nhs forth valley formulary 11 - Community Pharmacy
nhs forth valley formulary 11 - Community Pharmacy
nhs forth valley formulary 11 - Community Pharmacy

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
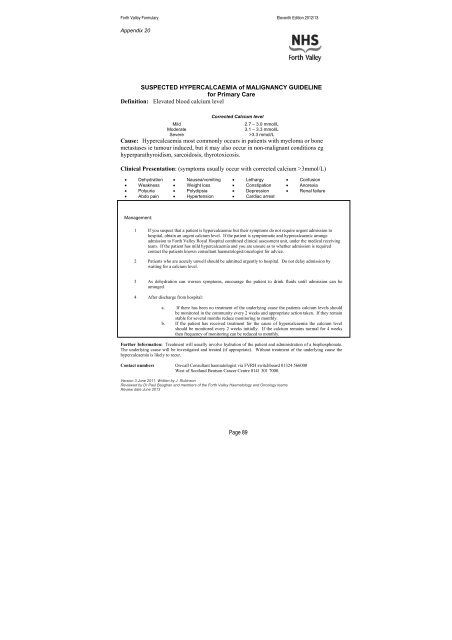
Forth Valley Formulary Eleventh Edition 2012/13Appendix 20SUSPECTED HYPERCALCAEMIA of MALIGNANCY GUIDELINEfor Primary CareDefinition: Elevated blood calcium levelCorrected Calcium levelMild2.7 – 3.0 mmol/LModerate3.1 – 3.3 mmol/LSevere>3.3 mmol/LCause: Hypercalcaemia most commonly occurs in patients with myeloma or bonemetastases ie tumour induced, but it may also occur in non-malignant conditions eghyperparathyroidism, sarcoidosis, thyrotoxicosis.Clinical Presentation: (symptoms usually occur with corrected calcium >3mmol/L)• Dehydration • Nausea/vomiting • Lethargy • Confusion• Weakness • Weight loss • Constipation • Anorexia• Polyuria • Polydipsia • Depression • Renal failure• Abdo pain • Hypertension • Cardiac arrestManagement:1 If you suspect that a patient is hypercalcaemic but their symptoms do not require urgent admission tohospital, obtain an urgent calcium level. If the patient is symptomatic and hypercalcaemic arrangeadmission to Forth Valley Royal Hospital combined clinical assessment unit, under the medical receivingteam. If the patient has mild hypercalcaemia and you are unsure as to whether admission is requiredcontact the patients known consultant haematologist/oncologist for advice.2 Patients who are acutely unwell should be admitted urgently to hospital. Do not delay admission bywaiting for a calcium level.3 As dehydration can worsen symptoms, encourage the patient to drink fluids until admission can bearranged.4 After discharge from hospital:a. If there has been no treatment of the underlying cause the patients calcium levels shouldbe monitored in the community every 2 weeks and appropriate action taken. If they remainstable for several months reduce monitoring to monthly.b. If the patient has received treatment for the cause of hypercalcaemia the calcium levelshould be monitored every 2 weeks initially. If the calcium remains normal for 4 weeksthen frequency of monitoring can be reduced to monthly.Further Information: Treatment will usually involve hydration of the patient and administration of a bisphosphonate.The underlying cause will be investigated and treated (if appropriate). Without treatment of the underlying cause thehypercalcaemia is likely to recur.Contact numbers On-call Consultant haematologist via FVRH switchboard 01324 566000West of Scotland Beatson Cancer Centre 0141 301 7000.Version 3 June 20<strong>11</strong> Written by J. RobinsonReviewed by Dr Paul Baughan and members of the Forth Valley Haematology and Oncology teamsReview date June 2013Page 89