

Current Allergy and Clinical Immunology - March 2008
Current Allergy and Clinical Immunology - March 2008
Current Allergy and Clinical Immunology - March 2008

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
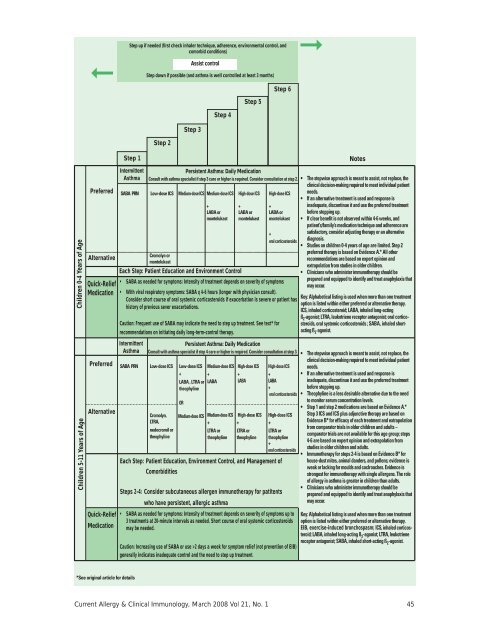
➞Step up if needed (first check inhaler technique, adherence, environmental control, <strong>and</strong>comorbid conditions)Assist controlStep down if possible (<strong>and</strong> asthma is well controlled at least 3 months)Step 6➞Step 5Step 4Step 3Step 2Step 1NotesChildren 0-4 Years of AgePreferredAlternativeQuick-ReliefMedicationIntermittentAsthmaPersistent Asthma: Daily MedicationConsult with asthma specialist if step 3 care or higher is required. Consider consultation at step 2.SABA PRN Low-dose ICS Medium-dose ICS Medium-dose ICS+LABA ormontelukastCromolyn ormontelukastEach Step: Patient Education <strong>and</strong> Environment ControlHigh-dose ICS+LABA ormontelukastHigh-dose ICS+LABA ormontelukast• SABA as needed for symptoms: Intensity of treatment depends on severity of symptems• With viral respiratory symptoms: SABA q 4-6 hours (longer with physician consult).Consider short course of oral systemic corticosteroids if exacerbation is severe or patient hashistory of previous sever exacerbations.Caution: Frequent use of SABA may indicate the need to step up treatment. See text* forrecommendations on initiating daily long-term-control therapy.+oral corticosteroids• The stepwise approach is meant to assist, not replace, theclinical decision-making required to meet individual patientneeds.• If an alternative treatment is used <strong>and</strong> response isinadequate, discontinue it <strong>and</strong> use the preferred treatmentbefore stepping up.• If clear benefit is not observed within 4-6 weeks, <strong>and</strong>patient’s/family’s medication technique <strong>and</strong> adherence aresatisfactory, consider adjusting therapy or an alternativediagnosis.• Studies on children 0-4 years of age are limited. Step 2preferred therapy is based on Evidence A.* All otherrecommendations are based on expert opinion <strong>and</strong>extrapolation from studies in older children.• Clinicians who administer immunotherapy should beprepared <strong>and</strong> equipped to identify <strong>and</strong> treat anaphylaxis thatmay occur.Key: Alphabetical listing is used when more than one treatmentoption is listed within either preferred or alternative therapy.ICS, inhaled corticosteroid; LABA, inhaled long-actingß 2 -agonist; LTRA, leukotriene receptor antagonist; oral corticosteroids,oral systemic corticosteroids ; SABA, inhaled shortactingß 2 -agonist.Children 5-11 Years of AgePreferredAlternativeQuick-ReliefMedicationIntermittentAsthmaPersistent Asthma: Daily MedicationConsult with asthma specialist if step 4 care or higher is required. Consider consultation at step 3.SABA PRN Low-dose ICS Low-dose ICS+Cromolyn,LTRA,nedocromil ortheophylineLABA , LTRA ortheophylineORMedium-dose ICSMedium-dose ICS High-dose ICS++LABALABAMedium-dose ICS+LTRA ortheophylineHigh-dose ICS+LTRA ortheophylineHigh-dose ICS+LABA+oral corticosteroidsHigh-dose ICS+LTRA ortheophyline+oral corticosteroidsEach Step: Patient Education, Environment Control, <strong>and</strong> Management ofComorbiditiesSteps 2-4: Consider subcutaneous allergen immunotherapy for patitentswho have persistent, allergic asthma• SABA as needed for symptoms: Intensity of treatment depends on severity of symptoms up to3 treatments at 20-minute intervals as needed. Short course of oral systemic corticosteroidsmay be needed.Caution: Increasing use of SABA or use >2 days a week for symptom relief (not prevention of EIB)generally indicates inadequate control <strong>and</strong> the need to step up treatment.• The stepwise approach is meant to assist, not replace, theclinical decision-making required to meet individual patientneeds.• If an alternative treatment is used <strong>and</strong> response isinadequate, discontinue it <strong>and</strong> use the preferred treatmentbefore stepping up.• Theophyline is a less desirable alternative due to the needto monitor serum concentration levels.• Step 1 <strong>and</strong> step 2 medications are based on Evidence A.*Step 3 ICS <strong>and</strong> ICS plus adjunctive therapy are based onEvidence B* for efficacy of each treatment <strong>and</strong> extrapolationfrom comparator trials in older children <strong>and</strong> adults –comparator trials are not available for this age group; steps4-6 are based on expert opinion <strong>and</strong> extrapolation fromstudies in older children <strong>and</strong> adults.• Immunotherapy for steps 2-4 is based on Evidence B* forhouse-dust mites, animal d<strong>and</strong>ers, <strong>and</strong> pollens; evidence isweak or lacking for moulds <strong>and</strong> coclroaches. Evidence isstrongest for immunotherapy with single allergens. The roleof allergy in asthma is greater in children than adults.• Clinicians who administer immunotherapy should beprepared <strong>and</strong> equipped to identify <strong>and</strong> treat anaphylaxis thatmay occur.Key: Alphabetical listing is used when more than one treatmentoption is listed within either preferred or alternative therapy.EIB, exercise-induced bronchospasm; ICS, inhaled corticosteroid;LABA, inhaled long-acting ß 2 -agonist; LTRA, leukotrienereceptor antagonist; SABA, inhaled short-acting ß 2 -agonist.*See original article for details<strong>Current</strong> <strong>Allergy</strong> & <strong>Clinical</strong> <strong>Immunology</strong>, <strong>March</strong> <strong>2008</strong> Vol 21, No. 1 45













