INFANT OF A DIABETIC MOTHERBY JEFFREY COOPER, MDIn our society, where diabetes <strong>and</strong> obesity problems areincreasing (no pun intended), we are seeing more <strong>and</strong> moreinfants born to diabetic mothers. This presents a unique setof challenges to the practitioner caring for these infants afterbirth. Improved maternal care during pregnancy may reducesome neonatal morbidities (hypoglycemia, polycythemia,hyperviscosity, intrauterine growth restriction), as well as fetalmacrosomia with consequent birth trauma. The following isa review of the care of the infant born to a diabetic mother(IDM).Macrosomia is the hallmark of diabetic pregnancy. Despitecontinued advances to normalize glucose concentrationsin mothers, fetal overgrowth occurs more than in normalpregnancies. As glucose passes across the placenta viafacilitated diffusion, maternal insulin does not cross. Thisrequires the infant to produce its own increased insulinsupply to utilize the glucose. This increase in insulin primarilystimulates adipose tissue. Brain <strong>and</strong> head growth tend to bespared, while shoulder size increases due to intrascapular fatdevelopment. IDMs have 50% more total body fat comparedwith infants of mothers with normal metabolism making themat increased risk for shoulder dystocia. They also have anincreased abdominal girth due to hepatomegaly from insulindrivingglycogen storage.Hypoglycemia occurs shortly after delivery, as the infant hasbeen receiving a steady state of glucose from the placenta.Once the cord is clamped, the infant transitions to using itsown glucose stored as glycogen or relying on glucose from oralintake. The insulin levels do not drop off immediately <strong>and</strong> theinfant requires sufficient glucose to prevent hypoglycemia.The goal of management should be to deliver enough glucoseto achieve normoglycemia while avoiding stimulation of thepancreas to produce more insulin.Hypocalcemia has also been observed, <strong>and</strong> infants may beasymptomatic, jittery or rarely, develop seizures. Recentdata may point to maternal diabetes causing urinary loss ofmagnesium, which blunts parathyroid hormone secretioncausing neonatal hypocalcemia.Respiratory distress syndrome (RDS) is another potentialproblem of IDMs. Fetal hyperinsulinemia impedes production<strong>and</strong> release of surfactant into the lungs. Previous inaccurateestimates of gestational age due to macrosomia resulted inpreterm delivery with associated RDS.IDMs are at increased risk for polycythemia <strong>and</strong> possiblehyperviscosity syndrome in the neonatal period. Erythroidprecursors tend to be sensitive to insulin which causes anincreased number of RBCs in the circulation. Hyperviscosityresulting from polycythemia may cause renal vein thrombosis,stroke, <strong>and</strong> other organ damage.Due to high red cell mass, hyperbilirubinemia is commonin IDMs. In addition, macrosomic infants tend to bebruised at delivery, <strong>and</strong> resorption of that blood can lead tohyperbilirubinemia.These infants are also at risk for cardiomyopathy, includingthickened interventricular septum <strong>and</strong> left or right ventricularwall. Rarely, they present with aortic outflow obstructionsufficient enough to cause left ventricular failure. Mostabnormalities resolve within the first year.Finally, IDMs are at an increased risk for congenitalmalformations, such as cardiac anomalies, spinal agenesiscaudalregression syndrome, neural tube defects, <strong>and</strong>gastrointestinal <strong>and</strong> urinary tract anomalies. Neonatal smallleft colon is a transient finding in IDMs. They present withintestinal obstruction with a Hirschsprung-like radiograph;however, they have normal bowel innervation. Eventually,they develop normal function.There should be a clear <strong>and</strong> organized plan for delivery.St<strong>and</strong>ard NRP protocol should be initiated at every delivery.Practitioners should be prepared for a possible shoulderdystocia, with resultant birth injury, <strong>and</strong>/or asphyxia during avaginal delivery. Care should be taken to properly document1 <strong>and</strong> 5 minute APGAR scores <strong>and</strong> look at cord blood gases ifasphyxia is a concern. Injury to the brachial plexus could causeproblems from damage to the nerves of the arm to unilateraldiaphragmatic paralysis if the phrenic nerve is affected.Respiratory distress syndrome (RDS) is a common complicationso the practitioner should be <strong>read</strong>y to appropriately ventilatethe patient with CPAP, PPV, or intubation as needed.Signs <strong>and</strong> symptoms of hypoglycemia are nonspecific<strong>and</strong> infants may not be symptomatic. Symptoms includejitteriness, agitation, poor feeding, lethargy, seizures, apnea,grunting <strong>and</strong> sweating. A plasma glucose should be checked ininfants of diabetic mothers, even in the absence of symptoms.As the plasma glucose concentration drops rapidly afterdelivery, a glucose level should be obtained within 30 minutesafter birth. Guidelines for the close glucose monitoring <strong>and</strong>VOL. 27 NO. 1 | MARCH <strong>2013</strong>
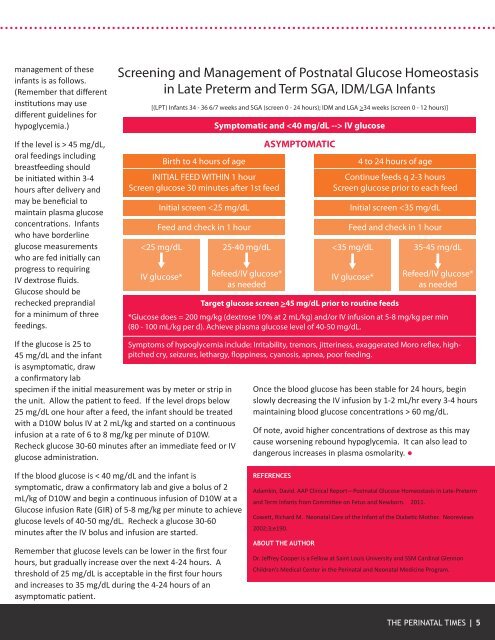
management of theseinfants is as follows.(Remember that differentinstitutions may usedifferent guidelines forhypoglycemia.)If the level is > 45 mg/dL,oral feedings includingbreastfeeding shouldbe initiated within 3-4hours after delivery <strong>and</strong>may be beneficial tomaintain plasma glucoseconcentrations. Infantswho have borderlineglucose measurementswho are fed initially canprogress to requiringIV dextrose fluids.Glucose should berechecked prepr<strong>and</strong>ialfor a minimum of threefeedings.Screening <strong>and</strong> Management of Postnatal Glucose Homeostasisin Late Preterm <strong>and</strong> Term SGA, IDM/LGA Infants[(LPT) Infants 34 - 36 6/7 weeks <strong>and</strong> SGA (screen 0 - 24 hours); IDM <strong>and</strong> LGA >34 weeks (screen 0 - 12 hours)]Birth to 4 hours of ageINITIAL FEED WITHIN 1 hourScreen glucose 30 minutes after 1st feedInitial screen