nhs forth valley formulary 11 - Community Pharmacy
nhs forth valley formulary 11 - Community Pharmacy
nhs forth valley formulary 11 - Community Pharmacy

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
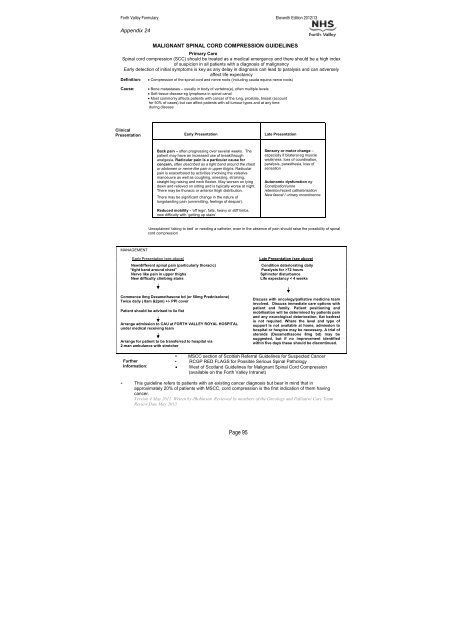
Forth Valley Formulary Eleventh Edition 2012/13Appendix 24MALIGNANT SPINAL CORD COMPRESSION GUIDELINESPrimary CareSpinal cord compression (SCC) should be treated as a medical emergency and there should be a high indexof suspicion in all patients with a diagnosis of malignancyEarly detection of initial symptoms is key as any delay in diagnosis can lead to paralysis and can adverselyaffect life expectancyDefinition: • Compression of the spinal cord and nerve roots (including cauda equina nerve roots)Cause:• Bone metastases – usually in body of vertebra(e), often multiple levels• Soft tissue disease eg lymphoma in spinal canal• Most commonly affects patients with cancer of the lung, prostate, breast (accountfor 50% of cases) but can affect patients with all tumour types and at any timeduring diseaseClinicalPresentationEarly PresentationLate PresentationBack pain – often progressing over several weeks. Thepatient may have an increased use of breakthroughanalgesia. Radicular pain is a particular cause forconcern, often described as a tight band around the chestor abdomen or nerve-like pain in upper thighs. Radicularpain is exacerbated by activities involving the valsalvamanoeuvre as well as coughing, sneezing, straining,straight leg raising and neck flexion. May worsen on lyingdown and relieved on sitting and is typically worse at night.There may be thoracic or anterior thigh distribution.There may be significant change in the nature oflongstanding pain (unremitting, feelings of despair).Reduced mobility - ‘off legs’, falls, heavy or stiff limbs,new difficulty with ‘getting up stairs’Sensory or motor change –especially if bilateral eg muscleweakness, loss of coordination,paralysis, parasthesia, loss ofsensationAutonomic dysfunction egConstipation/urineretention/recent catheterisationNew faecal / urinary incontinenceUnexplained ‘taking to bed’ or needing a catheter, even in the absence of pain should raise the possibility of spinalcord compressionMANAGEMENTEarly Presentation (see above)New/different spinal pain (particularly thoracic)“tight band around chest”Nerve like pain in upper thighsNew difficulty climbing stairsLate Presentation (see above)Condition deteriorating dailyParalysis for >72 hoursSphincter disturbanceLife expectancy < 4 weeksCommence 8mg Dexamethasone bd (or 50mg Prednisolone)Twice daily ( 8am &2pm) +/- PPI coverPatient should be advised to lie flatArrange admission to CAU at FORTH VALLEY ROYAL HOSPITALunder medical receiving teamArrange for patient to be transferred to hospital via2-man ambulance with stretcherDiscuss with oncology/palliative medicine teaminvolved. Discuss immediate care options withpatient and family. Patient positioning andmobilisation will be determined by patients painand any neurological deterioration, flat bedrestis not required. Where the level and type ofsupport is not available at home, admission tohospital or hospice may be necessary. A trial ofsteroids (Dexamethasone 8mg bd) may besuggested, but if no improvement identifiedwithin five days these should be discontinued.• MSCC section of Scottish Referral Guidelines for Suspected CancerFurther• RCGP RED FLAGS for Possible Serious Spinal PathologyInformation: • West of Scotland Guidelines for Malignant Spinal Cord Compression(available on the Forth Valley Intranet)• This guideline refers to patients with an existing cancer diagnosis but bear in mind that inapproximately 20% of patients with MSCC, cord compression is the first indication of them havingcancer.Version 4 May 20<strong>11</strong> Writen by JRobinson Reviewed by members of the Oncology and Palliative Care TeamReview Date May 2013Page 95