Furie et al <strong>Prevention</strong> <strong>of</strong> <strong>Stroke</strong> <strong>in</strong> Patients With <strong>Stroke</strong> and TIA 237<strong>of</strong> <strong>the</strong>se major trials showed that <strong>for</strong> patients with stenoses <strong>of</strong>50%, surgical <strong>in</strong>tervention did not <strong>of</strong>fer benefit <strong>in</strong> terms <strong>of</strong>reduction <strong>of</strong> stroke risk.Controversy exists <strong>for</strong> patients with symptomatic stenoses<strong>in</strong> <strong>the</strong> range <strong>of</strong> 50% to 69%. Among symptomatic NASCETpatients with a stenosis <strong>of</strong> 50% to 69%, <strong>the</strong> 5-year rate <strong>of</strong>any ipsilateral stroke was 15.7% <strong>in</strong> patients treated surgicallycompared with 22.2% <strong>in</strong> those treated medically(P0.045). 179 Thus, to prevent 1 ipsilateral stroke dur<strong>in</strong>g <strong>the</strong>5-year follow-up, 15 patients would have to undergo CEA. 179The conclusions justify use <strong>of</strong> CEA only with appropriatecase selection when <strong>the</strong> risk-benefit ratio is favorable <strong>for</strong> <strong>the</strong>patient. Patients with a moderate (50% to 69%) stenosis whoare at reasonable surgical and anes<strong>the</strong>tic risk may benefitfrom an <strong>in</strong>tervention per<strong>for</strong>med by a surgeon with excellentoperative skills and a perioperative morbidity and mortalityrate <strong>of</strong> 6%. 180Patient Selection Criteria Influenc<strong>in</strong>g Surgical RiskThe effect <strong>of</strong> sex on CEA results has been controversial.Some studies have identified a clear gender effect on perioperativestroke and death rates, though many such seriescomb<strong>in</strong>e both asymptomatic and symptomatic patients. Subgroupanalyses <strong>of</strong> <strong>the</strong> NASCET trial questions <strong>the</strong> benefit <strong>of</strong>CEA <strong>in</strong> symptomatic women, although women were not wellrepresented and <strong>the</strong> effect <strong>of</strong> sex was not overwhelm<strong>in</strong>g. 179,181These data suggest that women are more likely to have lessfavorable outcomes, <strong>in</strong>clud<strong>in</strong>g surgical mortality, neurologicalmorbidity, and recurrent carotid stenosis (14% <strong>in</strong> womenversus 3.9% <strong>in</strong> men, P0.008). 182 It has also been hypo<strong>the</strong>sizedthat women are more prone to develop recurrentstenosis due to smaller-caliber vessels, particularly withpatch<strong>in</strong>g, although this rema<strong>in</strong>s controversial. Of course,outcome differences <strong>in</strong> age and sex, along with medicalcomorbidities, must be considered when decid<strong>in</strong>g whe<strong>the</strong>r ornot to proceed with carotid revascularization.With modern perioperative care and anes<strong>the</strong>tic techniques,<strong>the</strong> effects <strong>of</strong> age and controlled medical comorbidities onoutcomes follow<strong>in</strong>g CEA are also ambiguous. Though octogenarianswere excluded from <strong>the</strong> NASCET, case series havedocumented <strong>the</strong> safety <strong>of</strong> CEA <strong>in</strong> those 80 years <strong>of</strong> age. 183Tim<strong>in</strong>g <strong>of</strong> Carotid RevascularizationThe tim<strong>in</strong>g <strong>of</strong> CEA after an acute neurological event rema<strong>in</strong>scontroversial, with experts advocat<strong>in</strong>g wait<strong>in</strong>g anywherefrom 2 to 6 weeks. The optimal tim<strong>in</strong>g <strong>for</strong> CEA after a m<strong>in</strong>oror nondisabl<strong>in</strong>g stroke with stabilized or improv<strong>in</strong>g neurologicaldeficits has been a subject <strong>of</strong> much debate. Thoserecommend<strong>in</strong>g early CEA (with<strong>in</strong> 6 weeks) report excellentresults without an <strong>in</strong>creased risk <strong>of</strong> recurrent stroke. Early<strong>in</strong>tervention may be beneficial <strong>in</strong> those without <strong>in</strong>itial evidence<strong>of</strong> <strong>in</strong>traparenchymal bra<strong>in</strong> hemorrhage. Very early<strong>in</strong>tervention (3 weeks) may also be per<strong>for</strong>med safely <strong>in</strong>low-risk patients with TIAs or m<strong>in</strong>or strokes. 184,185 Pooledanalyses from endarterectomy trials have shown that earlysurgery is associated with <strong>in</strong>creased benefits compared withdelayed surgery. Benefit from surgery was greatest <strong>in</strong> men75 years <strong>of</strong> age and those randomized with<strong>in</strong> 2 weeks after<strong>the</strong>ir last ischemic event; benefit fell rapidly with <strong>in</strong>creas<strong>in</strong>gdelay. 186Carotid Angioplasty and Stent<strong>in</strong>gCAS has emerged as a <strong>the</strong>rapeutic alternative to CEA <strong>for</strong>treatment <strong>of</strong> extracranial carotid artery occlusive disease.Carotid artery angioplasty is a less <strong>in</strong>vasive percutaneousprocedure that was first reported by Kerber et al <strong>in</strong> 1980. 187The expansion <strong>of</strong> this technique to <strong>in</strong>clude stent<strong>in</strong>g has beenunder <strong>in</strong>vestigation <strong>in</strong> <strong>the</strong> United States s<strong>in</strong>ce 1994. 188 Advances<strong>in</strong> endovascular technology, <strong>in</strong>clud<strong>in</strong>g embolic protectiondevices and improved stent design, have resulted <strong>in</strong>improvements <strong>in</strong> <strong>the</strong> technical aspects <strong>of</strong> CAS and improvedoutcomes. Exist<strong>in</strong>g available data suggest success and complicationrates comparable to CEA. 189,190 The proposed advantages<strong>of</strong> CAS are its less <strong>in</strong>vasive nature, decreasedpatient discom<strong>for</strong>t, and a shorter recuperation period, but itsdurability rema<strong>in</strong>s unproven. Cl<strong>in</strong>ical equipoise exists withrespect to its comparison with CEA. Currently, CAS isma<strong>in</strong>ly <strong>of</strong>fered to those patients considered high risk <strong>for</strong> openendarterectomy based on <strong>the</strong> available data from large,multicenter, prospective, randomized studies. High risk isdef<strong>in</strong>ed as (1) patients with severe comorbidities (class III/IVcongestive heart failure, class III/IV ang<strong>in</strong>a, left ma<strong>in</strong> coronaryartery disease, 2-vessel coronary artery disease, leftventricular ejection fraction [LVEF] 30%, recent MI, severelung disease, or severe renal disease), or (2) challeng<strong>in</strong>gtechnical or anatomic factors, such as prior neck operation(ie, radical neck dissection) or neck irradiation, postendarterectomyrestenosis, surgically <strong>in</strong>accessible lesions (ie, aboveC2, below <strong>the</strong> clavicle), contralateral carotid occlusion, contralateralvocal cord palsy, or <strong>the</strong> presence <strong>of</strong> a tracheostomy.Anatomic high risk has generally been accepted, but severalrecent studies have called medical high risk <strong>in</strong>to question,given improved anes<strong>the</strong>tic and critical care management. 191Most reported trials have been <strong>in</strong>dustry sponsored and evaluated<strong>the</strong> efficacy <strong>of</strong> a s<strong>in</strong>gle stent/neuroprotection system. Thefirst large randomized trial was <strong>the</strong> Carotid and Vertebral ArteryTranslum<strong>in</strong>al Angioplasty Study (CAVATAS). 192 In this trial,published <strong>in</strong> 2001, symptomatic patients suitable <strong>for</strong> surgerywere randomly assigned to ei<strong>the</strong>r stent<strong>in</strong>g or surgery. Patientsunsuitable <strong>for</strong> surgery were randomized to ei<strong>the</strong>r stent<strong>in</strong>g ormedical management. CAVATAS showed CAS to havecomparable outcomes to surgery (30-day rate <strong>of</strong> stroke ordeath, 6% <strong>in</strong> both groups); however, only 55 <strong>of</strong> <strong>the</strong> 251patients <strong>in</strong> <strong>the</strong> endovascular group were treated with a stent,and embolic protection devices were not used. Prelim<strong>in</strong>arylong-term data showed no difference <strong>in</strong> <strong>the</strong> rate <strong>of</strong> stroke <strong>in</strong>patients up to 3 years after randomization.Embolic protection devices have reduced periproceduralstroke rates and are required <strong>in</strong> procedures reimbursed by <strong>the</strong>Centers <strong>for</strong> Medicare and Medicaid. The SAPPHIRE trial(Stent<strong>in</strong>g and Angioplasty with Protection <strong>in</strong> Patients at HighRisk <strong>for</strong> Endarterectomy) had <strong>the</strong> primary objective <strong>of</strong>compar<strong>in</strong>g <strong>the</strong> safety and efficacy <strong>of</strong> CAS with an embolicprotection device with CEA <strong>in</strong> 334 symptomatic and asymptomatichigh-risk patients. 193 The perioperative 30-day comb<strong>in</strong>edstroke, death, and MI rates were 9.9% <strong>for</strong> surgeryversus 4.4% <strong>for</strong> stent<strong>in</strong>g. The 1-year primary end po<strong>in</strong>t <strong>of</strong>death, stroke, or MI at 30 days plus ipsilateral stroke or deathdue to neurological causes with<strong>in</strong> 31 days to 1 year was 20.1%<strong>for</strong> surgery and 12.0% <strong>for</strong> stent<strong>in</strong>g (P0.05). Despite <strong>the</strong> factDownloaded from stroke.ahajournals.org by on March 8, 2011
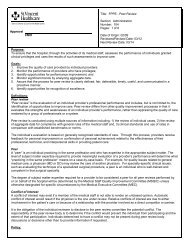
238 <strong>Stroke</strong> January 2011Table 6. Hazard Ratio <strong>for</strong> CAS Versus CEA <strong>in</strong> 1321 Symptomatic Patients byTreatment GroupPeriproceduralHR (95% CI)4-Year Study PeriodHR (95% CI)MI 0.45 (0.18–1.11) …Any periprocedural stroke or postprocedural ipsilateral stroke 1.74 (1.02–2.98) 1.29 (0.84–1.98)Any periprocedural stroke, death, or postprocedural ipsilateral stroke 1.89 (1.11–3.21) 1.37 (0.90–2.09)Any periprocedural stroke, MI, death, or postprocedural ipsilateral stroke 1.26 (0.81–1.96) 1.08 (0.74–1.59)that <strong>the</strong>se differences primarily represented differences <strong>in</strong>periprocedural MI rates, <strong>the</strong> major conclusion from this trial wasthat CAS was not <strong>in</strong>ferior to CEA <strong>in</strong> this specific high-riskpatient cohort. However, only 30% <strong>of</strong> <strong>the</strong> study population wassymptomatic, and no subset analyses were per<strong>for</strong>med.O<strong>the</strong>r randomized trials, EVA-3S (Endarterectomy VersusAngioplasty <strong>in</strong> Patients with Symptomatic Severe CarotidStenosis) and SPACE (Stent-supported Percutaneous Angioplasty<strong>of</strong> <strong>the</strong> Carotid artery versus Endarterectomy), had anon<strong>in</strong>feriority design compar<strong>in</strong>g CAS to CEA <strong>in</strong> symptomaticpatients. 194,195 Both trials were stopped prematurely <strong>for</strong>reasons <strong>of</strong> safety and futility because <strong>of</strong> a higher 30-daystroke and death rate <strong>in</strong> <strong>the</strong> CAS group. In <strong>the</strong> EVA-3S trial,<strong>the</strong> 30-day comb<strong>in</strong>ed stroke and death rate <strong>for</strong> CAS was 9.6%compared with 3.9% <strong>for</strong> CEA, with a relative risk <strong>of</strong> 2.5 <strong>for</strong>any stroke or death <strong>for</strong> CAS. 194 Fur<strong>the</strong>rmore, at 6 months, <strong>the</strong>risk <strong>for</strong> any stroke or death with CAS was 11.7% comparedwith 6.1% with CEA. Both trials have been criticized <strong>for</strong><strong>in</strong>adequate and nonuni<strong>for</strong>m operator experience, which mayhave had a negative impact on CAS.The Carotid Revascularization Endarterectomy versusStent Trial (CREST) was a prospective, randomized trialcompar<strong>in</strong>g <strong>the</strong> efficacy <strong>of</strong> CAS with CEA. Results <strong>of</strong> <strong>the</strong>CREST lead-<strong>in</strong> period demonstrated 30-day stroke and deathrates <strong>for</strong> symptomatic patients comparable to CEA. 196 Interimoutcomes from <strong>the</strong> lead-<strong>in</strong> data, however, showed an <strong>in</strong>creas<strong>in</strong>grisk <strong>of</strong> stroke and death with <strong>in</strong>creas<strong>in</strong>g age (P0.0006):1.7% <strong>of</strong> patients 60 years <strong>of</strong> age, 1.3% <strong>of</strong> patients 60 to 69years <strong>of</strong> age, 5.3% <strong>of</strong> patients 70 to 79 years <strong>of</strong> age, and12.1% <strong>of</strong> patients 80 years <strong>of</strong> age. 196 CREST randomized2502 symptomatic and asymptomatic patients with carotidstenosis (70% by ultrasonography or 50% by angiography)at 117 centers <strong>in</strong> <strong>the</strong> United States and Canada. Therewas no significant difference <strong>in</strong> <strong>the</strong> composite primaryoutcome (30-day rate <strong>of</strong> stroke, death, MI, and 4-yearipsilateral stroke) <strong>in</strong> patients treated with CAS (n1262)versus CEA (n1240; 7.2% versus 6.8%; HR <strong>for</strong> stent<strong>in</strong>g,1.1; 95% CI, 0.81 to 1.51, P0.51) at a median follow-up <strong>of</strong>2.5 years. In symptomatic patients <strong>the</strong> 4-year rate <strong>of</strong> stroke ordeath was 8% with CAS versus 6.4% with CEA (HR, 1.37;P0.14). In <strong>the</strong> first 30 days, <strong>in</strong> symptomatic patients <strong>the</strong> rate<strong>of</strong> any periprocedural stroke or postprocedural ipsilateralstroke was significantly higher <strong>in</strong> <strong>the</strong> CAS group than <strong>in</strong> <strong>the</strong>CEA group (5.50.9% versus 3.20.7%; P0.04). However,<strong>in</strong> symptomatic patients <strong>the</strong> rate <strong>of</strong> MI was higher <strong>in</strong> <strong>the</strong>CEA group (2.30.6% with CEA versus 1.00.4% withCAS; P0.08). Periprocedural and 4-year event hazard ratiosare summarized <strong>in</strong> Table 6. When all patients were analyzed(symptomatic and asymptomatic), <strong>the</strong>re was an <strong>in</strong>teractionbetween age and treatment efficacy (P0.02). For patients70 years <strong>of</strong> age, CAS showed greater efficacy, whereas <strong>for</strong>patients 70 years, CEA results were superior. There was nodifference by sex. 197Extracranial-Intracranial Bypass SurgeryExtracranial-<strong>in</strong>tracranial (EC/IC) bypass surgery was not foundto provide any benefit <strong>for</strong> patients with carotid occlusion or thosewith carotid artery narrow<strong>in</strong>g distal to <strong>the</strong> carotid bifurcation. 198New ef<strong>for</strong>ts are ongo<strong>in</strong>g, us<strong>in</strong>g more sensitive imag<strong>in</strong>g, such as15 O 2 /H 2 15 O positron emission tomography (PET), to selectpatients with <strong>the</strong> greatest hemodynamic compromise <strong>for</strong> arandomized controlled trial us<strong>in</strong>g EC/IC bypass surgery (CarotidOcclusion Surgery Study [COSS]). 198–200Recommendations1. For patients with recent TIA or ischemic stroke with<strong>in</strong><strong>the</strong> past 6 months and ipsilateral severe (70% to 99%)carotid artery stenosis, CEA is recommended if <strong>the</strong>perioperative morbidity and mortality risk is estimatedto be 70%) <strong>in</strong> whom <strong>the</strong> stenosis is difficult to accesssurgically, medical conditions are present thatgreatly <strong>in</strong>crease <strong>the</strong> risk <strong>for</strong> surgery, or when o<strong>the</strong>rspecific circumstances exist, such as radiation<strong>in</strong>ducedstenosis or restenosis after CEA, CAS maybe considered (Class IIb; Level <strong>of</strong> Evidence B).7. CAS <strong>in</strong> <strong>the</strong> above sett<strong>in</strong>g is reasonable when per<strong>for</strong>medby operators with established periproceduralmorbidity and mortality rates <strong>of</strong> 4% to 6%,similar to those observed <strong>in</strong> trials <strong>of</strong> CEA and CAS(Class IIa; Level <strong>of</strong> Evidence B).Downloaded from stroke.ahajournals.org by on March 8, 2011