Part One: Introduction1. Background to heart attacksThe term ‘heart attack’, while used widely in discussionsbetween clinicians and their patients, and therefore in thispublic report, is too imprecise to define the condition thatis the subject of this national clinical audit. The preferredterm is Acute Coronary Syndrome (ACS). This covers thesymptoms and clinical features that occur when there isan abrupt reduction in the blood supply to a segment ofheart muscle. Usually this is a consequence of a slowlyprogressive build-up of fibro-fatty material (atheroma)within the wall of the coronary artery, occurring over yearsand often without symptoms, followed by sudden disruptionof the internal artery wall. This readily causes blood to clotwithin the artery – a coronary thrombosis – and leads toa state of myocardial ischaemia, in which the demands ofthe affected heart muscle for oxygen-rich blood exceed thesupply of such blood down the clot-containing artery.If ischaemia is sufficiently prolonged or complete, death ofheart muscle results. This is myocardial infarction and isconfirmed if evidence of heart muscle cell death is found onblood testing. Such evidence may take some hours to appearand, to be most effective, treatment must start before theresults of such tests are available. <strong>Ischaemia</strong> is suggestedby characteristic symptoms (for example central chestdiscomfort, sweating, breathlessness) and abrupt changesin blood pressure, heart rate and heart rhythm (sometimesleading to collapse or sudden death). <strong>Ischaemia</strong> often can bedetected as electrical alterations on the electrocardiogram(ECG). When symptoms start it is uncertain whether theischaemia will be transient, and of no long-term consequence,or whether it will be prolonged and progress to infarction andconsequent failure of the heart to pump strongly. Rather thanwaiting to find out, all patients require urgent treatment toreverse ischaemia and prevent, or limit, infarction.Heart attack can occur at any age, but it is very rare toexperience one before middle age – consistently, most patientsin MINAP have been older than 65 years. This is because thedeposition of atheroma (see above) in the walls of coronaryarteries takes place over many years. Advanced investigationscan demonstrate coronary atheroma in many people in their30s and 40s who have no symptoms, yet who eventually suffera sudden coronary thrombosis many years later.A variety of genetic and potentially modifiable lifestyle factorsincrease the likelihood that a person will develop atheromaand later heart attack. The most easily recognised of theseinclude higher levels of blood lipids (e.g. cholesterol), blood1. http://www.bhf.org.uk/heart-health/prevention/risk-factors.aspx2. www.nice.org.uk/guidance/CG94glucose (i.e. diabetes) and blood pressure (hypertension), afamily history of premature coronary disease, a sedentarylifestyle with limited physical exercise, and cigarette smoking 1 .Many of these risk factors may be found in one individual,where they appear substantially to magnify the likelihood ofsuffering heart attack, or other vascular disorders. Someof them can be altered with a reduction in the chances ofheart attack and stroke – even in those who have alreadyexperienced such an event – forming part of the rationalefor both secondary preventive drug therapy and cardiacrehabilitation programmes.1.1 STEMI and nSTEMIBased upon the ECG, patients with characteristic symptomsare categorised into those with, and those without, ST segmentelevation – leading to the final diagnosis of those with STelevationmyocardial infarction (STEMI) and those with non-ST-elevation myocardial infarction (nSTEMI). A typical ECGshowing STEMI can be found accompanying the case studyfrom St George’s Hospital, London, later in this report (see partthree, case study 11). ST-elevation usually indicates completeblockage of a coronary artery and warrants specific immediatetreatment to re-open the artery – see ‘reperfusion therapy’below. The absence of ST-elevation usually indicates that anycoronary thrombosis is only partially occluding the artery.Although patients with STEMI are at greater early risk, themedium to long-term outcome (in terms of recurrent heartattack or death) is similar, if not worse, for those with nSTEMI– who are generally an older group. Each year MINAP reportsmore patients with nSTEMI than STEMI. Within the last threeyears the <strong>National</strong> Institute for Health and Clinical Excellence(NICE) 2 has published guidelines for the management ofpatients with nSTEMI, as well as the supporting evidence uponwhich the guidelines are based.1.2 Aims of managementThe aims of management of acute coronary syndromeare presented in Figure 1 together with examples of someinterventions that have been shown to be associated withbetter outcomes for patients, and have therefore beenincluded in various guidelines. Not all patients require allthe interventions and some interventions are unsuitable –contraindicated – in some patients. Therefore, cliniciansinvolved in providing care do not blindly follow protocols oftreatment but must use their clinical judgement to determinewhen particular treatments should be used, and when bestavoided, in individual patients.For patients with symptoms of ACS presenting without STelevationthere appears to be a clinically important spectrumof risk. This allows patients to be identified who would benefitmost from a more interventional approach – in particularan early coronary angiogram. Risk can be predicted by8 MINAP How the NHS cares for patients with heart attack
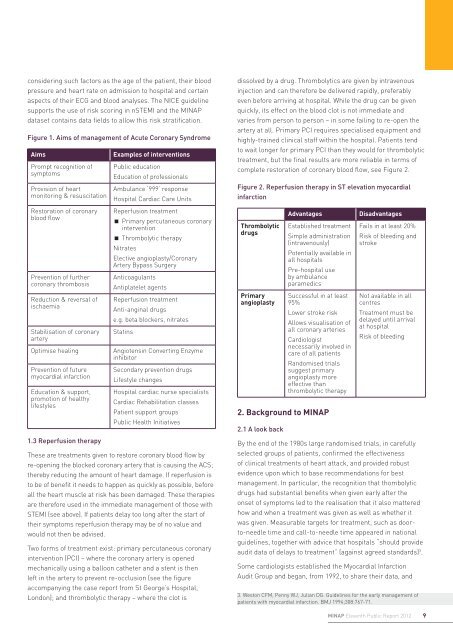
considering such factors as the age of the patient, their bloodpressure and heart rate on admission to hospital and certainaspects of their ECG and blood analyses. The NICE guidelinesupports the use of risk scoring in nSTEMI and the MINAPdataset contains data fields to allow this risk stratification.Figure 1. Aims of management of Acute Coronary SyndromeAimsPrompt recognition ofsymptomsProvision of heartmonitoring & resuscitationRestoration of coronaryblood flowPrevention of furthercoronary thrombosisReduction & reversal ofischaemiaStabilisation of coronaryarteryOptimise healingPrevention of futuremyocardial infarctionEducation & support,promotion of healthylifestyles1.3 Reperfusion therapyExamples of interventionsPublic educationEducation of professionalsAmbulance ‘999’ responseHospital Cardiac Care UnitsReperfusion treatmentPrimary percutaneous coronaryinterventionThrombolytic therapyNitratesElective angioplasty/CoronaryArtery Bypass SurgeryAnticoagulantsAntiplatelet agentsReperfusion treatmentAnti-anginal drugse.g. beta blockers, nitratesStatinsAngiotensin Converting EnzymeinhibitorSecondary prevention drugsLifestyle changesHospital cardiac nurse specialistsCardiac Rehabilitation classesPatient support groupsPublic Health InitiativesThese are treatments given to restore coronary blood flow byre-opening the blocked coronary artery that is causing the ACS;thereby reducing the amount of heart damage. If reperfusion isto be of benefit it needs to happen as quickly as possible, beforeall the heart muscle at risk has been damaged. These therapiesare therefore used in the immediate management of those withSTEMI (see above). If patients delay too long after the start oftheir symptoms reperfusion therapy may be of no value andwould not then be advised.Two forms of treatment exist: primary percutaneous coronaryintervention (PCI) – where the coronary artery is openedmechanically using a balloon catheter and a stent is thenleft in the artery to prevent re-occlusion (see the figureaccompanying the case report from St George’s Hospital,London); and thrombolytic therapy – where the clot isdissolved by a drug. Thrombolytics are given by intravenousinjection and can therefore be delivered rapidly, preferablyeven before arriving at hospital. While the drug can be givenquickly, its effect on the blood clot is not immediate andvaries from person to person – in some failing to re-open theartery at all. Primary PCI requires specialised equipment andhighly-trained clinical staff within the hospital. Patients tendto wait longer for primary PCI than they would for thrombolytictreatment, but the final results are more reliable in terms ofcomplete restoration of coronary blood flow, see Figure 2.Figure 2. Reperfusion therapy in ST elevation myocardialinfarctionThrombolyticdrugsPrimaryangioplastyAdvantagesEstablished treatmentSimple administration(intravenously)Potentially available inall hospitalsPre-hospital useby ambulanceparamedicsSuccessful in at least95%Lower stroke riskAllows visualisation ofall coronary arteriesCardiologistnecessarily involved incare of all patientsRandomised trialssuggest primaryangioplasty moreeffective thanthrombolytic therapy2. Background to MINAP2.1 A look backDisadvantagesFails in at least 20%Risk of bleeding andstrokeNot available in allcentresTreatment must bedelayed until arrivalat hospitalRisk of bleedingBy the end of the 1980s large randomised trials, in carefullyselected groups of patients, confirmed the effectivenessof clinical treatments of heart attack, and provided robustevidence upon which to base recommendations for bestmanagement. In particular, the recognition that thombolyticdrugs had substantial benefits when given early after theonset of symptoms led to the realisation that it also matteredhow and when a treatment was given as well as whether itwas given. Measurable targets for treatment, such as doorto-needletime and call-to-needle time appeared in nationalguidelines, together with advice that hospitals “should provideaudit data of delays to treatment” (against agreed standards) 3 .Some cardiologists established the <strong>Myocardial</strong> Infarction<strong>Audit</strong> Group and began, from 1992, to share their data, and3. Weston CFM, Penny WJ, Julian DG. Guidelines for the early management ofpatients with myocardial infarction. BMJ 1994;308:767-71.MINAP Eleventh Public Report 20129
- Page 1 and 2: Myocardial IschaemiaNational Audit
- Page 3 and 4: Myocardial Ischaemia National Audit
- Page 5 and 6: ForewordThe annual MINAP Report, no
- Page 7: Patients who received thrombolytic
- Page 11 and 12: egarding previous medical history.
- Page 13 and 14: 3. Improving quality,improving outc
- Page 15 and 16: is an acute heart failure syndrome
- Page 17 and 18: Alan KeysMINAP Steering Group patie
- Page 19 and 20: Figure 7. Patients admitted with a
- Page 21 and 22: Figure 11. Percentage of patients w
- Page 23 and 24: transfers require a significant amo
- Page 25 and 26: Table 8 shows the performance of th
- Page 27 and 28: This year we report on the interval
- Page 29 and 30: Conquest Hospital, St Leonards onSe
- Page 31 and 32: Royal Derby Hospital, Derby 62 89%
- Page 33 and 34: “During times of financial constr
- Page 35 and 36: Broomfield Hospital, Chelmsford 0 0
- Page 37 and 38: Leighton Hospital, Crewe 43 86% 49
- Page 39 and 40: Royal Preston Hospital, Preston 48
- Page 41 and 42: Wycombe Hospital, High Wycombe 11 1
- Page 43 and 44: “I know that MINAP data has been
- Page 45 and 46: Cheltenham General Hospital, Chelte
- Page 47 and 48: Manchester Royal Infirmary, Manches
- Page 49 and 50: Salford Royal Hospital, Manchester
- Page 51 and 52: “MINAP, and its long history, is
- Page 53 and 54: Table 6: Ambulance Services in Engl
- Page 55 and 56: Bradford Royal Infirmary, Bradford
- Page 57 and 58: Hexham General Hospital, Hexham 17
- Page 59 and 60:
Papworth Hospital, Cambridge 560 99
- Page 61 and 62:
Salisbury District Hospital, Salisb
- Page 63 and 64:
West Middlesex University Hospital,
- Page 65 and 66:
“We have participated in MINAP fr
- Page 67 and 68:
Dorset Cardiac and Stroke Network 7
- Page 69 and 70:
“Participation in MINAP has helpe
- Page 71 and 72:
Blackpool Victoria Hospital, Blackp
- Page 73 and 74:
Harefield Hospital 139 84% 156 94%
- Page 75 and 76:
Northern General Hospital, Sheffiel
- Page 77 and 78:
Royal Victoria Infirmary, Newcastle
- Page 79 and 80:
Warrington Hospital, Warrington 435
- Page 81 and 82:
Withybush General Hospital, Haverfo
- Page 83 and 84:
Part Three: Case Studies1. Call act
- Page 85 and 86:
3. Implementing a high-risk nSTEACS
- Page 87 and 88:
The British Heart Foundation is a r
- Page 89 and 90:
of six individual criteria - all in
- Page 91 and 92:
9. Use of MINAP data to develop and
- Page 93 and 94:
Figure 26. Part 2 collected by Card
- Page 95 and 96:
12. Shifting the FocusNicola Mannin
- Page 97 and 98:
Figure 29. Funnel plot of hospital
- Page 99 and 100:
Figure 30. Estimated excess risk of
- Page 101 and 102:
Part 6: AppendicesAppendix 1: MINAP
- Page 103 and 104:
Coronary thrombosisThe formation of
- Page 105 and 106:
Birkhead J, Walker L. MINAP, a proj
- Page 107:
Heart attacks recorded in MINAP in