HeritageSelect Envoy $5000 Deductible - Premera Blue Cross
HeritageSelect Envoy $5000 Deductible - Premera Blue Cross
HeritageSelect Envoy $5000 Deductible - Premera Blue Cross

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
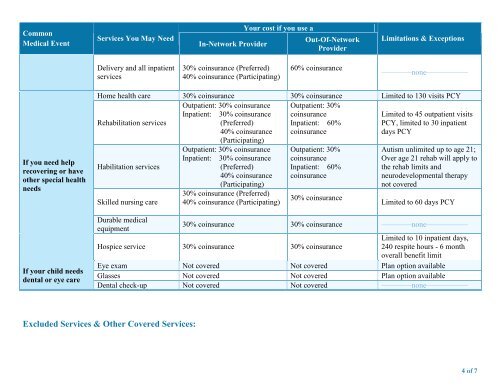
CommonMedical EventServices You May NeedIn-Network ProviderYour cost if you use aOut-Of-NetworkProviderLimitations & ExceptionsDelivery and all inpatientservices30% coinsurance (Preferred)40% coinsurance (Participating)60% coinsurance––––––––none–––––––––––If you need helprecovering or haveother special healthneedsIf your child needsdental or eye careHome health care 30% coinsurance 30% coinsurance Limited to 130 visits PCYRehabilitation servicesOutpatient: 30% coinsuranceInpatient: 30% coinsurance(Preferred)40% coinsurance(Participating)Outpatient: 30%coinsuranceInpatient: 60%coinsuranceLimited to 45 outpatient visitsPCY, limited to 30 inpatientdays PCYHabilitation servicesSkilled nursing careDurable medicalequipmentOutpatient: 30% coinsuranceInpatient: 30% coinsurance(Preferred)40% coinsurance(Participating)30% coinsurance (Preferred)40% coinsurance (Participating)Outpatient: 30%coinsuranceInpatient: 60%coinsurance30% coinsuranceAutism unlimited up to age 21;Over age 21 rehab will apply tothe rehab limits andneurodevelopmental therapynot coveredLimited to 60 days PCY30% coinsurance 30% coinsurance ––––––––none–––––––––––Hospice service 30% coinsurance 30% coinsuranceLimited to 10 inpatient days,240 respite hours - 6 monthoverall benefit limitEye exam Not covered Not covered Plan option availableGlasses Not covered Not covered Plan option availableDental check-up Not covered Not covered ––––––––none–––––––––––Excluded Services & Other Covered Services:4 of 7