Anatomy of Inferior Oblique - The Private Eye Clinic
Anatomy of Inferior Oblique - The Private Eye Clinic
Anatomy of Inferior Oblique - The Private Eye Clinic

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
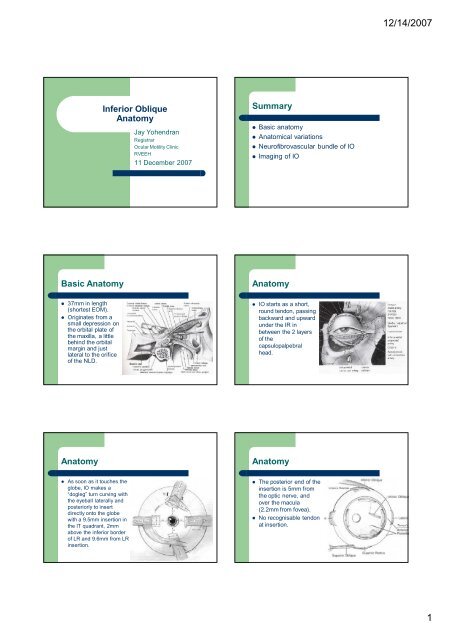
12/14/2007<strong>Inferior</strong> <strong>Oblique</strong><strong>Anatomy</strong>Jay YohendranRegistrarOcular Motility <strong>Clinic</strong>RVEEH11 December 2007Summary Basic anatomy Anatomical variations Neur<strong>of</strong>ibrovascular bundle <strong>of</strong> IO Imaging <strong>of</strong> IOBasic <strong>Anatomy</strong><strong>Anatomy</strong> 37mm in length(shortest EOM). Originates from asmall depression onthe orbital plate <strong>of</strong>the maxilla, a littlebehind the orbitalmargin and justlateral to the orifice<strong>of</strong> the NLD. IO starts as a short,round tendon, passingbackward and upwardunder the IR inbetween the 2 layers<strong>of</strong> thecapsulopalpebralhead.<strong>Anatomy</strong><strong>Anatomy</strong> As soon as it touches theglobe, IO makes a“dogleg” turn curving withthe eyeball laterally andposteriorly to insertdirectly onto the globewith a 9.5mm insertion inthe IT quadrant, 2mmabove the inferior border<strong>of</strong> LR and 9.6mm from LRinsertion. <strong>The</strong> posterior end <strong>of</strong> theinsertion is 5mm fromthe optic nerve, andover the macula(2.2mm from fovea). No recognisable tendonat insertion.1
12/14/2007<strong>Anatomy</strong><strong>Anatomy</strong> Nasal to the IRcrossing, IO is engulfedin orbital fat, is oval inshape with a diameter<strong>of</strong> 4-6mm. Lateral to the crossing itflattens and widens to8-10mm and is coveredby Tenon’s capsule. Between the Tenon’s capsule penetrationand insertion, IO muscle capsule contributesto the intermuscular septum, which providesinterconnection between IR, LR and IO.<strong>Anatomy</strong><strong>Anatomy</strong> <strong>The</strong> inferotemporal vortex vein exits from thesclera at the temporal border <strong>of</strong> IR, 12mmposterior to its insertion, then continues on acircuitous upward course on the innersurface <strong>of</strong> Tenon’s capsule just posterior toIO before penetrating the muscle cone.Unless visualised at the time IO is hooked,the vein may be damaged. IO inclinedposterolaterally at ~45 owith AP plane, almostparallel with SO tendon. <strong>The</strong> nerve and bloodsupply enter the IO inthe undersurface <strong>of</strong> the“dogleg” turn, 15mmfrom the insertion, justlateral to IR.ActionsAnatomical Variations IO elevates the visual axis because itdepresses the posterior aspect <strong>of</strong> the globe. Primary action, elevation, increases inadduction, and is nil in abduction. It is theonly elevator in adduction. Subsidiary actions, abduction and extorsion,increase with abduction and decrease withadduction. Stephen Kraft, Toronto, 1999, Am J Oph 100 cadaver “virgin” orbits:– # <strong>of</strong> divisions at insertion– Variation in anatomy 10 and 12mm from insertion– Total width <strong>of</strong> muscle belly2
12/14/2007Anatomical Variations - KraftAnatomical Variations - Kraft 17 multiple insertions, ranging from 2 to 4 8 had divisions at surgical capture site.Among these 8:– 4 had dehiscences within the muscle that resultedin 2 distinct bellies at 10 and 12mm positions, butthe bellies rejoined at the insertion.– remaining 4 had bifid muscle bellies that insertedseparately into the sclera. Muscle width at 10mm:– 8.4mm in 8 double bellies vs 7.7 in 92 other (notstat sig) Muscle width at 12mm:– 7.8mm vs 7.3 (not stat sig)Anatomical Variations - KraftAnatomical Variations – Kraft 2 <strong>The</strong>se results are for “normal” patients <strong>The</strong> incidence <strong>of</strong> anatomical variations couldbe higher in those with IOOA - ? Doublebellies have greater vertical action Failure to detect duplications at time <strong>of</strong>surgery incomplete weakening andrecurrence/persistence. JAAPOS 2001 – prospective survey over 7years. Compared eyes with double vs single belliedIO muscles:– Gradings <strong>of</strong> pre-op IO & SO actions– Presence <strong>of</strong> fundus excyclotropia– A/V patterns– Presence and size <strong>of</strong> primary positionhypertropias– Post-op IO actionAnatomical Variations – Kraft 2 27 <strong>of</strong> 247 (11%) eyes operated on haddouble bellied IO. Only fundus excyclotorsion incidence differedbetween groups – 48% with double bellies vs27% with single bellies. <strong>The</strong> efficacy <strong>of</strong> weakening surgery inreducing IOOA was similar in both groups.3
12/14/2007Anatomical Variations – Kraft 2Neuro(fibro)vascular bundle <strong>of</strong> IO Bottom-line:– About 10% <strong>of</strong> normals and IOOA have doublebellied IO– If pt has fundus excyclotorsion – look hard for 2bellies, but if no fundus exc doesn’t rule out 2bellies.– No pathognomonic signs that can predict 2bellies. David Stager, Texas,JAAPOS, 1997 Cadaveric eyes andsurgical specimens To investigate why IOanterior transposition<strong>of</strong>ten converts to IO toan “anti-elevator”Neuro(fibro)vascular bundle <strong>of</strong> IONeuro(fibro)vascular bundle <strong>of</strong> IO This study showed that the NFVB has a linear (notcircuitous) course in the orbit. It is 27mm long and extends from the orbital apex tothe midportion <strong>of</strong> IO just temporal to the lateralborder <strong>of</strong> IR. <strong>The</strong> terminal 8mm <strong>of</strong> the nerve lies encased withinsurrounding fibrous tissue bands that attachposteriorly to IR muscle capsule and anteriorly to IOmuscle caspule. <strong>The</strong>se fibrous bands may represent a posteriormodification <strong>of</strong> Lockwood’s ligament into a checkligament that binds the 2 muscles. This study also shows that the NFVB:– Has anatomical and physiological properties likea ligament (it is stiff).– Functions as an ancillary origin for IOImaging <strong>of</strong> IOResults Joseph Demer, Ophthalmology, 2003 Aim: To study the size and contractility <strong>of</strong> thenormal IO using high-res MRI and toevaluate abnormalities <strong>of</strong> SO and IO musclesin chronic SO palsy. Subjects: 13 pts with SO palsy, 17orthotropic pts Methods: 2mm sagittal and coronal imagesrepeated in multiple gaze directions. MRI confirmed ipsilateral decrease in SOsize and contractility in pts with chronic SOpalsy. In all subjects, anterior movement andcontractile thickening <strong>of</strong> IO was observed insupraduction, with posterior movement andrelaxational thinning in infraduction.4
12/14/2007Results But, in pts with chronic unilateral SO palsy,the IO cross-sectional area did not differ fromeither eye, nor from normal subjects. So despite these pts having IO “overaction”,their IO on MRI is not hypertrophied, norexhibits supranormal contractractility. “Overaction in adduction” due to a normal IOfaced with a weak antagonist SO?5