Chronic Kidney Disease (CKD) Algorithm - NHS Cumbria
Chronic Kidney Disease (CKD) Algorithm - NHS Cumbria
Chronic Kidney Disease (CKD) Algorithm - NHS Cumbria

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Chronic</strong> <strong>Kidney</strong> <strong>Disease</strong>(<strong>CKD</strong>) <strong>Algorithm</strong><strong>Chronic</strong> <strong>Kidney</strong> <strong>Disease</strong> (<strong>CKD</strong>) <strong>Algorithm</strong> | Page 1
<strong>Chronic</strong> <strong>Kidney</strong> <strong>Disease</strong> (<strong>CKD</strong>) <strong>Algorithm</strong>(See NICE Clinical Guideline CG73 1 and Quality Standards 2 )Who should have their kidney function checked?• Diabetes (See local Diabetes pathway)• Hypertension• Cardiovascular disease (ischaemic heart disease, chronic heart failure, peripheral vascular andcerebrovascular disease)• Structural renal tract disease, renal calculi or prostatic hypertrophy• Multisystem diseases with potential kidney involvement – e.g. systemic lupus erythematosus• Family history of kidney disease• Opportunistic detection of haematuria or proteinuria• People prescribed nephrotoxic drugs such as calcineurin inhibitors (Ciclosporin, Tacrolimus),Lithium and long term systemic NSAIDsIf none of the above do not use age gender or ethnicity as risk markers.<strong>Chronic</strong> <strong>Kidney</strong> <strong>Disease</strong> (<strong>CKD</strong>) <strong>Algorithm</strong> | Page 1
How should it be done?Measure eGFR• If eGFR in the first test < 60ml/min/1.73m 2 repeat within 14 days to exclude acute kidney injury• To identify progression take at least 3 eGFRs over at least 90 daysAdvise patient not to eat meat for 12 hours prior to eGFR blood test. Cooked meat increases serumcreatinine concentration and affects eGFR calculation. Ensure <strong>CKD</strong> classification is based on samplestaken fasting or when there has been no ingestion of meat.If blood sample taken fasting advise patient to drink water normally.Check urine for Albumin in all at risk groups• Do not rely on reagent strips to identify proteinuria• Use a reagent strip to detect haematuria See Box 8• Send urine for albumin:creatinine ratio (ACR)• If first result is abnormal repeat on an early morning urine sample• In patients with diabetes 2 out of 3 abnormal results confirm albuminuria<strong>Chronic</strong> <strong>Kidney</strong> <strong>Disease</strong> (<strong>CKD</strong>) <strong>Algorithm</strong> | Page 2
First steps & stagingIs there evidence of active renal diseaseor acute kidney injury? See Box 1NOStage the <strong>CKD</strong>YESConsider referral to nephrologist or urologist forinpatient / urgent outpatient assessmentBox 1 - Features of active renaldisease/acute kidney injury• In people aged > 70 years, an eGFR in the range 45–59 ml/min, if stable over time and withoutany other evidence of kidney damage, is unlikely to be associated with <strong>CKD</strong>-related complications• Test eGFR annually in at risk groups, during intercurrent illness and perioperatively in all patientswith <strong>CKD</strong>• Exact frequency depends on the clinical situationStageeGFR ml/in/1.73m 2Stages of <strong>CKD</strong> and frequency of eGFR testingTypical testingfrequency1 > 90 Normal or increased GFR, with other evidence of kidney disease 12 monthly2 60-89 Slight decrease in GFR, with other evidence of kidney disease 12 monthly3A 45-593B 30-444 15-29Moderate decrease in GFR, with or without other evidence ofkidney diseaseModerate decrease in GFR, with or without other evidence ofkidney diseaseSevere decrease in GFR, with or without other evidence ofkidney damage6 monthly6 monthly3 monthly5 < 15 Established renal failure 6 weeklyAre there features that cause particularconcern? e.g.:• Oliguria• Loin pain• Hyperkalaemia (K>7mmol/l)• Severe hypertension• Nephrotic syndrome• Haematoproteinuria (urinalysis in allcases) (NCG 73 page 8)• Lower urinary tract symptoms and signs(dysuria, obstructive symptoms)• Acute systemic symptoms (rash,arthritis, vomiting ,diarrhoea, rigors,confusion)Repeat eGFR within 3 days if any of theabove are present. Refer urgently if eGFRhas fallen by > 5 mL/min.<strong>Chronic</strong> <strong>Kidney</strong> <strong>Disease</strong> (<strong>CKD</strong>) <strong>Algorithm</strong> | Page 3
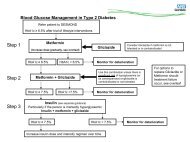
ManagementStages 1 & 2Stages 3A & 3BeGFR > 60 and ACR < 30If no other risk factors for<strong>CKD</strong>, consider normal. Ifrisk factors for <strong>CKD</strong> repeateGFR in 12 monthseGFR > 60 and ACR < 30-69See Box 2Management inPrimary CareeGFR > 30 and < 60ACR > 30 - 69No haematuriaSee Box 2Management inPrimary CareeGFR > 30 and < 60ACR 30 - 69With haematuriaSee Box 2Management inPrimary CareSee Haematuria boxConsider referral for renalspecialist opinionStages 4 & 5AlbuminuriaeGFR < 30Consider referral for renal specialist opinionACR > 70 Irrespective of eGFRConsider referral for renal specialist opinionunless diabetic on appropriate treatment<strong>Chronic</strong> <strong>Kidney</strong> <strong>Disease</strong> (<strong>CKD</strong>) <strong>Algorithm</strong> | Page 4
Management in Primary CareBox 2• Optimise blood pressure control Box 3• Use ACEI/ARBs where indicated Box 4• Reduce cardiovascular disease risk Box 5• Identify progressive <strong>CKD</strong> Box 6• Evaluate albuminuria and haematuriaBox 7 & Box 8• Consider renal ultrasound Box 9• Offer lifestyle advice – exercise, healthyweight and stop smoking• Review medication – avoid NSAIDs andother nephrotoxic agents• Immunisations Box 10• Anaemia Box 11• Potassium Box 12• Bone conditions Box 13• Diabetes Box 14• Refer in a timely manner to a nephrologistBox 15• Refer to appropriately trained professionalfor advice on salt and healthy eating advice.Refer to Community Dietitian for advice onpotassium or any other dietary issue whereappropriate<strong>Chronic</strong> <strong>Kidney</strong> <strong>Disease</strong> (<strong>CKD</strong>) <strong>Algorithm</strong> | Page 5
Box 3 -Optimise bloodpressure control(NCG 73 p13)• Aim to keep bloodpressure below140/90 mmHg in allpatients with <strong>CKD</strong>(target systolic120-139)• Aim to keep BPbelow 130/80 mmHgin people with <strong>CKD</strong>and diabetes orwhen the ACR is >70mg/mmol (targetsystolic 120-129)Box 4 - Use of ACEI/ARBs (NCG 73 p14)• Treat with ACEI first; move to ARBs if ACEIs are not tolerated• Titrate to maximum tolerated dose in all diabetic and nondiabeticpatients with proteinuria• Test eGFR and serum potassium before treatment starts andrepeat after 1- 2 weeks and each dose increment• If eGFR remains stable or shows a small decrease (up to 15%)*continue to titrate dose to maximum• If eGFR decreases 15 - 25%* following introduction or doseincrease:- do not modify dose- repeat the test after 1 – 2 weeks. Continue to titrate dose ifeGFR stable• If eGFR decreases by more than 25% or plasma creatinineincreases more than 30% following ACEI/ARB introduction ordose increase:- investigate for other causes of deterioration in renal function,eg volume depletion due to diuretics or NSAIDs. Considerreferral.• If no other cause: - stop ACEI/ARB therapy or reduce dose to apreviously tolerated lower dose - add alternative antihypertensivemedication if required<strong>Chronic</strong> <strong>Kidney</strong> <strong>Disease</strong> (<strong>CKD</strong>) <strong>Algorithm</strong> | Page 6
Box 5 - Reduce cardiovasculardisease risk• Offer statins for the primary prevention ofcardiovascular disease in the same way asin people without <strong>CKD</strong>• Use statins for the secondary preventionof cardiovascular disease irrespective ofbaseline lipids. Use statins in people withdiabetes (NCG67) 7• Patients with <strong>CKD</strong> are at high risk ofcardiovascular disease. The Framinghamrisk tables significantly underestimate CVrisk. All should be considered for statinstaking into account individual factors• Use antiplatelet drugs for the secondaryprevention of cardiovascular diseaseBox 6 - Identify progressive <strong>CKD</strong>(NCG 73 p5)• Define progressive as a decline in eGFR of>5ml/min per year, or >10ml/min in 5 years- For a new finding of reduced eGFR,repeat test within 2 weeks to excludeacute kidney injury- To identify progression take at least 3eGFRs over at least 90 days- Consider whether progression at theobserved rate would lead to renalreplacement therapy within the person’slifetime• <strong>Chronic</strong> use of NSAIDs may be associatedwith progression; exercise caution andmonitor GFR annually in those taking themlong-term<strong>Chronic</strong> <strong>Kidney</strong> <strong>Disease</strong> (<strong>CKD</strong>) <strong>Algorithm</strong> | Page 7
Evaluate albuminuria and haematuriaBox 7 - AlbuminuriaUrinary protein concentration and approximate equivalent valuesTreatmentACR mg/mmol(albumin:creatinine ratio)PCR mg/mmol(protein:creatinine ration)Urinary protein excretion(g/24hrs)30 50 0.570 100 1No diabetes• ACR < 30 mg/mmol and hypertension: offer a choice of antihypertensive treatment(see NICE guidelines)• ACR > 30 mg/mmol and hypertension: offer ACEI ACR > 30 and < 70 mg/mmol withouthypertension: consider ACEI inhibitor and monitor• ACR > 70 mg/mmol with or without hypertension: offer ACEIDiabetes• ACR > 2.5 (men) with or without hypertension: offer ACEI• ACR > 3.5 (women) with or without hypertension: offer ACEI<strong>Chronic</strong> <strong>Kidney</strong> <strong>Disease</strong> (<strong>CKD</strong>) <strong>Algorithm</strong> | Page 8
Evaluate albuminuria and haematuria (continued)Box 8 - Haematuria (see Joint Consensus Statement 3 )• Use reagent strips• Evaluate further if there is a result of 1+ or more• Confirm persistent invisible haematuria by two out of three positive sticks• Check eGFR in all patients• Do not use urine microscopy to confirm a positive resultRefer to Urology all Patients with• Visible haematuria (any age)• Invisible haematuria associated with lower urinary tract symptoms, if infection excluded (any age)• Asymptomatic invisible haematuria aged > 40 yearsRefer to Nephrology• Patients with rapidly declining renal function (see progressive <strong>CKD</strong> box)• Patients with <strong>CKD</strong> who have had a urological cause excluded• Patients with ACR > 30Monitor in Primary CarePersistent invisible haematuria without proteinuria follow up annually, repeat testing for haematuria,ACR, eGFR and blood pressure as long as the haematuria persists.<strong>Chronic</strong> <strong>Kidney</strong> <strong>Disease</strong> (<strong>CKD</strong>) <strong>Algorithm</strong> | Page 9
Box 9 - Renal Ultrasound(NCG 73 p12)• Offer a renal ultrasound to allpeople with <strong>CKD</strong> who:- have progressive <strong>CKD</strong>- have visible or persistentinvisible haematuria- have lower urinary tractsymptoms- have a family history of polycystickidney disease and are agedover 20yrs- have stage 4 or 5 <strong>CKD</strong>Box 10 - Immunisation• Offer annual influenza vaccinationto all patients with confirmed <strong>CKD</strong>stage 3 (eGFR < 60 ml/min)• Pneumococcal vaccination andrevaccinate according to DHGuidelines (Green Book) 4• Hepatitis B vaccination if there is apossibility of renal replacement• Advise people with a family historyof inherited kidney disease aboutthe implications of an abnormalresult before arranging the scan<strong>Chronic</strong> <strong>Kidney</strong> <strong>Disease</strong> (<strong>CKD</strong>) <strong>Algorithm</strong> | Page 10
Box 11 - Anaemia (NCG 114) 5• Check haemoglobin in people witheGFR < 45 ml/min to identify anaemia• Exclude other causes of anaemia• Consider referral for erythropoietin ifhaemoglobin < 10 g/dl• NICE guidance target haemoglobin forpatients on erythropoietin 10 -12 g/dl.Higher haemoglobins may be harmfulBox 12 - Potassium (NCG 73 p14) 1• Repeat if raised• If > 5.5 mmol/l- do not start ACEI/ARB- exclude other factors that causehyperkalaemia & recheck• If > 6.0 mmol/l and other drugs thatpromote hyperkalaemia have beendiscontinued, stop ACEI/ARBs• If > 7.0 mmol/l, repeat test and referurgently• If taking drugs that causehyperkalaemia, more frequentmonitoring of potassium is required<strong>Chronic</strong> <strong>Kidney</strong> <strong>Disease</strong> (<strong>CKD</strong>) <strong>Algorithm</strong> | Page 11
Box 13 - Manage bone conditions(NCG 73 p13) 1• Measure serum calcium and phosphate ifeGFR < 30ml/min• Seek specialist advice if renal bone diseasesuspected• Do not routinely measure serum calcium,phosphate or parathyroid hormone (PTH) ifeGFR > 30ml/min• Offer bisphosphonates for the prevention andtreatment of osteoporosis where appropriatein patients with eGFR > 30ml/min who are atrisk for other reasons (Manufacturers adviseavoid if eGFR 200mg/mmol despite treatment with maximumdose of ACE inhibitor/ARB• Refer to either diabetologist or nephrologistif blood pressure is difficult to controldespite three agents<strong>Chronic</strong> <strong>Kidney</strong> <strong>Disease</strong> (<strong>CKD</strong>) <strong>Algorithm</strong> | Page 12
ReferralBox 15Referral to a kidney specialist Routine Information required• Take into account theindividual’s wishes andco morbidities whenconsidering referral• People with <strong>CKD</strong> in thefollowing groups shouldnormally be referred forspecialist assessment:Urgent- Suspected Acute <strong>Kidney</strong>Injury- Newly detected eGFR < 15ml/min with symptoms- Nephrotic Syndrome- Accelerated Hypertension- Severe hyperkalaemia(MAU)• Stage 4 and 5 <strong>CKD</strong> (with or withoutdiabetes)• Proteinuria (ACR > 70 mg/mmol) unlessknown to have diabetes and alreadyappropriately treated with ACE Inhibitor orARB Box 14• Proteinuria (ACR > 30 mg/mmol) togetherwith haematuria• Declining eGFR (> 5 ml/min in 1 year, or > 10ml/min within 5 years)• Poorly controlled hypertension despite fourantihypertensive drugs at therapeutic doses• Suspected rare or genetic causes of <strong>CKD</strong>• Suspected renal artery stenosis• Urologically unexplained visible haematuria• Suspected renal anaemia Box 11• Symptoms and Reasonfor referral• Relevant medical andsocial history• Key examinationsfindings includingblood pressure• Serial creatinine / eGFRand urinary albuminresults• Renal ultrasound orother relevant testresult<strong>Chronic</strong> <strong>Kidney</strong> <strong>Disease</strong> (<strong>CKD</strong>) <strong>Algorithm</strong> | Page 13
Key MessagesAll patients with <strong>CKD</strong> have an increased risk of developing heart diseaseand other diseases of blood vessels, including stroke. For many, this ismore important than the risk of developing more serious kidney disease.Knowing that you have <strong>CKD</strong> can help reduce your risk of heart attack byprompting discussion about lifestyle issues and treatment of high bloodpressure and high cholesterol.Patients with advanced, progressive or proteinuric <strong>CKD</strong> require promptspecialist referral.Strict blood pressure control is fundamental in the management of <strong>CKD</strong>.<strong>Kidney</strong> failure accounts for 21% and 11% of deaths in type 1 and 2diabetes respectively.<strong>Chronic</strong> <strong>Kidney</strong> <strong>Disease</strong> (<strong>CKD</strong>) <strong>Algorithm</strong> | Page 14