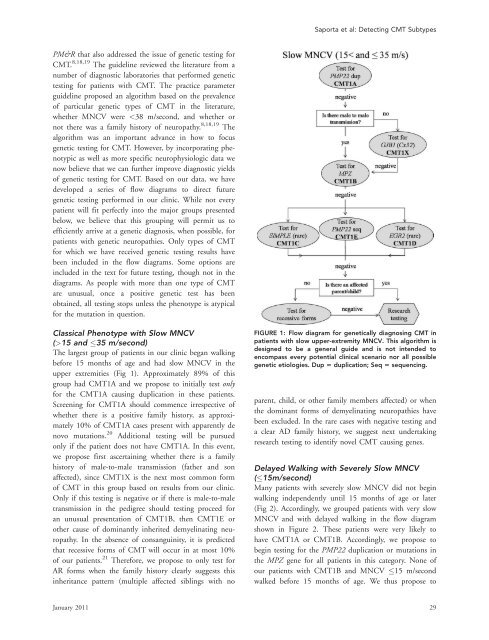
Saporta et al: Detecting CMT SubtypesPM&R that also addressed the issue of <strong>genetic</strong> testing forCMT. 8,18,19 The guideline reviewed the literature from anumber of diagnostic laboratories that performed <strong>genetic</strong>testing for patients with CMT. The practice parameterguideline proposed an algorithm based on the prevalenceof particular <strong>genetic</strong> types of CMT in the literature,whether MNCV were 15 <strong>and</strong> 35 m/second)The largest group of patients in our clinic began walkingbefore 15 months of age <strong>and</strong> had slow MNCV in theupper extremities (Fig 1). Approximately 89% of thisgroup had CMT1A <strong>and</strong> we propose to initially test onlyfor the CMT1A causing duplication in these patients.Screening for CMT1A should commence irrespective ofwhether there is a positive family history, as approximately10% of CMT1A cases present with apparently denovo mutations. 20 Additional testing will be pursuedonly if the patient does not have CMT1A. In this event,we propose first ascertaining whether there is a familyhistory of male-to-male transmission (father <strong>and</strong> sonaffected), since CMT1X is the next most common formof CMT in this group based on results from our clinic.Only if this testing is negative or if there is male-to-maletransmission in the pedigree should testing proceed foran unusual presentation of CMT1B, then CMT1E orother cause of dominantly inherited demyelinating neuropathy.In the absence of consanguinity, it is predictedthat recessive forms of CMT will occur in at most 10%of our patients. 21 Therefore, we propose to only test forAR forms when the family history clearly suggests thisinheritance pattern (multiple affected siblings with noFIGURE 1: Flow diagram for <strong>genetic</strong>ally diagnosing CMT inpatients with slow upper-extremity MNCV. This algorithm isdesigned to be a general guide <strong>and</strong> is not intended toencompass every potential clinical scenario nor all possible<strong>genetic</strong> etiologies. Dup 5 duplication; Seq 5 sequencing.parent, child, or other family members affected) or whenthe dominant forms of demyelinating neuropathies havebeen excluded. In the rare cases with negative testing <strong>and</strong>a clear AD family history, we suggest next undertakingresearch testing to identify novel CMT causing genes.Delayed Walking with Severely Slow MNCV(15m/second)Many patients with severely slow MNCV did not beginwalking independently until 15 months of age or later(Fig 2). Accordingly, we grouped patients with very slowMNCV <strong>and</strong> with delayed walking in the flow diagramshown in Figure 2. These patients were very likely tohave CMT1A or CMT1B. Accordingly, we propose tobegin testing for the PMP22 duplication or mutations inthe MPZ gene for all patients in this category. None ofour patients with CMT1B <strong>and</strong> MNCV 15 m/secondwalked before 15 months of age. We thus propose toJanuary 2011 29
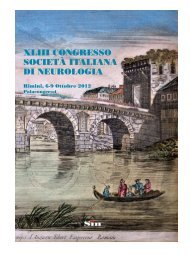
ANNALS of Neurologywhether to next test for AR disorders or whether researchtesting for novel genes is more appropriate.FIGURE 2: Flow diagram for <strong>genetic</strong>ally diagnosing CMT inpatients with very slow upper-extremity MNCV. Thisalgorithm is designed to be a general guide <strong>and</strong> is notintended to encompass every potential clinical scenario norall possible <strong>genetic</strong> etiologies. Dup 5 duplication; Seq 5sequencing.begin testing for only CMT1A for patients who havevery slow nerve conductions <strong>and</strong> walked before 15months of age. If this testing is negative, the next mostcommon cause of CMT for this group is CMT1B in ourclinic population. Because AD neuropathy is much morefrequent than AR neuropathy in our clinic population,we again propose continuing with AD disorders, even ifthere is no obvious family history of CMT. If there is noPMP22 duplication <strong>and</strong> if MPZ sequencing is normal wesuggest sequencing PMP22 (CMT1E), a less frequentcause of this presentation. Only if these tests are negativeshould testing proceed to CMT1C <strong>and</strong> CMT1D, veryrare forms of CMT1 in our patient group. If testing forthese is also negative, the presence or absence of anaffected parent or child can be used to determineCMT with Intermediate MNCV(>35 <strong>and</strong> 45 m/second)Patients with identified <strong>genetic</strong> causes of CMT who hadintermediate MNCV had primarily CMT1X or CMT1B(Fig 3). For patients with intermediate MNCV, the firststep is to determine whether the phenotype is classical oradult onset <strong>and</strong> then whether there is evidence of maleto-maletransmission. For patients with no male-to-maletransmission, intermediate conductions, <strong>and</strong> a classicalphenotype, the first test should be for GJB1 mutations(CMT1X) (78% of our clinic population with this phenotypehas these mutations). If this testing is negative,testing should proceed to MPZ mutations. Alternatively,if there is male-to-male transmission, testing for CMT1Bshould occur first since the inheritance pattern wouldformally exclude CMT1X. If patients with intermediateMNCV first develop symptoms in adulthood, testingshould begin with CMT1B, as this is most likely accordingto our results. As no patients with CMT1A had intermediateconduction velocities, testing for a PMP22duplication would not be warranted. If all testing is negative,the presence or absence of an affected parent orchild can be used to determine whether to next test forrare or AR disorders or whether research testing for novelgenes is more appropriate. Some rare genes for the dominantintermediate forms of CMT include DNM2 (DI-CMTB) <strong>and</strong> YARS (DI-CMTC) mutations. These arenot included on the flow diagram because there are no<strong>genetic</strong>ally confirmed cases of these in our clinic. However,it is possible that they will make up a clinically significantpart of the CMT population in the future, <strong>and</strong>these flowcharts can be altered to reflect that. Patientswith HNPP were identified in the intermediate NCVgroup with childhood <strong>and</strong> adult onset of symptoms.This disorder was not included in Figure 3 (or Fig 4)because of its characteristic presentation of focal episodesof weakness or sensory loss <strong>and</strong> focal slowing of MNCVthat distinguish it from other forms of CMT. These clinical<strong>and</strong> physiological findings should, by themselves,suggest testing for HNPP. 22,23Targeted Testing for Normal orUnobtainable NCVPatients with CMT2A were frequently severely affectedin infancy <strong>and</strong> childhood (see Table 6) to the extent thattheir CMAP amplitudes <strong>and</strong> NCV were unobtainable bytesting in the upper extremities (see Table 7, Table 8,<strong>and</strong> Fig 4), Since patients with CMT2A form our largestgroup of patients with CMT2 (Feely, unpublished30 Volume 69, No. 1