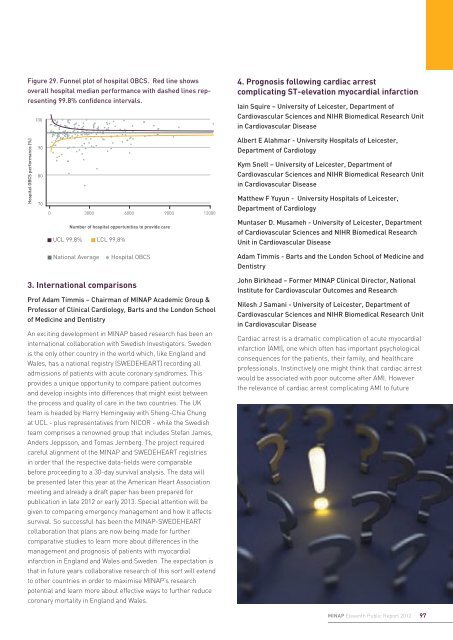
Part 4: Research use of MINAP data1. OverviewProf Adam Timmis – Chairman of MINAP AcademicGroup & Professor of Clinical Cardiology, Barts and theLondon School of Medicine and DentistryLucia Gavalova – MINAP <strong>Project</strong> ManagerMINAP now has over 1 million records with almost 100%hospital participation since 2003, making it the largestcollection of ACS data in the world covering most of thepatient population in England and Wales. As such it is aninvaluable research resource for observational studies.The MINAP Academic Group was delegated responsibility bythe Health Quality Improvement Partnership (HQIP) to releaseits audit data to external researchers. Research applicationsare considered by the MINAP Academic Group, and if approvalis given the data fields required for the research are madeavailable. Some preference is given to those researcherswith a track record and experience in working with large andcomplex datasets. More recently, the NICOR Research Grouphas been set up to oversee research strategy across all thedatasets under its custodianship.When NICOR was established in 2011, it facilitated the linkageof the national cardiovascular audits providing researcherswith a unique resource for tracking patients through theircardiovascular journey. MINAP has also been linked withCPRD (Clinical Practice Research Database) to explore patientcare before and after a heart attack..Vital status is updated annually by the Office of <strong>National</strong>Statistics. Researchers only have access to anonymised data.This is in compliance with the strict governance rules thatensure patient confidentiality.The MINAP Academic Group welcomes applications fromMINAP hospitals that are interested in regional or nationalanalyses that seek answers to valid research questions,and are able to facilitate collaborations with experiencedacademics and statisticians.To date, over 35 publications have resulted from the useof MINAP data and more projects are currently on-goingfollowing an approval by the MINAP Academic Group. Thefollowing sections highlight just a few that were published inthe last year or so.2. Evaluation of a composite performanceindicator in the assessment of hospitals care forpatients after a heart attack, MINAP 2008 to 2009.Dr Alex Simms - Cardiology Specialist RegistrarDr Chris Gale - Consultant CardiologistCentre for Epidemiology and Biostatistics, <strong>University</strong> of LeedsMINAP reports hospital performance – the care providedat each hospital to patients admitted there – in terms of anumber of different indicators of good quality care. Each ofthese indicators identifies one intervention, among many,that has been shown to improve the outcome for patientsexperiencing heart attack. We used data from MINAP to designand study a summary or composite score of how hospitalsprovided a number of these previously described singlemeasures. We advocate summary scores rather than singleindicators of care (such as “did all patients receive aspirin ondischarge”) because they measure achievements across awider range of care. Our indicator was an opportunity-basedcomposite score (OBCS) designed to be incorporate data frompatients discharged from hospital following a heart attack.The score measured all the fulfilled opportunities a hospitalhad to provide a care process, expressed as a percent. Thecare processes we used were the prescription of aspirin,thienopyridine inhibitors, β-blocker, ACE inhibitor and statin,as well as referral for cardiac rehabilitation.We found that, overall, 95% of opportunities to provide carewere achieved. This varied between hospitals in Englandand Wales – ranging from 76% to 100% across 199 acutehospitals. A funnel plot of hospital OBCS allowed visualisationof this variation between hospital (Figure 29). We also foundthat the OBCS more readily highlighted hospitals (24%)that needed to improve their performance, than using theindividual components of the OBCS, and that it showed greaterconsistency in identifying lower performing hospitals.Importantly, our study demonstrated that the OBCS had asignificant inverse relationship with death at 30-days and at6-months. It showed that better performing hospitals hadlower mortality rates. This effect persisted despite adjustmentfor differences in patient characteristics and the performanceof coronary artery catheterisation. Each percentage increasein hospital OBCS was associated with, on average, a 3% and2% decline in 30-day and 6-month death rate, respectively.In conclusion, our study found that the OBCS offered a summaryof hospital care for patients with heart attack, discriminatedhospital performance and was linked with longer-termoutcomes. The OBCS may therefore be suitable for inclusion inhospital quality-improvement strategies and for the comparisonof hospital performance in England and Wales.96 MINAP How the NHS cares for patients with heart attack
Figure 29. Funnel plot of hospital OBCS. Red line showsoverall hospital median performance with dashed lines representing99.8% confidence intervals.1004. Prognosis following cardiac arrestcomplicating ST-elevation myocardial infarctionIain Squire – <strong>University</strong> of Leicester, Department ofCardiovascular Sciences and NIHR Biomedical Research Unitin Cardiovascular DiseaseHospital OBCS performance (%)9080700 3000 6000 9000 12000Number of hospital opportunities to provide careUCL 99.8% LCL 99.8%Albert E Alahmar - <strong>University</strong> Hospitals of Leicester,Department of CardiologyKym Snell – <strong>University</strong> of Leicester, Department ofCardiovascular Sciences and NIHR Biomedical Research Unitin Cardiovascular DiseaseMatthew F Yuyun - <strong>University</strong> Hospitals of Leicester,Department of CardiologyMuntaser D. Musameh - <strong>University</strong> of Leicester, Departmentof Cardiovascular Sciences and NIHR Biomedical ResearchUnit in Cardiovascular Disease<strong>National</strong> AverageHospital OBCSAdam Timmis - Barts and the London School of Medicine andDentistry3. International comparisonsProf Adam Timmis – Chairman of MINAP Academic Group &Professor of Clinical Cardiology, Barts and the London Schoolof Medicine and DentistryAn exciting development in MINAP based research has been aninternational collaboration with Swedish Investigators. Swedenis the only other country in the world which, like England andWales, has a national registry (SWEDEHEART) recording alladmissions of patients with acute coronary syndromes. Thisprovides a unique opportunity to compare patient outcomesand develop insights into differences that might exist betweenthe process and quality of care in the two countries. The UKteam is headed by Harry Hemingway with Sheng-Chia Chungat UCL - plus representatives from NICOR - while the Swedishteam comprises a renowned group that includes Stefan James,Anders Jeppsson, and Tomas Jernberg. The project requiredcareful alignment of the MINAP and SWEDEHEART registriesin order that the respective data-fields were comparablebefore proceeding to a 30-day survival analysis. The data willbe presented later this year at the American Heart Associationmeeting and already a draft paper has been prepared forpublication in late 2012 or early 2013. Special attention will begiven to comparing emergency management and how it affectssurvival. So successful has been the MINAP-SWEDEHEARTcollaboration that plans are now being made for furthercomparative studies to learn more about differences in themanagement and prognosis of patients with myocardialinfarction in England and Wales and Sweden. The expectation isthat in future years collaborative research of this sort will extendto other countries in order to maximise MINAP’s researchpotential and learn more about effective ways to further reducecoronary mortality in England and Wales.John Birkhead – Former MINAP Clinical Director, <strong>National</strong>Institute for Cardiovascular Outcomes and ResearchNilesh J Samani - <strong>University</strong> of Leicester, Department ofCardiovascular Sciences and NIHR Biomedical Research Unitin Cardiovascular DiseaseCardiac arrest is a dramatic complication of acute myocardialinfarction (AMI), one which often has important psychologicalconsequences for the patients, their family, and healthcareprofessionals. Instinctively one might think that cardiac arrestwould be associated with poor outcome after AMI. Howeverthe relevance of cardiac arrest complicating AMI to futureMINAP Eleventh Public Report 201297
- Page 1 and 2:
Myocardial IschaemiaNational Audit
- Page 3 and 4:
Myocardial Ischaemia National Audit
- Page 5 and 6:
ForewordThe annual MINAP Report, no
- Page 7 and 8:
Patients who received thrombolytic
- Page 9 and 10:
considering such factors as the age
- Page 11 and 12:
egarding previous medical history.
- Page 13 and 14:
3. Improving quality,improving outc
- Page 15 and 16:
is an acute heart failure syndrome
- Page 17 and 18:
Alan KeysMINAP Steering Group patie
- Page 19 and 20:
Figure 7. Patients admitted with a
- Page 21 and 22:
Figure 11. Percentage of patients w
- Page 23 and 24:
transfers require a significant amo
- Page 25 and 26:
Table 8 shows the performance of th
- Page 27 and 28:
This year we report on the interval
- Page 29 and 30:
Conquest Hospital, St Leonards onSe
- Page 31 and 32:
Royal Derby Hospital, Derby 62 89%
- Page 33 and 34:
“During times of financial constr
- Page 35 and 36:
Broomfield Hospital, Chelmsford 0 0
- Page 37 and 38:
Leighton Hospital, Crewe 43 86% 49
- Page 39 and 40:
Royal Preston Hospital, Preston 48
- Page 41 and 42:
Wycombe Hospital, High Wycombe 11 1
- Page 43 and 44:
“I know that MINAP data has been
- Page 45 and 46: Cheltenham General Hospital, Chelte
- Page 47 and 48: Manchester Royal Infirmary, Manches
- Page 49 and 50: Salford Royal Hospital, Manchester
- Page 51 and 52: “MINAP, and its long history, is
- Page 53 and 54: Table 6: Ambulance Services in Engl
- Page 55 and 56: Bradford Royal Infirmary, Bradford
- Page 57 and 58: Hexham General Hospital, Hexham 17
- Page 59 and 60: Papworth Hospital, Cambridge 560 99
- Page 61 and 62: Salisbury District Hospital, Salisb
- Page 63 and 64: West Middlesex University Hospital,
- Page 65 and 66: “We have participated in MINAP fr
- Page 67 and 68: Dorset Cardiac and Stroke Network 7
- Page 69 and 70: “Participation in MINAP has helpe
- Page 71 and 72: Blackpool Victoria Hospital, Blackp
- Page 73 and 74: Harefield Hospital 139 84% 156 94%
- Page 75 and 76: Northern General Hospital, Sheffiel
- Page 77 and 78: Royal Victoria Infirmary, Newcastle
- Page 79 and 80: Warrington Hospital, Warrington 435
- Page 81 and 82: Withybush General Hospital, Haverfo
- Page 83 and 84: Part Three: Case Studies1. Call act
- Page 85 and 86: 3. Implementing a high-risk nSTEACS
- Page 87 and 88: The British Heart Foundation is a r
- Page 89 and 90: of six individual criteria - all in
- Page 91 and 92: 9. Use of MINAP data to develop and
- Page 93 and 94: Figure 26. Part 2 collected by Card
- Page 95: 12. Shifting the FocusNicola Mannin
- Page 99 and 100: Figure 30. Estimated excess risk of
- Page 101 and 102: Part 6: AppendicesAppendix 1: MINAP
- Page 103 and 104: Coronary thrombosisThe formation of
- Page 105 and 106: Birkhead J, Walker L. MINAP, a proj
- Page 107: Heart attacks recorded in MINAP in