Diabetes Medical Management Plan (DMMP) Forms
Diabetes Medical Management Plan (DMMP) Forms
Diabetes Medical Management Plan (DMMP) Forms

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
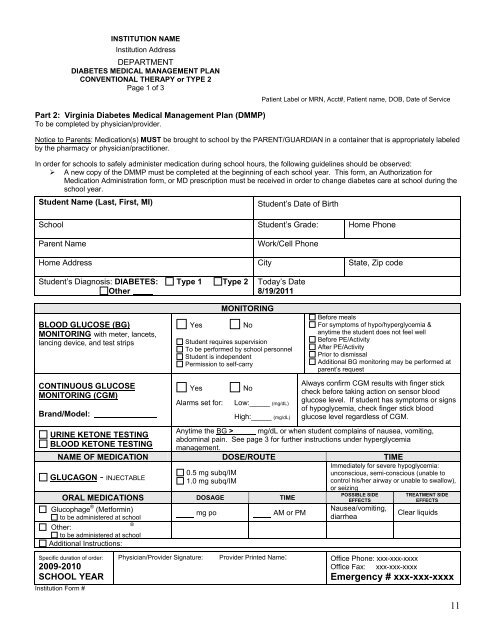
INSTITUTION NAMEInstitution AddressDEPARTMENTDIABETES MEDICAL MANAGEMENT PLANCONVENTIONAL THERAPY or TYPE 2Page 1 of 3Patient Label or MRN, Acct#, Patient name, DOB, Date of ServicePart 2: Virginia <strong>Diabetes</strong> <strong>Medical</strong> <strong>Management</strong> <strong>Plan</strong> (<strong>DMMP</strong>)To be completed by physician/provider.Notice to Parents: Medication(s) MUST be brought to school by the PARENT/GUARDIAN in a container that is appropriately labeledby the pharmacy or physician/practitioner.In order for schools to safely administer medication during school hours, the following guidelines should be observed:‣ A new copy of the <strong>DMMP</strong> must be completed at the beginning of each school year. This form, an Authorization forMedication Administration form, or MD prescription must be received in order to change diabetes care at school during theschool year.Student Name (Last, First, MI)Student’s Date of BirthSchool Student’s Grade: Home PhoneParent NameWork/Cell PhoneHome Address City State, Zip codeStudent’s Diagnosis: DIABETES: Type 1 Type 2OtherToday’s Date8/19/2011BLOOD GLUCOSE (BG)MONITORING with meter, lancets,lancing device, and test stripsYesMONITORINGNoStudent requires supervisionTo be performed by school personnelStudent is independentPermission to self-carryBefore mealsFor symptoms of hypo/hyperglycemia &anytime the student does not feel wellBefore PE/ActivityAfter PE/ActivityPrior to dismissalAdditional BG monitoring may be performed atparent’s requestCONTINUOUS GLUCOSEMONITORING (CGM)Brand/Model:YesAlarms set for:NoLow:_____ (mg/dL)High:_____ (mg/dL)Always confirm CGM results with finger stickcheck before taking action on sensor bloodglucose level. If student has symptoms or signsof hypoglycemia, check finger stick bloodglucose level regardless of CGM.Anytime the BG > mg/dL or when student complains of nausea, vomiting,URINE KETONE TESTINGabdominal pain. See page 3 for further instructions under hyperglycemiaBLOOD KETONE TESTINGmanagement.NAME OF MEDICATION DOSE/ROUTE TIMEImmediately for severe hypoglycemia:0.5 mg subq/IMunconscious, semi-conscious (unable toGLUCAGON - INJECTABLE1.0 mg subq/IMcontrol his/her airway or unable to swallow),or seizingORAL MEDICATIONS DOSAGE TIMEGlucophage ® (Metformin)to be administered at schoolmg poAM or PMOther:®to be administered at schoolAdditional Instructions:POSSIBLE SIDEEFFECTSNausea/vomiting,diarrheaTREATMENT SIDEEFFECTSClear liquidsSpecific duration of order:2009-2010SCHOOL YEARInstitution Form #Physician/Provider Signature: Provider Printed Name: Office Phone: xxx-xxx-xxxxOffice Fax: xxx-xxx-xxxxEmergency # xxx-xxx-xxxx11