NCEPOD: Trauma - Who Cares? - London Health Programmes
NCEPOD: Trauma - Who Cares? - London Health Programmes
NCEPOD: Trauma - Who Cares? - London Health Programmes

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
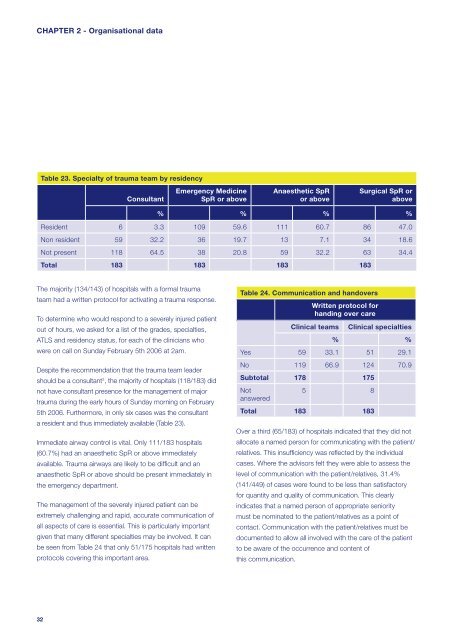
CHAPTER 2 - Organisational dataTable 23. Specialty of trauma team by residencyConsultantEmergency MedicineSpR or aboveAnaesthetic SpRor aboveSurgical SpR orabove% % % %Resident 6 3.3 109 59.6 111 60.7 86 47.0Non resident 59 32.2 36 19.7 13 7.1 34 18.6Not present 118 64.5 38 20.8 59 32.2 63 34.4Total 183 183 183 183The majority (134/143) of hospitals with a formal traumateam had a written protocol for activating a trauma response.To determine who would respond to a severely injured patientout of hours, we asked for a list of the grades, specialties,ATLS and residency status, for each of the clinicians whowere on call on Sunday February 5th 2006 at 2am.Despite the recommendation that the trauma team leadershould be a consultant 3 , the majority of hospitals (118/183) didnot have consultant presence for the management of majortrauma during the early hours of Sunday morning on February5th 2006. Furthermore, in only six cases was the consultanta resident and thus immediately available (Table 23).Immediate airway control is vital. Only 111/183 hospitals(60.7%) had an anaesthetic SpR or above immediatelyavailable. <strong>Trauma</strong> airways are likely to be diffi cult and ananaesthetic SpR or above should be present immediately inthe emergency department.The management of the severely injured patient can beextremely challenging and rapid, accurate communication ofall aspects of care is essential. This is particularly importantgiven that many different specialties may be involved. It canbe seen from Table 24 that only 51/175 hospitals had writtenprotocols covering this important area.Table 24. Communication and handoversWritten protocol forhanding over careClinical teamsClinical specialties% %Yes 59 33.1 51 29.1No 119 66.9 124 70.9Subtotal 178 175Notanswered5 8Total 183 183Over a third (65/183) of hospitals indicated that they did notallocate a named person for communicating with the patient/relatives. This insuffi ciency was refl ected by the individualcases. Where the advisors felt they were able to assess thelevel of communication with the patient/relatives, 31.4%(141/449) of cases were found to be less than satisfactoryfor quantity and quality of communication. This clearlyindicates that a named person of appropriate senioritymust be nominated to the patient/relatives as a point ofcontact. Communication with the patient/relatives must bedocumented to allow all involved with the care of the patientto be aware of the occurrence and content ofthis communication.32