EDI - European Association of Dental Implantologists
EDI - European Association of Dental Implantologists
EDI - European Association of Dental Implantologists

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
32<br />
<strong>EDI</strong><br />
<strong>EDI</strong> News<br />
Immediate loading<br />
vs. time-efficient treatment<br />
Competition increased as other manufacturers<br />
emerged. Much was made <strong>of</strong> the effectiveness <strong>of</strong> different<br />
surface types in the ensuing campaigns. These<br />
were designed to reach not only the dentists responsible<br />
for treatment decisions, but marketing efforts were<br />
also targeted directly at the patients. Today, the controversy<br />
has largely abated. Surfaces treated by sandblasting<br />
and high-temperature etching have become<br />
something <strong>of</strong> a standard. Their use can be considered<br />
the state <strong>of</strong> the art in the quest for osseointegration.<br />
Any newly developed surfaces will have to stand the<br />
test <strong>of</strong> time, which is not going to be easy given the<br />
very high success rates already on record.<br />
Competing manufacturers, but also implantologists,<br />
have instead embarked on a race for shorter<br />
healing periods and ways <strong>of</strong> <strong>of</strong>fering patients the<br />
benefits <strong>of</strong> immediate restoration. Extensive debates<br />
about these issues are a relatively new phenomenon,<br />
having started only five to seven years ago. Once<br />
again, however, they are based on the efforts and<br />
experience <strong>of</strong> dentists such as Dr Ledermann, who successfully<br />
used a bar design for the immediate restoration<br />
<strong>of</strong> implants 30 years ago. Some <strong>of</strong> the original<br />
techniques have fallen into oblivion, either because<br />
the system components available at the time would<br />
not allow the spectrum <strong>of</strong> indications to be increased<br />
or because the available implants did not have the<br />
properties required for immediate restoration.<br />
Furthermore, any expectations <strong>of</strong> immediately<br />
restoring all implants have turned out to be over -<br />
enthusiastic and are clearly being reconsidered today.<br />
Reduced healing periods <strong>of</strong> six to eight weeks <strong>of</strong>ten do<br />
not justify the extra effort that is required for immediate<br />
restoration. Even temporary restorations can <strong>of</strong>fer<br />
good patient comfort today. Current scientific evidence<br />
on the subject was summarized at the 1 st <strong>European</strong><br />
Consensus Conference <strong>of</strong> the BDIZ <strong>EDI</strong> in 2006.<br />
Challenges in the maxillary<br />
posterior segment<br />
Continuous progress has been made over the past<br />
25 years with regard to treatment options. The first<br />
implants were placed in the maxillary anterior segment<br />
(using the Tübingen implants for immediate<br />
placement) or to support a bar in the mandible<br />
(using titanium implants). These original indications<br />
were followed by maxillary restorations supported by<br />
implants, whose insertion was guided by the principle<br />
<strong>of</strong> utilizing existing bone. Prosthetic handling<br />
became extremely difficult when implants were<br />
inserted in the tuberosity region. Some fellow den-<br />
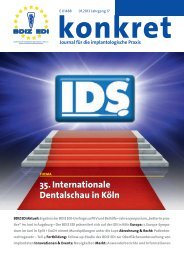
TPS-coated IMZ implant afflicted with peri-implantitis. A large bone defect is present<br />
on the lingual aspect.<br />
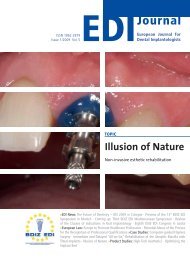
Polarized-light micrograph <strong>of</strong> an<br />
osseointegrated implant. Note the<br />
structure <strong>of</strong> collagen fibers.<br />
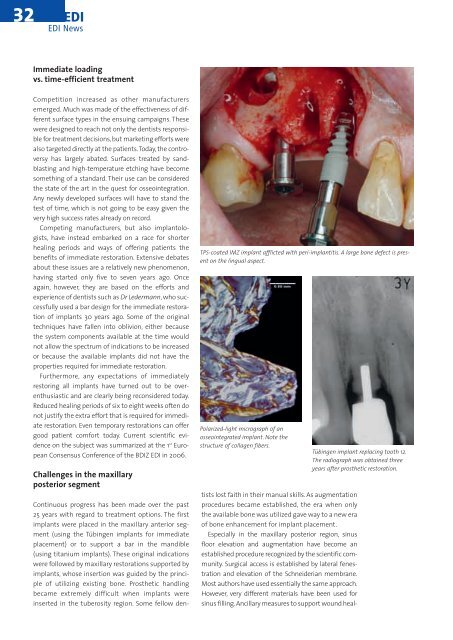
Tübingen implant replacing tooth 12.<br />
The radiograph was obtained three<br />
years after prosthetic restoration.<br />
tists lost faith in their manual skills. As augmentation<br />
procedures became established, the era when only<br />
the available bone was utilized gave way to a new era<br />
<strong>of</strong> bone enhancement for implant placement.<br />
Especially in the maxillary posterior region, sinus<br />
floor elevation and augmentation have become an<br />
established procedure recognized by the scientific community.<br />
Surgical access is established by lateral fenestration<br />
and elevation <strong>of</strong> the Schneiderian membrane.<br />
Most authors have used essentially the same approach.<br />
However, very different materials have been used for<br />
sinus filling. Ancillary measures to support wound heal-