Mims et al, Anti elevation syndrome after anterior transposition of the ...
Mims et al, Anti elevation syndrome after anterior transposition of the ...
Mims et al, Anti elevation syndrome after anterior transposition of the ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
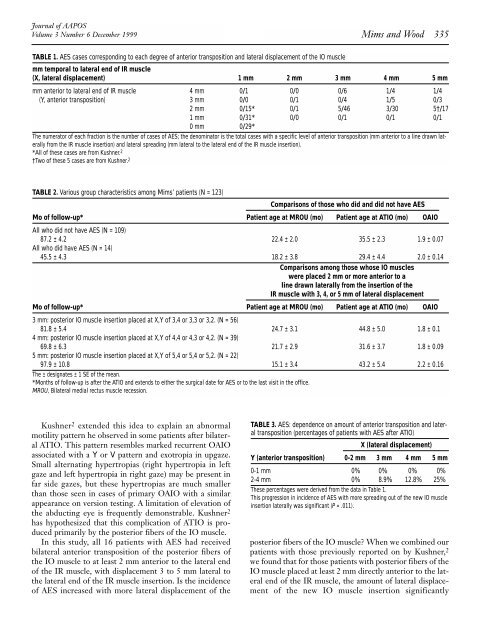
Journ<strong>al</strong> <strong>of</strong> AAPOSVolume 3 Number 6 December 1999<strong>Mims</strong> and Wood 335TABLE 1. AES cases corresponding to each degree <strong>of</strong> <strong>anterior</strong> <strong>transposition</strong> and later<strong>al</strong> displacement <strong>of</strong> <strong>the</strong> IO musclemm tempor<strong>al</strong> to later<strong>al</strong> end <strong>of</strong> IR muscle(X, later<strong>al</strong> displacement) 1 mm 2 mm 3 mm 4 mm 5 mmmm <strong>anterior</strong> to later<strong>al</strong> end <strong>of</strong> IR muscle 4 mm 0/1 0/0 0/6 1/4 1/4(Y, <strong>anterior</strong> <strong>transposition</strong>) 3 mm 0/0 0/1 0/4 1/5 0/32 mm 0/15* 0/1 5/46 3/30 5†/171 mm 0/31* 0/0 0/1 0/1 0/10 mm 0/29*The numerator <strong>of</strong> each fraction is <strong>the</strong> number <strong>of</strong> cases <strong>of</strong> AES; <strong>the</strong> denominator is <strong>the</strong> tot<strong>al</strong> cases with a specific level <strong>of</strong> <strong>anterior</strong> <strong>transposition</strong> (mm <strong>anterior</strong> to a line drawn later<strong>al</strong>lyfrom <strong>the</strong> IR muscle insertion) and later<strong>al</strong> spreading (mm later<strong>al</strong> to <strong>the</strong> later<strong>al</strong> end <strong>of</strong> <strong>the</strong> IR muscle insertion).*All <strong>of</strong> <strong>the</strong>se cases are from Kushner. 2†Two <strong>of</strong> <strong>the</strong>se 5 cases are from Kushner. 2TABLE 2. Various group characteristics among <strong>Mims</strong>’ patients (N = 123)Comparisons <strong>of</strong> those who did and did not have AESMo <strong>of</strong> follow-up* Patient age at MROU (mo) Patient age at ATIO (mo) OAIOAll who did not have AES (N = 109)87.2 ± 4.2 22.4 ± 2.0 35.5 ± 2.3 1.9 ± 0.07All who did have AES (N = 14)45.5 ± 4.3 18.2 ± 3.8 29.4 ± 4.4 2.0 ± 0.14Comparisons among those whose IO muscleswere placed 2 mm or more <strong>anterior</strong> to <strong>al</strong>ine drawn later<strong>al</strong>ly from <strong>the</strong> insertion <strong>of</strong> <strong>the</strong>IR muscle with 3, 4, or 5 mm <strong>of</strong> later<strong>al</strong> displacementMo <strong>of</strong> follow-up* Patient age at MROU (mo) Patient age at ATIO (mo) OAIO3 mm: posterior IO muscle insertion placed at X,Y <strong>of</strong> 3,4 or 3,3 or 3,2. (N = 56)81.8 ± 5.4 24.7 ± 3.1 44.8 ± 5.0 1.8 ± 0.14 mm: posterior IO muscle insertion placed at X,Y <strong>of</strong> 4,4 or 4,3 or 4,2. (N = 39)69.8 ± 6.3 21.7 ± 2.9 31.6 ± 3.7 1.8 ± 0.095 mm: posterior IO muscle insertion placed at X,Y <strong>of</strong> 5,4 or 5,4 or 5,2. (N = 22)97.9 ± 10.8 15.1 ± 3.4 43.2 ± 5.4 2.2 ± 0.16The ± designates ± 1 SE <strong>of</strong> <strong>the</strong> mean.*Months <strong>of</strong> follow-up is <strong>after</strong> <strong>the</strong> ATIO and extends to ei<strong>the</strong>r <strong>the</strong> surgic<strong>al</strong> date for AES or to <strong>the</strong> last visit in <strong>the</strong> <strong>of</strong>fice.MROU, Bilater<strong>al</strong> medi<strong>al</strong> rectus muscle recession.Kushner 2 extended this idea to explain an abnorm<strong>al</strong>motility pattern he observed in some patients <strong>after</strong> bilater<strong>al</strong>ATIO. This pattern resembles marked recurrent OAIOassociated with a Y or V pattern and exotropia in upgaze.Sm<strong>al</strong>l <strong>al</strong>ternating hypertropias (right hypertropia in leftgaze and left hypertropia in right gaze) may be present infar side gazes, but <strong>the</strong>se hypertropias are much sm<strong>al</strong>lerthan those seen in cases <strong>of</strong> primary OAIO with a similarappearance on version testing. A limitation <strong>of</strong> <strong>elevation</strong> <strong>of</strong><strong>the</strong> abducting eye is frequently demonstrable. Kushner 2has hypo<strong>the</strong>sized that this complication <strong>of</strong> ATIO is producedprimarily by <strong>the</strong> posterior fibers <strong>of</strong> <strong>the</strong> IO muscle.In this study, <strong>al</strong>l 16 patients with AES had receivedbilater<strong>al</strong> <strong>anterior</strong> <strong>transposition</strong> <strong>of</strong> <strong>the</strong> posterior fibers <strong>of</strong><strong>the</strong> IO muscle to at least 2 mm <strong>anterior</strong> to <strong>the</strong> later<strong>al</strong> end<strong>of</strong> <strong>the</strong> IR muscle, with displacement 3 to 5 mm later<strong>al</strong> to<strong>the</strong> later<strong>al</strong> end <strong>of</strong> <strong>the</strong> IR muscle insertion. Is <strong>the</strong> incidence<strong>of</strong> AES increased with more later<strong>al</strong> displacement <strong>of</strong> <strong>the</strong>TABLE 3. AES: dependence on amount <strong>of</strong> <strong>anterior</strong> <strong>transposition</strong> and later<strong>al</strong><strong>transposition</strong> (percentages <strong>of</strong> patients with AES <strong>after</strong> ATIO)X (later<strong>al</strong> displacement)Y (<strong>anterior</strong> <strong>transposition</strong>) 0-2 mm 3 mm 4 mm 5 mm0-1 mm 0% 0% 0% 0%2-4 mm 0% 8.9% 12.8% 25%These percentages were derived from <strong>the</strong> data in Table 1.This progression in incidence <strong>of</strong> AES with more spreading out <strong>of</strong> <strong>the</strong> new IO muscleinsertion later<strong>al</strong>ly was significant (P = .011).posterior fibers <strong>of</strong> <strong>the</strong> IO muscle? When we combined ourpatients with those previously reported on by Kushner, 2we found that for those patients with posterior fibers <strong>of</strong> <strong>the</strong>IO muscle placed at least 2 mm directly <strong>anterior</strong> to <strong>the</strong> later<strong>al</strong>end <strong>of</strong> <strong>the</strong> IR muscle, <strong>the</strong> amount <strong>of</strong> later<strong>al</strong> displacement<strong>of</strong> <strong>the</strong> new IO muscle insertion significantly