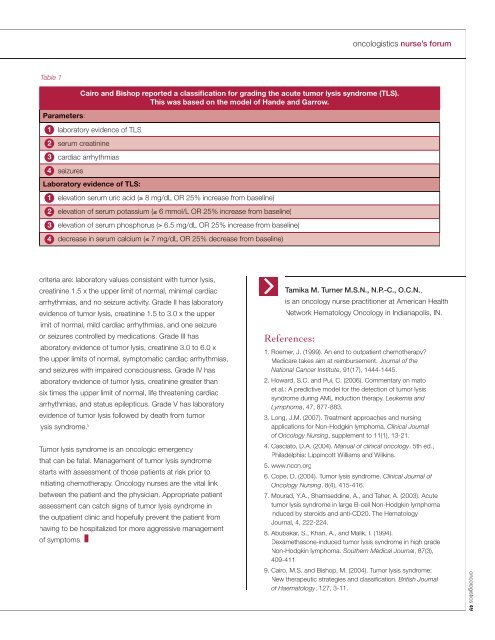
nurse’s forumoncologistics volume 7, issue 1 - spr<strong>in</strong>g <strong>2008</strong> 48excessive sweat<strong>in</strong>g or night sweats, anorexia, fever,or unexpla<strong>in</strong>ed fatigue. 2 Enlarged lymph nodes can befound upon physical exam<strong>in</strong>ation or on radiology fi lms,such as chest x-rays or CT scans. Diagnosis is made byobta<strong>in</strong><strong>in</strong>g a tissue biopsy of an <strong>in</strong>volved organ or lymphnode. A complete blood count, lactic dehydrogenase level,electrolytes, liver function tests, and renal function tests arealso done as part of the rout<strong>in</strong>e workup for Diffuse largeB-cell lymphoma. Further workup may <strong>in</strong>clude a positronemission tomography test to evaluate if metastatic diseaseis present. 3Diffuse large B-cell lymphoma is staged by utiliz<strong>in</strong>gCotswold’s classifi cation system. Stage one disease<strong>in</strong>volves a s<strong>in</strong>gle lymph node or structure; stage twodisease <strong>in</strong>volves two or more lymph nodes on the sameside of the diaphragm; stage three disease <strong>in</strong>volves two ormore lymph nodes on both sides of the diaphragm; andstage four disease <strong>in</strong>volves one or more extranodal sites. 4Treatment options are based on stag<strong>in</strong>g of the disease,and for all <strong>in</strong>tensive purposes, the goal of <strong>in</strong>ductionchemotherapy for Diffuse large B-cell lymphoma iscurative. Treatment for localized (stage I or II) diseaseis based on the size or bulk<strong>in</strong>ess of the tumor. Tumorsthat are “non-bulky” and less than 10 cm can be treatedwith three cycles of Rituxan ® (rituximab), Cytoxan ®(cyclophosphamide), Oncov<strong>in</strong> ® (v<strong>in</strong>crist<strong>in</strong>e), Adriamyc<strong>in</strong> ®(doxorubic<strong>in</strong>), prednisone, and radiation therapy. Tumorsthat are greater than or equal to 10 cm or “bulky”should be treated with six to eight cycles of rituximab,cyclophosphamide, v<strong>in</strong>crist<strong>in</strong>e, doxorubic<strong>in</strong>, prednisone,and radiation therapy. Tumors that are “advanced” (stage IIIor IV) should be treated the same as bulky tumors. Cl<strong>in</strong>icaltrials are also an option for those with advanced disease aswell as autologous stem cell transplants. 5Adverse effects from the chemotherapy agents usedto treat Diffuse large B-cell lymphoma <strong>in</strong>clude: nausea,vomit<strong>in</strong>g, diarrhea, constipation, oral mucositis, anorexia,cytopenias, oral candidiasis, cystitis, pa<strong>in</strong>, peripheralneuropathy, alopecia, depression, and tumor lysis syndrome.Of the adverse effects, tumor lysis syndrome is knownas one of the “oncologic emergencies” as it can be lifethreaten<strong>in</strong>g. It is a complication that follows chemotherapyfor lympho-proliferative disorders. There is a spontaneousor chemotherapy-<strong>in</strong>duced mass destruction of tumorcells. Cell lysis releases <strong>in</strong>tracellular contents <strong>in</strong>to thebloodstream and can cause fatal arrhythmias if notcorrected. Nucleic acids are also released <strong>in</strong>to thebloodstream and further broken down <strong>in</strong>to uric acid.Renal <strong>in</strong>suffi ciency can result <strong>in</strong> the <strong>in</strong>ability of the kidneysto excrete uric acid, which can lead to acute renal failure. 6Tumor lysis syndrome is characterized by hyperuricemia,hyperkalemia, hypocalcemia, hyperphosphatemia, lacticacidosis, and renal failure. 7What role do oncology nurses, who work <strong>in</strong> outpatient<strong>in</strong>fusion cl<strong>in</strong>ics, play <strong>in</strong> patients receiv<strong>in</strong>g chemotherapyfor Diffuse large B-cell lymphoma? Oncology nurses haveto fi rst be aware of those patients at risk for tumor lysis.Tumor lysis syndrome commonly occurs <strong>in</strong> tumors that arehighly responsive to chemotherapy such as lymphomas.The risk for tumor lysis is also greater <strong>in</strong> those patientswith extreme leukocytosis, bulky tumors, elevated LDH,pre-exist<strong>in</strong>g renal <strong>in</strong>suffi ciency, and hyperuricemia priorto <strong>in</strong>itiation of chemotherapy. 8 The oncology nurseshould be assess<strong>in</strong>g all patients with risk factors prior tothem receiv<strong>in</strong>g chemotherapy. The patient’s laboratorydata should be reviewed and renal function should beassessed. Any abnormal laboratory results, as well asabnormal fi nd<strong>in</strong>gs on a physical exam, should be reportedimmediately to the physician or mid-level provider (NP orCNS). Management of tumor lysis syndrome <strong>in</strong>volves goodhydration with diuresis, alkal<strong>in</strong>ization of ur<strong>in</strong>e with sodiumbicarbonate, use of Allopur<strong>in</strong>ol or Rasburicase for reductionof uric acid, dietary restriction of phosphorus or phosphateb<strong>in</strong>ders, and Kaexylate for hyperkalemia. Allopur<strong>in</strong>olshould be given at a dose of 300 mg by mouth twicedaily and should beg<strong>in</strong> at least two days prior to start<strong>in</strong>gchemotherapy. Rasburicase is given <strong>in</strong>travenously, its effectpeaks with<strong>in</strong> hours of <strong>in</strong>fus<strong>in</strong>g and it removes exist<strong>in</strong>g uricacid from the body. It is given at 0.05mg/kg up to 0.2mg/kg. The disadvantage of Rasburicase is that it should begiven for three to fi ve days <strong>in</strong> order to control tumor lysis.Table 1 by Cairo and Bishop shows laboratory valuesconsistent with tumor lysis syndrome. They also gradedtumor lysis syndrome on a scale of one to fi ve. Grade I
oncologistics nurse’s forumTable 1Parameters:1234Cairo and Bishop reported a classification for grad<strong>in</strong>g the acute tumor lysis syndrome (TLS).This was based on the model of Hande and Garrow.laboratory evidence of TLSserum creat<strong>in</strong><strong>in</strong>ecardiac arrhythmiasseizuresLaboratory evidence of TLS:1234elevation serum uric acid (≥ 8 mg/dL OR 25% <strong>in</strong>crease from basel<strong>in</strong>e)elevation of serum potassium (≥ 6 mmol/L OR 25% <strong>in</strong>crease from basel<strong>in</strong>e)elevation of serum phosphorus (≥ 6.5 mg/dL OR 25% <strong>in</strong>crease from basel<strong>in</strong>e)decrease <strong>in</strong> serum calcium (≤ 7 mg/dL OR 25% decrease from basel<strong>in</strong>e)criteria are: laboratory values consistent with tumor lysis,creat<strong>in</strong><strong>in</strong>e 1.5 x the upper limit of normal, m<strong>in</strong>imal cardiacarrhythmias, and no seizure activity. Grade II has laboratoryevidence of tumor lysis, creat<strong>in</strong><strong>in</strong>e 1.5 to 3.0 x the upperlimit of normal, mild cardiac arrhythmias, and one seizureor seizures controlled by medications. Grade III haslaboratory evidence of tumor lysis, creat<strong>in</strong><strong>in</strong>e 3.0 to 6.0 xthe upper limits of normal, symptomatic cardiac arrhythmias,and seizures with impaired consciousness. Grade IV haslaboratory evidence of tumor lysis, creat<strong>in</strong><strong>in</strong>e greater thansix times the upper limit of normal, life threaten<strong>in</strong>g cardiacarrhythmias, and status epilepticus. Grade V has laboratoryevidence of tumor lysis followed by death from tumorlysis syndrome. 9Tumor lysis syndrome is an oncologic emergencythat can be fatal. Management of tumor lysis syndromestarts with assessment of those patients at risk prior to<strong>in</strong>itiat<strong>in</strong>g chemotherapy. Oncology nurses are the vital l<strong>in</strong>kbetween the patient and the physician. Appropriate patientassessment can catch signs of tumor lysis syndrome <strong>in</strong>the outpatient cl<strong>in</strong>ic and hopefully prevent the patient fromhav<strong>in</strong>g to be hospitalized for more aggressive managementof symptoms. ❚Tamika M. Turner M.S.N., N.P.-C., O.C.N.,is an oncology nurse practitioner at American HealthNetwork <strong>Hematology</strong> Oncology <strong>in</strong> Indianapolis, IN.References:1. Roemer, J. (1999). An end to outpatient chemotherapy?Medicare takes aim at reimbursement. Journal of theNational Cancer Institute, 91(17), 1444-1445.2. Howard, S.C. and Pui, C. (2006). Commentary on matoet al.: A predictive model for the detection of tumor lysissyndrome dur<strong>in</strong>g AML <strong>in</strong>duction therapy. Leukemia andLymphoma, 47, 877-883.3. Long, J.M. (2007). Treatment approaches and nurs<strong>in</strong>gapplications for Non-Hodgk<strong>in</strong> lymphoma. Cl<strong>in</strong>ical Journalof Oncology Nurs<strong>in</strong>g, supplement to 11(1), 13-21.4. Casciato, D.A. (2004). Manual of cl<strong>in</strong>ical oncology. 5th ed.,Philadelphia: Lipp<strong>in</strong>cott Williams and Wilk<strong>in</strong>s.5. www.nccn.org6. Cope, D. (2004). Tumor lysis syndrome. Cl<strong>in</strong>ical Journal ofOncology Nurs<strong>in</strong>g, 8(4), 415-416.7. Mourad, Y.A., Shamsedd<strong>in</strong>e, A., and Taher, A. (2003). Acutetumor lysis syndrome <strong>in</strong> large B-cell Non-Hodgk<strong>in</strong> lymphoma<strong>in</strong>duced by steroids and anti-CD20. The <strong>Hematology</strong>Journal, 4, 222-224.8. Abubakar, S., Khan, A., and Malik, I. (1994).Dexamethasone-<strong>in</strong>duced tumor lysis syndrome <strong>in</strong> high gradeNon-Hodgk<strong>in</strong> lymphoma. Southern Medical Journal, 87(3),409-411.9. Cairo, M.S. and Bishop, M. (2004). Tumor lysis syndrome:New therapeutic strategies and classifi cation. British Journalof Haematology, 127, 3-11.oncologistics 49