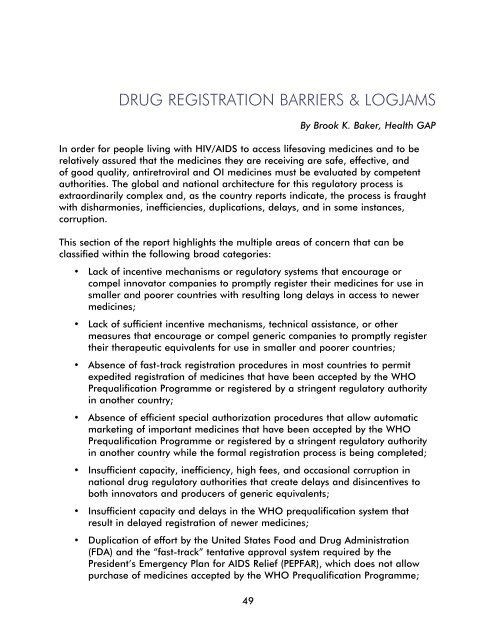
DRUG REGISTRATION BARRIERS & LOGJAMS49By Brook K. Baker, Health GAPIn order for people living with HIV/<strong>AIDS</strong> to access lifesaving medicines and to berelatively assured that <strong>the</strong> medicines <strong>the</strong>y are receiving are safe, effective, andof good quality, antiretroviral and OI medicines must be evaluated by competentauthorities. The global and national architecture for this regulatory process isextraordinarily complex and, as <strong>the</strong> country reports indicate, <strong>the</strong> process is fraughtwith disharmonies, inefficiencies, duplications, delays, and in some instances,corruption.This section of <strong>the</strong> report highlights <strong>the</strong> multiple areas of concern that can beclassified within <strong>the</strong> following broad categories:• Lack of incentive mechanisms or regulatory systems that encourage orcompel innovator companies to promptly register <strong>the</strong>ir medicines for use insmaller and poorer countries with resulting long delays in access to newermedicines;• Lack of sufficient incentive mechanisms, technical assistance, or o<strong>the</strong>rmeasures that encourage or compel generic companies to promptly register<strong>the</strong>ir <strong>the</strong>rapeutic equivalents for use in smaller and poorer countries;• Absence of fast-track registration procedures in most countries to permitexpedited registration of medicines that have been accepted by <strong>the</strong> WHOPrequalification Programme or registered by a stringent regulatory authorityin ano<strong>the</strong>r country;• Absence of efficient special authorization procedures that allow automaticmarketing of important medicines that have been accepted by <strong>the</strong> WHOPrequalification Programme or registered by a stringent regulatory authorityin ano<strong>the</strong>r country while <strong>the</strong> formal registration process is being completed;• Insufficient capacity, inefficiency, high fees, and occasional corruption innational drug regulatory authorities that create delays and disincentives toboth innovators and producers of generic equivalents;• Insufficient capacity and delays in <strong>the</strong> WHO prequalification system thatresult in delayed registration of newer medicines;• Duplication of effort by <strong>the</strong> United States Food and <strong>Drug</strong> Administration(FDA) and <strong>the</strong> “fast-track” tentative approval system required by <strong>the</strong>President’s Emergency Plan for <strong>AIDS</strong> Relief (PEPFAR), which does not allowpurchase of medicines accepted by <strong>the</strong> WHO Prequalification Programme;
• Data exclusivity and registration/patent linkage rules, which in <strong>the</strong>ir mostabsolute form can prevent registration of follow-on generic products;• Lack of post-approval quality assurance mechanisms and lack of efficientsupervision of <strong>the</strong> marketing of medicine to prevent <strong>the</strong> use of substandardor counterfeit medicines 1 ; and• Lack of a global, up-to-date, accessible registry on registration status of HIV/<strong>AIDS</strong> medicines.In addressing <strong>the</strong>se myriad problems, both international and national authoritiesbear responsibility to expedite and rationalize <strong>the</strong> assessment and registrationof lifesaving medicines. In this regard, this section of <strong>the</strong> report considers <strong>the</strong>performance of key international institutions, including WHO, UNITAID, PEPFAR, <strong>the</strong>Clinton Foundation, and o<strong>the</strong>rs, to highlight areas of progress and fur<strong>the</strong>r work tobe done. In addition, this chapter highlights key regulatory reforms needed at <strong>the</strong>local level to ensure that PLWHA receive good quality medicines.The perverse registration practices of innovator pharmaceutical companiesThe current regulatory regime for country-by-country registration of medicinesprovides few if any incentives or requirements for drug companies to register newmedicines in a particular market o<strong>the</strong>r than <strong>the</strong> purely profit-driven motive ofwhe<strong>the</strong>r registration will be worth <strong>the</strong> time, effort, and money (Morocco, China).As <strong>the</strong> report from Morocco states, drug companies do not register <strong>the</strong>ir new HIV/<strong>AIDS</strong> medicines in smaller markets or in countries with small numbers of PLWHA.Accordingly, <strong>the</strong> country reports indicate that atazanavir (ATV), tenofovir (TDF),emtricitabine (FTC), lopinavir (LPV), ritonavir (r), and efavirenz + emtricitabine+ tenofovir (Atripla), some of <strong>the</strong> most important, newer first- and second-linemedicines, are currently not registered separately or as appropriate combinations,in most countries. 21 The term “counterfeit medicine” does not apply to legitimate generic equivalents of innovatordrugs, but is limited to medicines that are deliberately and fraudulently mislabeled, that often donot contain any or <strong>the</strong> correct amounts of active ingredients and expedients claimed, and that are<strong>the</strong>refore dangerous and/or ineffective for patients.2 Abbott claims that its Kaletra capsule has been registered in 118 countries, and that it has filedfor registration in 135 countries for Aluvia tablets and had obtained 89 approvals as of June 2007.Abbott claims it will seek to register Aluvia in over 150 countries. Just this November, Gileadposted country-by-country registration status of TDF (tenofovir - Viread®) and TDF/FTC (tenofovir/emtricitabine - Truvada®) in its International <strong>Access</strong> Operations. See http://www.gilead.com/pdf/GAP_Registration_Status.pdf. As of November 13, 2007, TDF had been approved in 43countries, been filed in ano<strong>the</strong>r 35, but not filed in 51; TDF/FTC has been approved in 36 countries,filed in 34, and pending submission in 59. It should clearly become an industry standard thatcompanies list country-by-country registration status on a publicly accessible website.50
- Page 1 and 2:
Missing the Target #5:Improving AID
- Page 4 and 5:
ArgentinaDr. María Lorena Di Giano
- Page 8 and 9: Executive SummaryAt the G8 meeting
- Page 12: • UN agencies should provide incr
- Page 16 and 17: Price should not be a barrier when
- Page 18 and 19: The Global Fund and UNITAID: The Fu
- Page 20 and 21: The real cost of free treatmentBy a
- Page 22 and 23: Remaining work for asuccessful prog
- Page 24 and 25: DOMINICAN REPUBLICto access rapid t
- Page 26 and 27: DOMINICAN REPUBLICIn Santo Domingo
- Page 28 and 29: ZIMBABWEtreatment, representing 35
- Page 30 and 31: ZIMBABWEAccording to the Medicines
- Page 32 and 33: ZIMBABWEZimbabwe’s application fo
- Page 34 and 35: ZIMBABWENational government• Addr
- Page 36 and 37: RUSSIAMigrantsRussia, with the seco
- Page 38 and 39: a person with HIV will die very qui
- Page 40 and 41: FamiliesIn Kenya, families are the
- Page 42 and 43: INDIA2. Provide pediatric formulati
- Page 44 and 45: Linking nutrition and treatmentBy W
- Page 46 and 47: Most people living with advanced HI
- Page 48 and 49: only available in the capital, Yaou
- Page 50 and 51: ZAMBIAFindings in particular provin
- Page 52 and 53: The DACA for Chadiza District was a
- Page 54 and 55: Many health care workers are inadeq
- Page 58 and 59: Country ATV RLPV/rLPV/r(HS)TDFArgen
- Page 60 and 61: development and registration. Likew
- Page 62 and 63: Capacity issues and delays in the W
- Page 64 and 65: Lack of post-approval quality assur
- Page 66 and 67: ARV PROCUREMENT, REGISTRATION,AND S
- Page 68 and 69: ARGENTINAParallel importingRelating
- Page 70 and 71: ARGENTINAAccess to ARVsNo difficult
- Page 72 and 73: Viral load tests are available, but
- Page 74 and 75: Cambodiaby Mony PenOnly pharmacists
- Page 76 and 77: ChinaBy anonymous Missing the Targe
- Page 78 and 79: CHINAThe current process for regist
- Page 80 and 81: Dominican RepublicBy Eugene Schiff
- Page 82 and 83: IndiaBy Abraham KK, Celina D’Cost
- Page 84 and 85: MalawiBy Lot Nyirenda and Grace Bon
- Page 86 and 87: MALAWIStock-outsAccording to an ext
- Page 88 and 89: MoroccoBy Othman MelloukMorocco has
- Page 90 and 91: Determine the patent status of all
- Page 92 and 93: MOROCCOThe shortage occurred becaus
- Page 94 and 95: As of November 2007, the unit cost
- Page 96 and 97: NIGERIADiagnostic testsDiagnostic t
- Page 98 and 99: The government’s initial inabilit
- Page 100 and 101: Increase training and capacity buil
- Page 102 and 103: treatment practice. The Minster ann
- Page 104 and 105: Ugandaby Richard Hasunira, Prima Ka
- Page 106 and 107:
UGANDAExtracts from the MoH’s rep
- Page 108 and 109:
ZAMBIAIn gathering this information
- Page 110 and 111:
However, since manufacturing prices
- Page 112 and 113:
105SHORT SUMMARY
- Page 114:
PAKISTANAccess for marginalized gro