Ravi Kumar GuptaAssociate ProfessorDeptt. of <strong>Orthopaedic</strong>sGovt. Medical College& Hospital, ChandigarhDr. B.S. BrarAssociate ProfessorDeptt. of <strong>Orthopaedic</strong>sGovt. Medical College& Hospital, PatialaCo - EditorsDr. H. S. GillConsultant<strong>Orthopaedic</strong>s SurgeonApollo HospitalLudhianaDr. Harpal Singh SehliAssociate ProfessorDeptt. of <strong>Orthopaedic</strong>sDayanand Medical College& Hospital, LudhianaWebsite : www.punjaborthoassociation.com
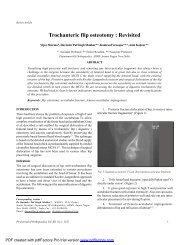
PUNJAB JOURNAL OF ORTHOPAEDICS(An Official Organ of <strong>Punjab</strong> <strong>Orthopaedic</strong> <strong>Association</strong>Vol. XII, No. - I, December 2011Contents<strong>Editorial</strong> Dr. Ravi GuptaArthroplastyTrochanteric flip osteotomy : Revisited 1-4Vijay Sharma, Davinder Pal Singh Makkar, Kamran Farooque, Amit KapoorRole of primary bipolar arthroplasty or total hip arthroplasty for the treatment 5-9of intertrochanteric fracture femur in elderlyJaswinder Pal Singh Walia, Dheeraj Sansanwal, Sonam Kaur Walia, Sargun Singh,Avinash Chander GuptaAcetabuloplasty technique in primary total hip arthroplasty for the dysplastic hip 10-13Wong HC, Ho STTotal knee replacement in osteoarthritis knee with genu varus deformity - 14-17A study of seventy four casesA S Sidhu, B S Brar MS, H S Mann, H S Gill, Gursukhman D S Sidhu, A BassiTwo year follow up in 30 cases of total knee replacement 18-21Jaswinder Pal Singh Walia, Avinash Chander Gupta, Anshul Dahuja,Sonam Kaur Walia, Sargun Singh, Kuldeep SandhuTraumaManagement of distal fracture femur - supracondylar nailing 22-26versus open dynamic condylar screwA S Sidhu, H S Mann, Gursukhman D S Sidhu, A Bassi, A BangaRole of tibial buttress plating in fracture of upper end tibia: A study of 50 cases 27-30J P S Walia, Avinash Gupta, Surinder Kumar, Sonam Kaur Walia, Sargun SinghShoe lace suture technique for management of lower limb diabetic amputations- 31-33A study of 24 casesPankaj Mahindra, J L Bassi, Dhiren Bassi, Mohammad Yamin, Rajneesh Garg,Harpal Singh Selhi, Deepak JainManagement of fracture shaft of humerus - open versus closed antegrade nailing 34-37A S Sidhu, H S Mann, Gursukhman D S Sidhu, A Banga, A Bassi, M Gupta
HandMicrosurgery training in <strong>Orthopaedic</strong>s 38-39WONG H KGiant cell tumor of tendon sheath - A rare case report 40-44Jaswinder Pal Singh Walia, R L Mittal, Avinash Chander Gupta,Girish Sahni, K Kalaivanan, Sargun SinghFailure of fixation in a case of fracture dislocation of interphalangeal joint of 45-48thumb due to planning error: A case reportRavi Gupta, Ashish Chhabra, Amit KumarStudy of clinical problems: Mallet injuries 49-56Dr. Hin-Keung WONGMiscellaneousMorphological classification of tali on the basis of calcanean articular facets 57-60Mandeep Kaur, Gurdeep Kalsey, Vijay LaxmiSciatic-Femoral block for all surgeries below and around knee - ramifications 61-63for orthopaedic surgeon in a compromised set upKandarp Vidyarthi, Sujata Sharma, Rahul Kakran, Vivek Jangira, Hitesh Lal,Rahul Khare, Deepak MittalEffectiveness of transcutaneous electrical nerve stimulation and interferential 64-71electrotherapy in adhesive capsulitisAarti Dewan, Rohit SharmaBurns secondary to improper usage of transcutaneous electrical nerve stimulation: 72-73A case reportMrinalini Sharma, Varun Aggarwal, Raj Bahadur, Ravi Gupta
<strong>Editorial</strong>Improving the trauma care in IndiaAccording to WHO estimates of 2002, road traffic accidents killed over 10 lac people worldwide and injureda further 2-5 crores. Road traffic injuries (RTI) are projected to become the 3rd largest contributor to theglobal disease burden by 2020.In India, RTIs are second frequent cause of public health burden, the first being cardiovascular. A traumarelateddeath is estimated to occur in India every 1.9 minutes. In India, the majority of the victims are pedestrians,two wheeler riders and bicyclists in comparison to the passengers of four wheelers in the developed countries.75-80% victims are 20-44 years old causing an estimated economic loss of 3% gross domestic product (GDP)every year.Ironically, India with 1% global motor vehicles, contributes 6% global road accidents. This is mainly dueto risk factors like unorganized road traffic, alcohol, use of mobile phones and inadequate enforcement oftraffic safety rules. In our licensing system, we do test the road worthiness of a vehicle, but worthiness ofroads is usually neglected by the authorities. All vehicles ply randomly on out highways without earmarkingof lanes. The slow moving vehicles with unlicensed drivers (bicycles, rickshaws, bull carts etc) pose a greaterrisk of accidents.The other important reason of high mortality and morbidity of trauma victims in our country is the lack ofbasic trauma care concept in India. Ambulance services are run by a multitude of organizations includinggovernment, police, fire brigades, hospitals, NGOs, and private agencies. In the absence of guidelines, decisionsabout evacuation of the victim and the choice of the destination hospital are made on an individual basis.Communication in trauma systems is nonexistent. Most of the trauma victims are taken to the public hospitals,thus stressing the already burdened system mostly resulting in delayed treatment of even the already admittedpatients.The problem is multifold which requires a well coordinated action plan at the level of various departmentswhich include police, public health, road & transportation, civil administration and the health department forthe improvements in the standards of the roads, stricter enforcement of the safety standards of vehicles,organization of the traffic including separate roads for the slow moving vehicles, a uniform policy of evictionand on the site first aid and transportation of the patient to a center with standardized facilities of traumacare. Legislative provisions for the minimum qualification and minimum number of ambulance personnel, thetype and quality of ambulance equipment and essential hospital capabilities need to be enacted at the nationallevel.A comprehensive synchronization between public and private health care institutions to evenly distributethe workload may prove to be helpful in improving the medical outcome of trauma victims, where a via mediamay be found to financially support the private institutions to which the trauma victims should be shifted fromgovernment hospitals to decompress the over burdened system of public hospitals.Ravi Gupta MS, DNB, MNAMSAssociate ProfessorDepartment of Orthopedics,Government Medical College Hospital, ChandigarhPb Journal of <strong>Orthopaedic</strong>s Vol-XII, No.1, 2011