PCD Strategy Evaluation 2007.pdf - NT Health Digital Library ...
PCD Strategy Evaluation 2007.pdf - NT Health Digital Library ...
PCD Strategy Evaluation 2007.pdf - NT Health Digital Library ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
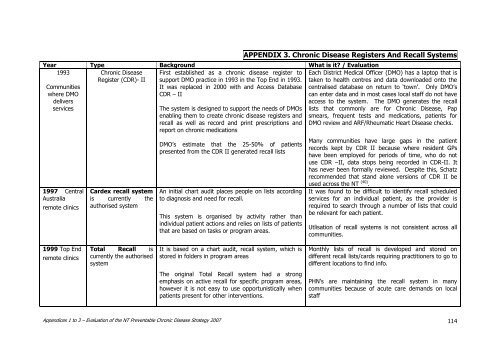
Communitieswhere DMOdeliversservicesAPPENDIX 3. Chronic Disease Registers And Recall SystemsYear Type Background What is it? / <strong>Evaluation</strong>1993Chronic DiseaseRegister (CDR)- II1997 CentralAustraliaremote clinicsCardex recall systemis currently theauthorised systemFirst established as a chronic disease register tosupport DMO practice in 1993 in the Top End in 1993.It was replaced in 2000 with and Access DatabaseCDR – IIThe system is designed to support the needs of DMOsenabling them to create chronic disease registers andrecall as well as record and print prescriptions andreport on chronic medicationsDMO‟s estimate that the 25-50% of patientspresented from the CDR II generated recall listsAn initial chart audit places people on lists accordingto diagnosis and need for recall.This system is organised by activity rather thanindividual patient actions and relies on lists of patientsthat are based on tasks or program areas.Each District Medical Officer (DMO) has a laptop that istaken to health centres and data downloaded onto thecentralised database on return to „town‟. Only DMO‟scan enter data and in most cases local staff do not haveaccess to the system. The DMO generates the recalllists that commonly are for Chronic Disease, Papsmears, frequent tests and medications, patients forDMO review and ARF/Rheumatic Heart Disease checks.Many communities have large gaps in the patientrecords kept by CDR II because where resident GPshave been employed for periods of time, who do notuse CDR –II, data stops being recorded in CDR-II. Ithas never been formally reviewed. Despite this, Schatzrecommended that stand alone versions of CDR II beused across the <strong>NT</strong> (40) .It was found to be difficult to identify recall scheduledservices for an individual patient, as the provider isrequired to search through a number of lists that couldbe relevant for each patient.Utlisation of recall systems is not consistent across allcommunities.1999 Top Endremote clinicsTotal Recall iscurrently the authorisedsystemIt is based on a chart audit, recall system, which isstored in folders in program areasMonthly lists of recall is developed and stored ondifferent recall lists/cards requiring practitioners to go todifferent locations to find info.The original Total Recall system had a strongemphasis on active recall for specific program areas,however it is not easy to use opportunistically whenpatients present for other interventions.PHN‟s are maintaining the recall system in manycommunities because of acute care demands on localstaffAppendices 1 to 3 – <strong>Evaluation</strong> of the <strong>NT</strong> Preventable Chronic Disease <strong>Strategy</strong> 2007 114