AHA/ASA Guideline Guidelines for the Prevention of Stroke in ...
AHA/ASA Guideline Guidelines for the Prevention of Stroke in ...
AHA/ASA Guideline Guidelines for the Prevention of Stroke in ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
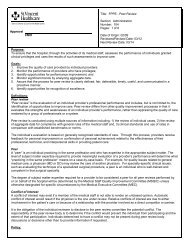
234 <strong>Stroke</strong> January 2011Table 4.Recommendations <strong>for</strong> Modifiable Behavioral Risk FactorsRisk FactorCigarette smok<strong>in</strong>gAlcohol consumptionRecommendationsHealthcare providers should strongly advise every patient with stroke or TIA who has smoked <strong>in</strong> <strong>the</strong> pastyear to quit (Class I; Level <strong>of</strong> Evidence C).It is reasonable to avoid environmental (passive) tobacco smoke (Class IIa; Level <strong>of</strong> Evidence C).Counsel<strong>in</strong>g, nicot<strong>in</strong>e products, and oral smok<strong>in</strong>g cessation medications are effective <strong>for</strong> help<strong>in</strong>g smokers toquit (Class I; Level <strong>of</strong> Evidence A).Patients with ischemic stroke or TIA who are heavy dr<strong>in</strong>kers should elim<strong>in</strong>ate or reduce <strong>the</strong>ir consumption <strong>of</strong>alcohol (Class I; Level <strong>of</strong> Evidence C).Light to moderate levels <strong>of</strong> alcohol consumption (no more than 2 dr<strong>in</strong>ks per day <strong>for</strong> men and 1 dr<strong>in</strong>k per day<strong>for</strong> nonpregnant women) may be reasonable; nondr<strong>in</strong>kers should not be counseled to start dr<strong>in</strong>k<strong>in</strong>g (ClassIIb; Level <strong>of</strong> Evidence B).Physical activity For patients with ischemic stroke or TIA who are capable <strong>of</strong> engag<strong>in</strong>g <strong>in</strong> physical activity, at least 30m<strong>in</strong>utes <strong>of</strong> moderate-<strong>in</strong>tensity physical exercise, typically def<strong>in</strong>ed as vigorous activity sufficient to break asweat or noticeably raise heart rate, 1 to 3 times a week (eg, walk<strong>in</strong>g briskly, us<strong>in</strong>g an exercise bicycle)may be considered to reduce risk factors and comorbid conditions that <strong>in</strong>crease <strong>the</strong> likelihood <strong>of</strong> recurrentstroke (Class IIb; Level <strong>of</strong> Evidence C).For those <strong>in</strong>dividuals with a disability follow<strong>in</strong>g ischemic stroke, supervision by a healthcare pr<strong>of</strong>essional,such as a physical <strong>the</strong>rapist or cardiac rehabilitation pr<strong>of</strong>essional, at least on <strong>in</strong>itiation <strong>of</strong> an exerciseregimen, may be considered (Class IIb; Level <strong>of</strong> Evidence C).Metabolic syndrome At this time, <strong>the</strong> utility <strong>of</strong> screen<strong>in</strong>g patients <strong>for</strong> <strong>the</strong> metabolic syndrome after stroke has not beenestablished (Class IIb; Level <strong>of</strong> Evidence C). (New recommendation)For patients who are screened and classified as hav<strong>in</strong>g <strong>the</strong> metabolic syndrome, management should <strong>in</strong>cludecounsel<strong>in</strong>g <strong>for</strong> lifestyle modification (diet, exercise, and weight loss) <strong>for</strong> vascular risk reduction (Class I;Level <strong>of</strong> Evidence C). (New recommendation)Preventive care <strong>for</strong> patients with <strong>the</strong> metabolic syndrome should <strong>in</strong>clude appropriate treatment <strong>for</strong> <strong>in</strong>dividualcomponents <strong>of</strong> <strong>the</strong> syndrome that are also stroke risk factors, particularly dyslipidemia and hypertension(Class I; Level <strong>of</strong> Evidence A). (New recommendation)*See Tables 1 and 2 <strong>for</strong> explanation <strong>of</strong> class and level <strong>of</strong> evidence.Class/Level <strong>of</strong>Evidence*Class I; Level CClass IIa; Level CClass I; Level AClass I; Level CClass IIb; Level BClass IIb; Level CClass IIb; Level CClass IIb; Level CClass I; Level CClass I; Level ARecommendations1. Healthcare providers should strongly advise everypatient with stroke or TIA who has smoked <strong>in</strong> <strong>the</strong>past year to quit (Class I; Level <strong>of</strong> Evidence C).2. It is reasonable to avoid environmental (passive)tobacco smoke (Class IIa; Level <strong>of</strong> Evidence C).3. Counsel<strong>in</strong>g, nicot<strong>in</strong>e products, and oral smok<strong>in</strong>gcessation medications are effective <strong>for</strong> help<strong>in</strong>g smokersquit (Class I; Level <strong>of</strong> Evidence A) (Table 4).E. Alcohol ConsumptionThere is strong evidence that chronic alcoholism and heavydr<strong>in</strong>k<strong>in</strong>g are risk factors <strong>for</strong> all stroke subtypes. 82–86 Studieshave demonstrated an association between alcohol and ischemicstroke, rang<strong>in</strong>g from a def<strong>in</strong>ite <strong>in</strong>dependent effect to noeffect. Most studies have suggested a J-shaped associationbetween alcohol and ischemic stroke, with a protective effectfrom light or moderate consumption and an elevated risk <strong>of</strong>stroke with heavy consumption <strong>of</strong> alcohol. 82,83,87–96The majority <strong>of</strong> <strong>the</strong> data on <strong>the</strong> risk <strong>of</strong> alcohol are relatedto primary prevention, which is discussed extensively <strong>in</strong> <strong>the</strong><strong>AHA</strong>/<strong>ASA</strong> guidel<strong>in</strong>e statement on primary prevention <strong>of</strong>ischemic stroke. 13Few studies have evaluated <strong>the</strong> association between alcoholconsumption and recurrent stroke. <strong>Stroke</strong> recurrence was significantly<strong>in</strong>creased among ischemic stroke patients with priorheavy alcohol use <strong>in</strong> <strong>the</strong> Nor<strong>the</strong>rn Manhattan cohort. 89 Nostudies have demonstrated that reduction <strong>of</strong> alcohol <strong>in</strong>takedecreases risk <strong>of</strong> recurrent stroke. The mechanism <strong>for</strong> reducedrisk <strong>of</strong> ischemic stroke with light to moderate alcohol consumptionmay be related to an <strong>in</strong>crease <strong>in</strong> HDL, 97,98 a decrease <strong>in</strong>platelet aggregation, 99,100 and a lower concentration <strong>of</strong> plasmafibr<strong>in</strong>ogen. 101,102 The mechanism <strong>of</strong> risk <strong>in</strong> heavy alcohol users<strong>in</strong>cludes alcohol-<strong>in</strong>duced hypertension, hypercoagulable state,reduced cerebral blood flow, and AF or cardioembolism due tocardiomyopathy. 83,89,103 In addition, alcohol consumption has beenassociated with <strong>in</strong>sul<strong>in</strong> resistance and <strong>the</strong> metabolic syndrome. 104It is well established that alcohol can cause dependenceand that alcoholism is a major public health problem. Whenadvis<strong>in</strong>g a patient about behaviors to reduce risk <strong>of</strong> recurrentstroke, cl<strong>in</strong>icians should consider <strong>the</strong> <strong>in</strong>terrelationship betweeno<strong>the</strong>r risk factors and alcohol consumption. Nondr<strong>in</strong>kersshould not be counseled to start dr<strong>in</strong>k<strong>in</strong>g. A primary goal<strong>for</strong> secondary stroke prevention is to elim<strong>in</strong>ate or reducealcohol consumption <strong>in</strong> heavy dr<strong>in</strong>kers through establishedscreen<strong>in</strong>g and counsel<strong>in</strong>g methods as outl<strong>in</strong>ed <strong>in</strong> <strong>the</strong> USPreventive Services Task Force Update 2004. 105Recommendations1. Patients with ischemic stroke or TIA who are heavydr<strong>in</strong>kers should elim<strong>in</strong>ate or reduce <strong>the</strong>ir consumption<strong>of</strong> alcohol (Class I; Level <strong>of</strong> Evidence C).2. Light to moderate levels <strong>of</strong> alcohol consumption (nomore than 2 dr<strong>in</strong>ks per day <strong>for</strong> men and 1 dr<strong>in</strong>k perday <strong>for</strong> women who are not pregnant) may be reasonable;nondr<strong>in</strong>kers should not be counseled to startdr<strong>in</strong>k<strong>in</strong>g (Class IIb; Level <strong>of</strong> Evidence B) (Table 4).Downloaded from stroke.ahajournals.org by on March 8, 2011