Whilst traditionally, the coronary care unit has been thedomain of patients presenting with acute STEMI, with suchpatients now being concentrated in primary PCI (Heart AttackCentres), a unique opportunity has arisen to extend andexpand specialist cardiac care to patients with other acutecardiac complaints who have also been shown to benefit fromcare by cardiology teams. In particular, there is an imperativeto use such a system to provide uniformly high standard careto those with nSTEMI.Crucial to the report was acquisition of reliable data to providethe evidence to support such recommendations. Data fromMINAP regarding management of over 80,000 cases of nSTEMIbetween 2008 and 2009 was used to illustrate the potentialbenefits of dedicated cardiological care in these patients.nSTEMI care may be delivered by general physicians orcardiologists, depending on local protocols or arrangements.MINAP data indicates that those patients admitted under thecare of a cardiologist or to a cardiology unit (encompassingboth coronary care units and dedicated cardiology beds) weremore likely to receive appropriate secondary preventativecardiac medications and were more likely to be referred on forcoronary angiography and subsequent revascularisation. Mostimportantly, those patients under the care of cardiologists in adesignated cardiac unit had significantly lower hospital lengthof stay and were less likely to die within 30 days after their heartattack. The arguments, therefore, for dedicated cardiologicalcare for nSTEMI patients can clearly be made in terms of qualityof care, financial expediency and clinical governance.The Working Group’s report has already been influentialin assisting Trusts where coronary care units had beenthreatened with downgrading or reassignment, and continuesto influence Cardiac Networks across the country in terms ofprovision of equity of evidence-based acute cardiac care.3.3 nSTEMI and access to angiographyThe absence of ST-elevation on the presenting ECG ofthe patient with ACS (nSTEMI) is thought to indicatethat any coronary thrombosis is not totally blocking theaffected coronary artery. As such, immediate coronaryangiography with a view to proceeding straight to PCI orimmediate administration of a powerful thrombolytic drug,is not warranted. Often the event can be managed with acombination of drug treatments.However, some patients with nSTEMI either do not ‘settle’,and continue to suffer ischaemic pain, or initially appear tostabilise but soon afterwards have a further heart attack.Rather than waiting for this to happen patients can beassessed within hours of admission to hospital using a variety16. Gale CP, Manda SO, Weston CF, Birkhead JS, Batin PD, Hall AS. Evaluation ofrisk scores for risk stratification of acute coronary syndromes in the <strong>Myocardial</strong>Infarction <strong>National</strong> <strong>Audit</strong> <strong>Project</strong> (MINAP) database. Heart. 2009;95:221-7.of validated risk scores 16 . For those of at least moderate risk,a policy of routine early angiography (and revascularisationwhere possible) appears to prevent more heart attacks andreadmissions to hospital than medical treatment alone.The 2009 NICE Guideline, that used MINAP data to model theimplications of its recommendations, suggested that ACSpatients at moderate risk, and those in whom it is possibleto demonstrate residual ischaemia on testing after the acuteevent (evidence of persisting narrowing of a coronary artery),should be advised to have a coronary angiogram within 96hours of admission. Other international guidelines haveencouraged even earlier angiography, if only to reduce theoverall length of stay in hospital.The percentage of patients with a final diagnosis of nSTEMI(broadly reflecting the NICE classification of moderate severity)who have angiography during the admission has increasedfrom just over 30% in 2003 to 76% in 2011/12 – as significanta change in management as the development of primary PCIfor STEMI. However, angiography is not appropriate for allpatients with nSTEMI and those at the very highest risk werenot included in trials that demonstrated the benefit of routineangiography. So, there is no nationally agreed standard for theproportion of patients that should undergo angiography.3.4 Of broken hearts and octopus potsWith increasing use of coronary angiography during the earlymanagement of heart attack it has become apparent thatabout 2% of patients admitted to hospital with features ofacute myocardial infarction have a condition called TakotsuboCardiomyopathy – also known as Stress Cardiomyopathy,Apical Ballooning Syndrome and Broken Heart Syndrome. This14 MINAP How the NHS cares for patients with heart attack
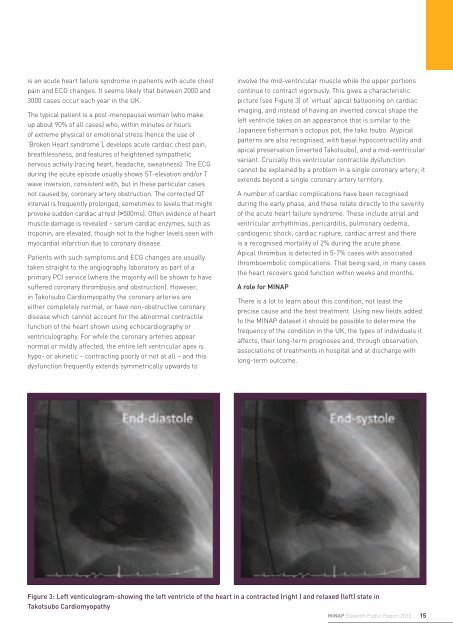
is an acute heart failure syndrome in patients with acute chestpain and ECG changes. It seems likely that between 2000 and3000 cases occur each year in the UK.The typical patient is a post-menopausal woman (who makeup about 90% of all cases) who, within minutes or hoursof extreme physical or emotional stress (hence the use of‘Broken Heart syndrome’), develops acute cardiac chest pain,breathlessness, and features of heightened sympatheticnervous activity (racing heart, headache, sweatiness). The ECGduring the acute episode usually shows ST-elevation and/or Twave inversion, consistent with, but in these particular casesnot caused by, coronary artery obstruction. The corrected QTinterval is frequently prolonged, sometimes to levels that mightprovoke sudden cardiac arrest (>500ms). Often evidence of heartmuscle damage is revealed – serum cardiac enzymes, such astroponin, are elevated, though not to the higher levels seen withmyocardial infarction due to coronary disease.Patients with such symptoms and ECG changes are usuallytaken straight to the angiography laboratory as part of aprimary PCI service (where the majority will be shown to havesuffered coronary thrombosis and obstruction). However,in Takotsubo Cardiomyopathy the coronary arteries areeither completely normal, or have non-obstructive coronarydisease which cannot account for the abnormal contractilefunction of the heart shown using echocardiography orventriculography. For while the coronary arteries appearnormal or mildly affected, the entire left ventricular apex ishypo- or akinetic – contracting poorly or not at all – and thisdysfunction frequently extends symmetrically upwards toinvolve the mid-ventricular muscle while the upper portionscontinue to contract vigorously. This gives a characteristicpicture (see Figure 3) of ‘virtual’ apical ballooning on cardiacimaging, and instead of having an inverted conical shape theleft ventricle takes on an appearance that is similar to theJapanese fisherman’s octopus pot, the tako tsubo. Atypicalpatterns are also recognised, with basal hypocontractility andapical preservation (inverted Takotsubo), and a mid-ventricularvariant. Crucially this ventricular contractile dysfunctioncannot be explained by a problem in a single coronary artery; itextends beyond a single coronary artery territory.A number of cardiac complications have been recognisedduring the early phase, and these relate directly to the severityof the acute heart failure syndrome. These include atrial andventricular arrhythmias, pericarditis, pulmonary oedema,cardiogenic shock, cardiac rupture, cardiac arrest and thereis a recognised mortality of 2% during the acute phase.Apical thrombus is detected in 5-7% cases with associatedthromboembolic complications. That being said, in many casesthe heart recovers good function within weeks and months.A role for MINAPThere is a lot to learn about this condition, not least theprecise cause and the best treatment. Using new fields addedto the MINAP dataset it should be possible to determine thefrequency of the condition in the UK, the types of individuals itaffects, their long-term prognoses and, through observation,associations of treatments in hospital and at discharge withlong-term outcome.Figure 3: Left venticulogram-showing the left ventricle of the heart in a contracted (right ) and relaxed (left) state inTakotsubo CardiomyopathyMINAP Eleventh Public Report 201215
- Page 1 and 2: Myocardial IschaemiaNational Audit
- Page 3 and 4: Myocardial Ischaemia National Audit
- Page 5 and 6: ForewordThe annual MINAP Report, no
- Page 7 and 8: Patients who received thrombolytic
- Page 9 and 10: considering such factors as the age
- Page 11 and 12: egarding previous medical history.
- Page 13: 3. Improving quality,improving outc
- Page 17 and 18: Alan KeysMINAP Steering Group patie
- Page 19 and 20: Figure 7. Patients admitted with a
- Page 21 and 22: Figure 11. Percentage of patients w
- Page 23 and 24: transfers require a significant amo
- Page 25 and 26: Table 8 shows the performance of th
- Page 27 and 28: This year we report on the interval
- Page 29 and 30: Conquest Hospital, St Leonards onSe
- Page 31 and 32: Royal Derby Hospital, Derby 62 89%
- Page 33 and 34: “During times of financial constr
- Page 35 and 36: Broomfield Hospital, Chelmsford 0 0
- Page 37 and 38: Leighton Hospital, Crewe 43 86% 49
- Page 39 and 40: Royal Preston Hospital, Preston 48
- Page 41 and 42: Wycombe Hospital, High Wycombe 11 1
- Page 43 and 44: “I know that MINAP data has been
- Page 45 and 46: Cheltenham General Hospital, Chelte
- Page 47 and 48: Manchester Royal Infirmary, Manches
- Page 49 and 50: Salford Royal Hospital, Manchester
- Page 51 and 52: “MINAP, and its long history, is
- Page 53 and 54: Table 6: Ambulance Services in Engl
- Page 55 and 56: Bradford Royal Infirmary, Bradford
- Page 57 and 58: Hexham General Hospital, Hexham 17
- Page 59 and 60: Papworth Hospital, Cambridge 560 99
- Page 61 and 62: Salisbury District Hospital, Salisb
- Page 63 and 64: West Middlesex University Hospital,
- Page 65 and 66:
“We have participated in MINAP fr
- Page 67 and 68:
Dorset Cardiac and Stroke Network 7
- Page 69 and 70:
“Participation in MINAP has helpe
- Page 71 and 72:
Blackpool Victoria Hospital, Blackp
- Page 73 and 74:
Harefield Hospital 139 84% 156 94%
- Page 75 and 76:
Northern General Hospital, Sheffiel
- Page 77 and 78:
Royal Victoria Infirmary, Newcastle
- Page 79 and 80:
Warrington Hospital, Warrington 435
- Page 81 and 82:
Withybush General Hospital, Haverfo
- Page 83 and 84:
Part Three: Case Studies1. Call act
- Page 85 and 86:
3. Implementing a high-risk nSTEACS
- Page 87 and 88:
The British Heart Foundation is a r
- Page 89 and 90:
of six individual criteria - all in
- Page 91 and 92:
9. Use of MINAP data to develop and
- Page 93 and 94:
Figure 26. Part 2 collected by Card
- Page 95 and 96:
12. Shifting the FocusNicola Mannin
- Page 97 and 98:
Figure 29. Funnel plot of hospital
- Page 99 and 100:
Figure 30. Estimated excess risk of
- Page 101 and 102:
Part 6: AppendicesAppendix 1: MINAP
- Page 103 and 104:
Coronary thrombosisThe formation of
- Page 105 and 106:
Birkhead J, Walker L. MINAP, a proj
- Page 107:
Heart attacks recorded in MINAP in