Furie et al <strong>Prevention</strong> <strong>of</strong> <strong>Stroke</strong> <strong>in</strong> Patients With <strong>Stroke</strong> and TIA 243<strong>in</strong>dicate that ei<strong>the</strong>r <strong>in</strong>creas<strong>in</strong>g <strong>the</strong> <strong>in</strong>tensity <strong>of</strong> anticoagulationor add<strong>in</strong>g an antiplatelet agent provides additional protectionaga<strong>in</strong>st future ischemic events. In addition, both <strong>of</strong> <strong>the</strong>sestrategies are associated with an <strong>in</strong>crease <strong>in</strong> bleed<strong>in</strong>g risk. Forexample, <strong>in</strong> <strong>the</strong> <strong>Stroke</strong> <strong>Prevention</strong> us<strong>in</strong>g an ORal Thromb<strong>in</strong><strong>in</strong>hibitor <strong>in</strong> Atrial Fibrillation study (SPORTIF), AF patientswith prior stroke or TIA who were treated with <strong>the</strong> comb<strong>in</strong>ation<strong>of</strong> aspir<strong>in</strong> and warfar<strong>in</strong> were at considerably higherrisk <strong>of</strong> major bleed<strong>in</strong>g (1.5% per year with warfar<strong>in</strong> and4.95% per year with warfar<strong>in</strong> plus aspir<strong>in</strong>; P0.004) and noreduction <strong>in</strong> ischemic events. 234 High INR values are clearlyassociated with <strong>in</strong>creased risk <strong>of</strong> hemorrhage; risk <strong>of</strong> ICH<strong>in</strong>creases dramatically at INR values 4.0. 229Patients with AF and prior stroke or TIA have <strong>in</strong>creasedstroke risk when oral anticoagulant <strong>the</strong>rapy is temporarily<strong>in</strong>terrupted (typically <strong>for</strong> surgical procedures). The issue <strong>of</strong>whe<strong>the</strong>r to use bridg<strong>in</strong>g <strong>the</strong>rapy with <strong>in</strong>travenous hepar<strong>in</strong> or alow-molecular-weight hepar<strong>in</strong> (LMWH) <strong>in</strong> <strong>the</strong>se situations iscomplex and has been recently reviewed. 238 In general, bridg<strong>in</strong>ganticoagulation is recommended <strong>for</strong> AF patients assessed to beat particularly high risk (stroke or TIA with<strong>in</strong> 3 months,CHADS 2 score <strong>of</strong> 5 or 6, or mechanical or rheumatic valvedisease). The preferred method <strong>for</strong> bridg<strong>in</strong>g is typically LMWHadm<strong>in</strong>istered <strong>in</strong> an outpatient sett<strong>in</strong>g <strong>in</strong> full treatment doses (asopposed to low prophylactic doses). 238About one quarter <strong>of</strong> patients who present with AF andischemic stroke will be found to have o<strong>the</strong>r potential causes<strong>of</strong> <strong>the</strong> stroke, such as carotid stenosis. 239 For <strong>the</strong>se patients,treatment decisions should focus on <strong>the</strong> presumed most likelystroke etiology. In many cases it will be appropriate to <strong>in</strong>itiateanticoagulation because <strong>of</strong> <strong>the</strong> AF, as well as an additional<strong>the</strong>rapy (such as CEA).Recommendations1. For patients with ischemic stroke or TIA withparoxysmal (<strong>in</strong>termittent) or permanent AF, anticoagulationwith a vitam<strong>in</strong> K antagonist (target INR2.5; range, 2.0 to 3.0) is recommended (Class I; Level<strong>of</strong> Evidence A).2. For patients unable to take oral anticoagulants, aspir<strong>in</strong>alone (Class I; Level <strong>of</strong> Evidence A) is recommended.The comb<strong>in</strong>ation <strong>of</strong> clopidogrel plus aspir<strong>in</strong> carries arisk <strong>of</strong> bleed<strong>in</strong>g similar to that <strong>of</strong> warfar<strong>in</strong> and <strong>the</strong>re<strong>for</strong>eis not recommended <strong>for</strong> patients with a hemorrhagiccontra<strong>in</strong>dication to warfar<strong>in</strong> (Class III; Level <strong>of</strong>Evidence B). (New recommendation)3. For patients with AF at high risk <strong>for</strong> stroke (strokeor TIA with<strong>in</strong> 3 months, CHADS 2 score <strong>of</strong> 5 or 6,mechanical or rheumatic valve disease) who requiretemporary <strong>in</strong>terruption <strong>of</strong> oral anticoagulation,bridg<strong>in</strong>g <strong>the</strong>rapy with an LMWH adm<strong>in</strong>istered subcutaneouslyis reasonable (Class IIa; Level <strong>of</strong> EvidenceC). (New recommendation; Table 8)B. Acute MI and LV ThrombusWithout acute reperfusion <strong>the</strong>rapy, <strong>in</strong>tracardiac thrombusoccurs <strong>in</strong> about one third <strong>of</strong> patients <strong>in</strong> <strong>the</strong> first 2 weeks afteranterior MI and <strong>in</strong> an even greater proportion <strong>of</strong> those withlarge <strong>in</strong>farcts <strong>in</strong>volv<strong>in</strong>g <strong>the</strong> LV apex. 224,240–243 In <strong>the</strong> absence<strong>of</strong> anticoagulant <strong>the</strong>rapy, cl<strong>in</strong>ically evident cerebral <strong>in</strong>farctionoccurs <strong>in</strong> approximately 10% <strong>of</strong> patients with LV thrombusfollow<strong>in</strong>g MI. 241 Thrombolytic <strong>the</strong>rapy may result <strong>in</strong> a lower<strong>in</strong>cidence <strong>of</strong> LV thrombus <strong>for</strong>mation, 242,244,245 but <strong>the</strong> magnitude<strong>of</strong> risk reduction is controversial. 246 The rema<strong>in</strong>der <strong>of</strong>ventricular mural thrombi occur <strong>in</strong> patients with chronicventricular dysfunction result<strong>in</strong>g from coronary disease, hypertension,or o<strong>the</strong>r <strong>for</strong>ms <strong>of</strong> dilated cardiomyopathy, wh<strong>of</strong>ace a persistent risk <strong>of</strong> stroke and systemic embolismwhe<strong>the</strong>r or not AF is documented.Over <strong>the</strong> past 20 years, 3 large trials <strong>in</strong>volv<strong>in</strong>g patients withacute <strong>in</strong>ferior and anterior MIs concluded that <strong>in</strong>itial treatmentwith hepar<strong>in</strong> followed by adm<strong>in</strong>istration <strong>of</strong> warfar<strong>in</strong>reduced <strong>the</strong> occurrence <strong>of</strong> cerebral embolism from 3% to 1%compared with no anticoagulation. Differences were statisticallysignificant <strong>in</strong> 2 <strong>of</strong> <strong>the</strong> 3 studies, with a concordant trend<strong>in</strong> <strong>the</strong> third. 242,244,245 Four randomized studies <strong>in</strong>volv<strong>in</strong>gpatients with acute MI have addressed <strong>the</strong> relationship <strong>of</strong>echocardiographically detected LV thrombus and cerebralembolism. 247–250 In aggregate, thrombus <strong>for</strong>mation was reducedby 50% with anticoagulation; <strong>in</strong>dividually, however,each trial had <strong>in</strong>sufficient sample size to detect significantdifferences <strong>in</strong> embolism.On <strong>the</strong> basis <strong>of</strong> available cl<strong>in</strong>ical trial results, Class Irecommendations have been promulgated <strong>for</strong> oral anticoagulanttreatment <strong>of</strong> patients with echocardiographically detectedLV thrombi after anterior MI. There is no consensusregard<strong>in</strong>g <strong>the</strong> duration <strong>of</strong> anticoagulant treatment. 251 Thepersistence <strong>of</strong> stroke risk <strong>for</strong> several months after <strong>in</strong>farction<strong>in</strong> <strong>the</strong>se patients is suggested by aggregate results <strong>of</strong> a number<strong>of</strong> studies, but alternative antithrombotic regimens have notbeen systematically evaluated. The risk <strong>of</strong> thromboembolismseems to decrease after <strong>the</strong> first 3 months, and <strong>in</strong> patients withchronic ventricular aneurysm, <strong>the</strong> risk <strong>of</strong> embolism is comparativelylow, even though <strong>in</strong>tracardiac thrombi occur frequently<strong>in</strong> this condition.Recommendation1. Patients with ischemic stroke or TIA <strong>in</strong> <strong>the</strong> sett<strong>in</strong>g <strong>of</strong>acute MI complicated by LV mural thrombus <strong>for</strong>mationidentified by echocardiography or ano<strong>the</strong>rcardiac imag<strong>in</strong>g technique should be treated withoral anticoagulation (target INR 2.5, range 2.0 to3.0) <strong>for</strong> at least 3 months (Class I; Level <strong>of</strong> EvidenceB) (Table 8).C. CardiomyopathyAlthough numeric estimates are difficult to verify, approximately10% <strong>of</strong> patients with ischemic stroke have an LVEF30%. 252 The first randomized trial to study warfar<strong>in</strong> <strong>in</strong>patients with heart failure <strong>in</strong> <strong>the</strong> era <strong>of</strong> modern heart failuremanagement, <strong>the</strong> Warfar<strong>in</strong> and Antiplatelet Therapy <strong>in</strong>Chronic Heart Failure trial (WATCH) was term<strong>in</strong>ated withoutadequate power to def<strong>in</strong>e <strong>the</strong> effect <strong>of</strong> warfar<strong>in</strong> comparedwith aspir<strong>in</strong> or clopidogrel on stroke. 253Similarly, no adequately powered randomized studies <strong>of</strong>aspir<strong>in</strong> or o<strong>the</strong>r platelet <strong>in</strong>hibitor drugs have been carried out <strong>in</strong>patients with chronic heart failure. An ongo<strong>in</strong>g trial, Warfar<strong>in</strong>versus Aspir<strong>in</strong> <strong>in</strong> Reduced Cardiac Ejection Fraction(WARCEF), is designed to compare <strong>the</strong> efficacy <strong>of</strong> warfar<strong>in</strong>(INR 2.5 to 3.0) and aspir<strong>in</strong> (325 mg daily) with regard to <strong>the</strong>composite end po<strong>in</strong>t <strong>of</strong> death or stroke (ischemic or hemor-Downloaded from stroke.ahajournals.org by on March 8, 2011
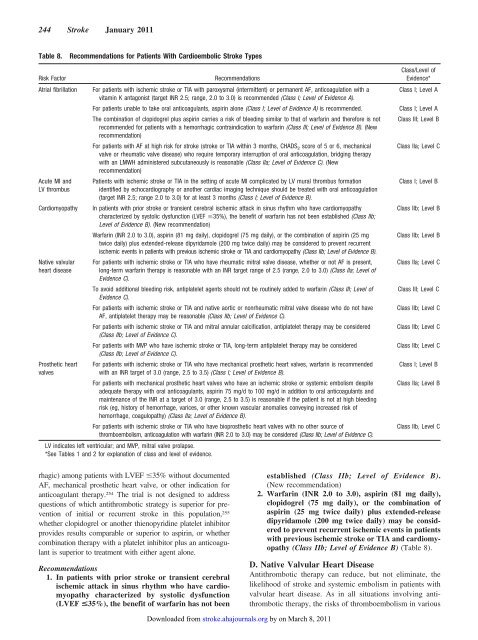
244 <strong>Stroke</strong> January 2011Table 8.Recommendations <strong>for</strong> Patients With Cardioembolic <strong>Stroke</strong> TypesRisk FactorAtrial fibrillationAcute MI andLV thrombusCardiomyopathyNative valvularheart diseasePros<strong>the</strong>tic heartvalvesRecommendationsFor patients with ischemic stroke or TIA with paroxysmal (<strong>in</strong>termittent) or permanent AF, anticoagulation with avitam<strong>in</strong> K antagonist (target INR 2.5; range, 2.0 to 3.0) is recommended (Class I; Level <strong>of</strong> Evidence A).For patients unable to take oral anticoagulants, aspir<strong>in</strong> alone (Class I; Level <strong>of</strong> Evidence A) is recommended.The comb<strong>in</strong>ation <strong>of</strong> clopidogrel plus aspir<strong>in</strong> carries a risk <strong>of</strong> bleed<strong>in</strong>g similar to that <strong>of</strong> warfar<strong>in</strong> and <strong>the</strong>re<strong>for</strong>e is notrecommended <strong>for</strong> patients with a hemorrhagic contra<strong>in</strong>dication to warfar<strong>in</strong> (Class III; Level <strong>of</strong> Evidence B). (Newrecommendation)For patients with AF at high risk <strong>for</strong> stroke (stroke or TIA with<strong>in</strong> 3 months, CHADS 2 score <strong>of</strong> 5 or 6, mechanicalvalve or rheumatic valve disease) who require temporary <strong>in</strong>terruption <strong>of</strong> oral anticoagulation, bridg<strong>in</strong>g <strong>the</strong>rapywith an LMWH adm<strong>in</strong>istered subcutaneously is reasonable (Class IIa; Level <strong>of</strong> Evidence C). (Newrecommendation)Patients with ischemic stroke or TIA <strong>in</strong> <strong>the</strong> sett<strong>in</strong>g <strong>of</strong> acute MI complicated by LV mural thrombus <strong>for</strong>mationidentified by echocardiography or ano<strong>the</strong>r cardiac imag<strong>in</strong>g technique should be treated with oral anticoagulation(target INR 2.5; range 2.0 to 3.0) <strong>for</strong> at least 3 months (Class I; Level <strong>of</strong> Evidence B).In patients with prior stroke or transient cerebral ischemic attack <strong>in</strong> s<strong>in</strong>us rhythm who have cardiomyopathycharacterized by systolic dysfunction (LVEF 35%), <strong>the</strong> benefit <strong>of</strong> warfar<strong>in</strong> has not been established (Class IIb;Level <strong>of</strong> Evidence B). (New recommendation)Warfar<strong>in</strong> (INR 2.0 to 3.0), aspir<strong>in</strong> (81 mg daily), clopidogrel (75 mg daily), or <strong>the</strong> comb<strong>in</strong>ation <strong>of</strong> aspir<strong>in</strong> (25 mgtwice daily) plus extended-release dipyridamole (200 mg twice daily) may be considered to prevent recurrentischemic events <strong>in</strong> patients with previous ischemic stroke or TIA and cardiomyopathy (Class IIb; Level <strong>of</strong> Evidence B).For patients with ischemic stroke or TIA who have rheumatic mitral valve disease, whe<strong>the</strong>r or not AF is present,long-term warfar<strong>in</strong> <strong>the</strong>rapy is reasonable with an INR target range <strong>of</strong> 2.5 (range, 2.0 to 3.0) (Class IIa; Level <strong>of</strong>Evidence C).To avoid additional bleed<strong>in</strong>g risk, antiplatelet agents should not be rout<strong>in</strong>ely added to warfar<strong>in</strong> (Class III; Level <strong>of</strong>Evidence C).For patients with ischemic stroke or TIA and native aortic or nonrheumatic mitral valve disease who do not haveAF, antiplatelet <strong>the</strong>rapy may be reasonable (Class IIb; Level <strong>of</strong> Evidence C).For patients with ischemic stroke or TIA and mitral annular calcification, antiplatelet <strong>the</strong>rapy may be considered(Class IIb; Level <strong>of</strong> Evidence C).For patients with MVP who have ischemic stroke or TIA, long-term antiplatelet <strong>the</strong>rapy may be considered(Class IIb; Level <strong>of</strong> Evidence C).For patients with ischemic stroke or TIA who have mechanical pros<strong>the</strong>tic heart valves, warfar<strong>in</strong> is recommendedwith an INR target <strong>of</strong> 3.0 (range, 2.5 to 3.5) (Class I; Level <strong>of</strong> Evidence B).For patients with mechanical pros<strong>the</strong>tic heart valves who have an ischemic stroke or systemic embolism despiteadequate <strong>the</strong>rapy with oral anticoagulants, aspir<strong>in</strong> 75 mg/d to 100 mg/d <strong>in</strong> addition to oral anticoagulants andma<strong>in</strong>tenance <strong>of</strong> <strong>the</strong> INR at a target <strong>of</strong> 3.0 (range, 2.5 to 3.5) is reasonable if <strong>the</strong> patient is not at high bleed<strong>in</strong>grisk (eg, history <strong>of</strong> hemorrhage, varices, or o<strong>the</strong>r known vascular anomalies convey<strong>in</strong>g <strong>in</strong>creased risk <strong>of</strong>hemorrhage, coagulopathy) (Class IIa; Level <strong>of</strong> Evidence B).For patients with ischemic stroke or TIA who have biopros<strong>the</strong>tic heart valves with no o<strong>the</strong>r source <strong>of</strong>thromboembolism, anticoagulation with warfar<strong>in</strong> (INR 2.0 to 3.0) may be considered (Class IIb; Level <strong>of</strong> Evidence C).LV <strong>in</strong>dicates left ventricular; and MVP, mitral valve prolapse.*See Tables 1 and 2 <strong>for</strong> explanation <strong>of</strong> class and level <strong>of</strong> evidence.Class/Level <strong>of</strong>Evidence*Class I; Level AClass I; Level AClass III; Level BClass IIa; Level CClass I; Level BClass IIb; Level BClass IIb; Level BClass IIa; Level CClass III; Level CClass IIb; Level CClass IIb; Level CClass IIb; Level CClass I; Level BClass IIa; Level BClass IIb, Level Crhagic) among patients with LVEF 35% without documentedAF, mechanical pros<strong>the</strong>tic heart valve, or o<strong>the</strong>r <strong>in</strong>dication <strong>for</strong>anticoagulant <strong>the</strong>rapy. 254 The trial is not designed to addressquestions <strong>of</strong> which antithrombotic strategy is superior <strong>for</strong> prevention<strong>of</strong> <strong>in</strong>itial or recurrent stroke <strong>in</strong> this population, 255whe<strong>the</strong>r clopidogrel or ano<strong>the</strong>r thienopyrid<strong>in</strong>e platelet <strong>in</strong>hibitorprovides results comparable or superior to aspir<strong>in</strong>, or whe<strong>the</strong>rcomb<strong>in</strong>ation <strong>the</strong>rapy with a platelet <strong>in</strong>hibitor plus an anticoagulantis superior to treatment with ei<strong>the</strong>r agent alone.Recommendations1. In patients with prior stroke or transient cerebralischemic attack <strong>in</strong> s<strong>in</strong>us rhythm who have cardiomyopathycharacterized by systolic dysfunction(LVEF