

perinatal-times_2013-03_print_and_read - SSM Cardinal Glennon ...
perinatal-times_2013-03_print_and_read - SSM Cardinal Glennon ...
perinatal-times_2013-03_print_and_read - SSM Cardinal Glennon ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
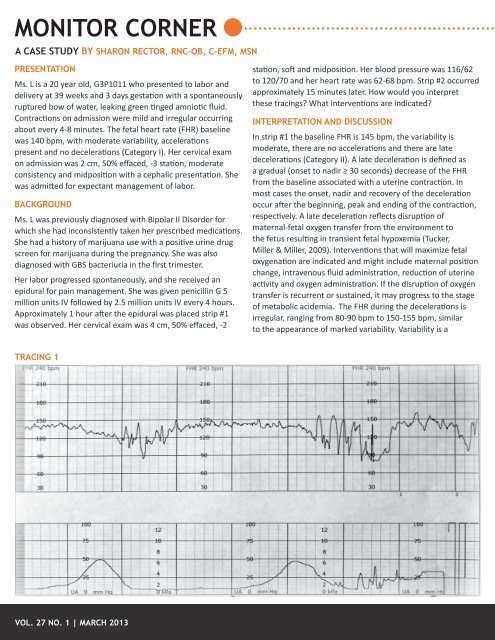
MONITOR CORNERA CASE STUDY BY SHARON RECTOR, RNC-OB, C-EFM, MSNPRESENTATIONMs. L is a 20 year old, G3P1011 who presented to labor <strong>and</strong>delivery at 39 weeks <strong>and</strong> 3 days gestation with a spontaneouslyruptured bow of water, leaking green tinged amniotic fluid.Contractions on admission were mild <strong>and</strong> irregular occurringabout every 4-8 minutes. The fetal heart rate (FHR) baselinewas 140 bpm, with moderate variability, accelerationspresent <strong>and</strong> no decelerations (Category I). Her cervical examon admission was 2 cm, 50% effaced, -3 station, moderateconsistency <strong>and</strong> midposition with a cephalic presentation. Shewas admitted for expectant management of labor.BACKGROUNDMs. L was previously diagnosed with Bipolar II Disorder forwhich she had inconsistently taken her prescribed medications.She had a history of marijuana use with a positive urine drugscreen for marijuana during the pregnancy. She was alsodiagnosed with GBS bacteriuria in the first trimester.Her labor progressed spontaneously, <strong>and</strong> she received anepidural for pain management. She was given penicillin G 5million units IV followed by 2.5 million units IV every 4 hours.Approximately 1 hour after the epidural was placed strip #1was observed. Her cervical exam was 4 cm, 50% effaced, -2station, soft <strong>and</strong> midposition. Her blood pressure was 116/62to 120/70 <strong>and</strong> her heart rate was 62-68 bpm. Strip #2 occurredapproximately 15 minutes later. How would you interpretthese tracings? What interventions are indicated?INTERPRETATION AND DISCUSSIONIn strip #1 the baseline FHR is 145 bpm, the variability ismoderate, there are no accelerations <strong>and</strong> there are latedecelerations (Category II). A late deceleration is defined asa gradual (onset to nadir ≥ 30 seconds) decrease of the FHRfrom the baseline associated with a uterine contraction. Inmost cases the onset, nadir <strong>and</strong> recovery of the decelerationoccur after the beginning, peak <strong>and</strong> ending of the contraction,respectively. A late deceleration reflects disruption ofmaternal-fetal oxygen transfer from the environment tothe fetus resulting in transient fetal hypoxemia (Tucker,Miller & Miller, 2009). Interventions that will maximize fetaloxygenation are indicated <strong>and</strong> might include maternal positionchange, intravenous fluid administration, reduction of uterineactivity <strong>and</strong> oxygen administration. If the disruption of oxygentransfer is recurrent or sustained, it may progress to the stageof metabolic acidemia. The FHR during the decelerations isirregular, ranging from 80-90 bpm to 150-155 bpm, similarto the appearance of marked variability. Variability is aTRACING 1VOL. 27 NO. 1 | MARCH <strong>2013</strong>













