INTERNATIONAL TRENDS IN IMMUNITY VOL.1 NO.2 APRIL 2013ISSN 2326-3121 (Pr<strong>in</strong>t) ISSN 2326-313X (Onl<strong>in</strong>e) http://www.researchpub.org/journal/iti/iti.htmlcohort #1). Reactive LN were non tumoral but <strong>in</strong>flammatory oradjacent to a lymphomatous LN for one DLBCL patient (n=7,cohort#1). Tumoral LN were HL, LL, FL or DLBCL (n=27,cohort#1; n=22, cohort#2; n=46, cohort#3).TABLE ISUMMARY OF PATIENT CHARACTERISTICS AT DIAGNOSIS FOR COHORTS #1(PARIS-HEGP HOSPITAL), #2 (PARIS-HÔTEL DIEU HOSPITAL), AND #3(RENNES-PONTCHAILLOU HOSPITAL).Cohort#1#2#3Lymph nodeB. <strong>Cell</strong> isolationFresh unfixed LN were m<strong>in</strong>ced with a sterile blade <strong>in</strong> RPMImedium and were either digested with 2mg/mL Collagenase(Worth<strong>in</strong>gton, Roche, Meylan, France) and 0.1mg/mL Dnase I(Roche, Meylan, France) at 37°C for 50m<strong>in</strong>, filtered and r<strong>in</strong>sed<strong>in</strong> PBS with 2mM EDTA and 2% FCS (cohort#1), or weresubjected to a mechanical dissociation <strong>in</strong> petri dishes us<strong>in</strong>g25-gauge needles (cohort#2), or with the Medimach<strong>in</strong>e (BectonDick<strong>in</strong>son, San Jose, CA) (cohort#3).C. Flow cytometry<strong>Cell</strong>s were pre<strong>in</strong>cubated with PBS + 2% human AB serum toblock non-specific b<strong>in</strong>d<strong>in</strong>g to Fc receptors, then 5.10 5 cells perwell were sta<strong>in</strong>ed with ECD anti-CD3 (UCHT1), PE-cyan<strong>in</strong>5anti-<strong>CD4</strong> (13B8.2), PE-cyan<strong>in</strong>7 anti-<strong>CD8</strong> (SFCI21Thy2D3)from Beckman Coulter, or with PE-cyan<strong>in</strong>5 conjugatedanti-CD3 (UCHT1, Dako, Trappes, France) and/or with thefollow<strong>in</strong>g BD-Biosciences (Le Pont-de-Claix, France) mAb:Alexa fluor 700 anti-CD3 (UCHT1), PE anti-<strong>CD4</strong> (SK3),pacific blue anti-<strong>CD4</strong> (SK3), FITC anti-<strong>CD8</strong> (SK1),APC-cyan<strong>in</strong>7 anti-<strong>CD8</strong> (SK1) or the correspond<strong>in</strong>g isotypicmAb controls. Data were acquired us<strong>in</strong>g a n<strong>in</strong>e-colours LSRII(BD-Biosciences) or a four-colors FACS calibur(BD-Biosciences) or a five-colors FC500 (Beckman Coulter),and analyzed with the Diva (BD-Biosciences), <strong>Cell</strong>quest(BD-Biosciences), or CXP softwares (Beckman Coulter) forcohorts #1, #2 and #3, respectively.D. ImmunohistochemistryNumber(% of total)AgeM<strong>in</strong>-max (median)SexM/FNormal 11 (9.7%) 55-81 (72) 9/2Reactive 7 (6.2%) 25-70 (32) 3/4HL :non mediast<strong>in</strong>al localizations7 (6.2%) 21-80 (35) 3/4LL 4 (3.5%) 64-86 (75) 4/0FL 9 (8%) 27-83 (56) 5/4DLBCL : mediast<strong>in</strong>al 2 (1.8%) 25-55 (40) 2/0Other localizations 5 (4.4%) 53-86 (73) 3/2DLBCL : mediast<strong>in</strong>al 10 (9.9%) 18-68 (33) 5/5Other localizations 4 (3.5%) 40-79 (66.5) 4/0HL: mediast<strong>in</strong>al 7 (6.2%) 25-50 (32) 4/3Other localizations 1 (0.9%) 42 (42) 1/0DLBCL : mediast<strong>in</strong>al 4 (3.5%) 20-25 (23.5) 1/3Other localizations 26 (23%) 37-96 (77.5) 15/11HL: mediast<strong>in</strong>al 1 (0.9%) 36 (36) 1/0Other localizations 15 (13.3%) 15-80 (32) 6/9HL, hodgk<strong>in</strong> lymphoma ; LL, lymphocytic lymphoma ; FL, follicularlymphoma ; DLBCL, diffuse large B-cell lymphoma ; M, male ; F, female.Immunohistochemistry sta<strong>in</strong><strong>in</strong>g was performed on paraff<strong>in</strong>embedded sections with the follow<strong>in</strong>g mAb specific to CD3,(clone SP7, Microm Neomarker, Francheville, France), <strong>CD8</strong>(114B, Dako), TiA1 (TiA1, Beckman Coulter, Villep<strong>in</strong>te,France), Granzyme B (GranzB, Tebu, Le Perray-en-Yvel<strong>in</strong>es,France) for the T-cell subtypes. Briefly, immunosta<strong>in</strong><strong>in</strong>g onparaff<strong>in</strong> section was performed after antigen retrieval,avid<strong>in</strong>/biot<strong>in</strong> and Fc receptors block<strong>in</strong>g treatment. Sta<strong>in</strong><strong>in</strong>g wasrevealed with streptavid<strong>in</strong>-peroxidase and DAB.E. Statistical analysisMann-Whitney tests were performed us<strong>in</strong>g StatView (SASInstitute, Cary, NC). P values less than 0.05 were consideredstatistically significant.III. RESULTS AND DISCUSSIONLN from 7 HL and 21 B-NHL subtypes were analyzed byflow cytometry for the presence and the relative distribution of<strong>CD4</strong> + and <strong>CD8</strong> + T-cell subsets. These lymphomas werecompared to 11 normal and 7 reactive LN (Table 1, cohort #1).Non tumoral LN as well as HL, LL and FL samples showed amedian <strong>CD4</strong>:<strong>CD8</strong> ratio > 2 (Fig. 1). Surpris<strong>in</strong>gly, an <strong>in</strong>vertedmedian <strong>CD4</strong>:<strong>CD8</strong> T-cell ratio was specifically observed <strong>in</strong>DLBCL (0.76±0.33; DLBCL vs normal LN: P
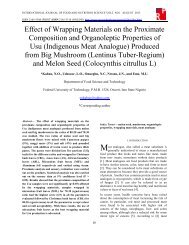
INTERNATIONAL TRENDS IN IMMUNITY VOL.1 NO.2 APRIL 2013ISSN 2326-3121 (Pr<strong>in</strong>t) ISSN 2326-313X (Onl<strong>in</strong>e) http://www.researchpub.org/journal/iti/iti.htmlshown <strong>in</strong> Fig. 1 (open and light-blue diamonds, cohorts #2 and#3 respectively) confirmed the low median <strong>CD4</strong>:<strong>CD8</strong> ratio(0.79±0.57 and 1.22±1.27, respectively) without statisticaldifference between the three cohorts (P=0.37). Moreover, <strong>in</strong>two DLBCL cases, tumoral LN from cohorts #1 and #2 weretreated simultaneously but <strong>in</strong>dependently with differenttechniques and the respective <strong>CD4</strong>:<strong>CD8</strong> T-cell ratios werequite similar (data not shown). Interest<strong>in</strong>gly, a tumoral LN andan adjacent non tumoral LN (confirmed by pathologicalexam<strong>in</strong>ation) from one patient were analyzed simultaneouslyand different <strong>CD4</strong>:<strong>CD8</strong> ratios were found (Fig. 1, arrows). Inthis case, the <strong>CD4</strong>:<strong>CD8</strong> ratio from the LN without presence oftumor cells was <strong>in</strong> the range of the set of reactive LN whereasthe tumoral LN displayed the lowest <strong>CD4</strong>:<strong>CD8</strong> ratio (0.11).Therefore, the low <strong>CD4</strong>:<strong>CD8</strong> T-cell ratio for DLBCL samplesseems to be restricted to the tumoral LN and may be <strong>in</strong>duced bythe tumour cells. Moreover, the <strong>CD4</strong>:<strong>CD8</strong> ratio is not l<strong>in</strong>ked tothe T-cell number variation (data not shown).In an extensive study on T cell lymphoma, Gorczyca et coll.noticed a low <strong>CD4</strong>:<strong>CD8</strong> ratio <strong>in</strong> 10 DLBCL cases [5]. Anotherstudy showed that DLBCL patients display<strong>in</strong>g the lowest<strong>CD4</strong>:<strong>CD8</strong> ratios showed a worse overall survival,<strong>in</strong>dependently from the cl<strong>in</strong>ical stage at diagnosis [9]. However,no extensive comparison between normal and tumorallymphoid tissues, nor between LN from HL and non-Hodgk<strong>in</strong>lymphoma subtypes was performed <strong>in</strong> these studies. In thepresent work we analyzed 67 LN from three <strong>in</strong>dependentcohorts classified <strong>in</strong> 6 entities and we demonstrate that DLBCLLN exhibit an <strong>in</strong>verted <strong>CD4</strong>:<strong>CD8</strong> ratio before any treatment.To <strong>in</strong>vestigate the <strong>in</strong>fluence of the mediast<strong>in</strong>al (ie. thymic)localisation on the <strong>CD4</strong>:<strong>CD8</strong> ratio, we compared DLBCL andHL which are the most common lymphomas of themediast<strong>in</strong>um. Identification of these tumors (DLBCL; HL,respectively) was assessed by immunohistochemistry for theexpression of the follow<strong>in</strong>g markers: CD20 + (12/12; 0/7),CD79a + (12/12; 0/7), CD23 + (10/12; 1/7), CD30 + (10/12; 7/7),CD15 + (0/12; 5/7), and LMP-1 + (0/12; 1/7). The median<strong>CD4</strong>:<strong>CD8</strong> ratios are below 1 <strong>in</strong> primary mediast<strong>in</strong>al (0.69±1.15)and non mediast<strong>in</strong>al (0.91±1.03) tumoral LN from DLBCLpatients, and are not significantly different (Fig. 2; P=0.10).Contrast<strong>in</strong>g with DLBCL, the median <strong>CD4</strong>:<strong>CD8</strong> ratio for HLwas over 3, <strong>in</strong>dependently from the mediast<strong>in</strong>al and nonmediast<strong>in</strong>al localisations (3.93±4.29 and 5.61±10.98,respectively; P=0.73). Altogether these results suggest that the<strong>CD4</strong>:<strong>CD8</strong> ratio seems to depend more on the lymphomasubtype than on tumoral LN localization. The <strong>CD4</strong>:<strong>CD8</strong> ratioevaluation <strong>in</strong> LN could be an <strong>in</strong>terest<strong>in</strong>g additional tool for thedifferential diagnosis between some primary mediast<strong>in</strong>alDLBCL and mediast<strong>in</strong>al HL.The <strong>in</strong>verted median ratio <strong>in</strong> DLBCL could be expla<strong>in</strong>ed byan <strong>in</strong>creased number of <strong>CD8</strong> + T-cells, a decreased number of<strong>CD4</strong> + T-cells, or both. Us<strong>in</strong>g immunohistochemistry, we founda high proportion of <strong>CD8</strong> + cells compared to the CD3 sta<strong>in</strong><strong>in</strong>gof T-cells <strong>in</strong> DLBCL (Fig. 3). In contiguous slides, these cellsexpressed cytotoxic prote<strong>in</strong>s like TiA1 and Granzyme B.Moreover, the DLBCL T-cell proportion did not differ from HLand FL, nor reactive and normal LN (data not shown).DLBCLHLCD3<strong>CD8</strong>100nonmediast<strong>in</strong>almediast<strong>in</strong>alnonmediast<strong>in</strong>almediast<strong>in</strong>aliiitioral10e-cT8D:C4 1DCiiiTiA1ivGz-B0.1***********Fig. 2. Analysis of the <strong>CD4</strong>:<strong>CD8</strong> T-cell ratio for different subgroups ofDLBCL patients. <strong>CD4</strong>:<strong>CD8</strong> T-cell ratios are represented on a logarithmicord<strong>in</strong>ate <strong>in</strong> order to respect the proportionality of distribution between valuesover or below 1. The horizontal red bar corresponds to the median value.Statistical analysis was performed us<strong>in</strong>g the Mann-Whitney test.Significativity values are <strong>in</strong>dicated as follow: *: P < 0.05 ; **: P < 0.01 ; ***:P < 0.001.47Fig. 3. Immunosta<strong>in</strong><strong>in</strong>g of (i) CD3, (ii) <strong>CD8</strong>, (iii) TiA-1 and (iv) GranzymeB on a lymph node from a representative mediast<strong>in</strong>al DLBCL patient.Magnification: 200. Bars: 20µm.