for uninsured services - Saskatchewan Medical Association
for uninsured services - Saskatchewan Medical Association
for uninsured services - Saskatchewan Medical Association

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
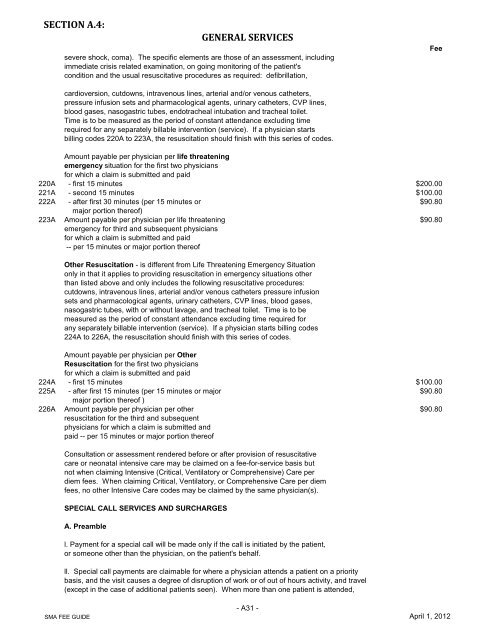
SECTION A.4:GENERAL SERVICESsevere shock, coma). The specific elements are those of an assessment, includingimmediate crisis related examination, on going monitoring of the patient'scondition and the usual resuscitative procedures as required: defibrillation,Feecardioversion, cutdowns, intravenous lines, arterial and/or venous catheters,pressure infusion sets and pharmacological agents, urinary catheters, CVP lines,blood gases, nasogastric tubes, endotracheal intubation and tracheal toilet.Time is to be measured as the period of constant attendance excluding timerequired <strong>for</strong> any separately billable intervention (service). If a physician startsbilling codes 220A to 223A, the resuscitation should finish with this series of codes.Amount payable per physician per life threateningemergency situation <strong>for</strong> the first two physicians<strong>for</strong> which a claim is submitted and paid220A - first 15 minutes $200.00221A - second 15 minutes $100.00222A - after first 30 minutes (per 15 minutes or $90.80major portion thereof)223A Amount payable per physician per life threatening $90.80emergency <strong>for</strong> third and subsequent physicians<strong>for</strong> which a claim is submitted and paid-- per 15 minutes or major portion thereofOther Resuscitation - is different from Life Threatening Emergency Situationonly in that it applies to providing resuscitation in emergency situations otherthan listed above and only includes the following resuscitative procedures:cutdowns, intravenous lines, arterial and/or venous catheters pressure infusionsets and pharmacological agents, urinary catheters, CVP lines, blood gases,nasogastric tubes, with or without lavage, and tracheal toilet. Time is to bemeasured as the period of constant attendance excluding time required <strong>for</strong>any separately billable intervention (service). If a physician starts billing codes224A to 226A, the resuscitation should finish with this series of codes.Amount payable per physician per OtherResuscitation <strong>for</strong> the first two physicians<strong>for</strong> which a claim is submitted and paid224A - first 15 minutes $100.00225A - after first 15 minutes (per 15 minutes or major $90.80major portion thereof )226A Amount payable per physician per other $90.80resuscitation <strong>for</strong> the third and subsequentphysicians <strong>for</strong> which a claim is submitted andpaid -- per 15 minutes or major portion thereofConsultation or assessment rendered be<strong>for</strong>e or after provision of resuscitativecare or neonatal intensive care may be claimed on a fee-<strong>for</strong>-service basis butnot when claiming Intensive (Critical, Ventilatory or Comprehensive) Care perdiem fees. When claiming Critical, Ventilatory, or Comprehensive Care per diemfees, no other Intensive Care codes may be claimed by the same physician(s).SPECIAL CALL SERVICES AND SURCHARGESA. Preamblel. Payment <strong>for</strong> a special call will be made only if the call is initiated by the patient,or someone other than the physician, on the patient's behalf.ll. Special call payments are claimable <strong>for</strong> where a physician attends a patient on a prioritybasis, and the visit causes a degree of disruption of work or of out of hours activity, and travel(except in the case of additional patients seen). When more than one patient is attended,SMA FEE GUIDE- A31 -April 1, 2012