7 Orthopedics andRehabilitation <strong>Management</strong>Care <strong>of</strong> Contractures and ScoliosisPeople with all forms <strong>of</strong> <strong>CMD</strong> are commonlyfaced with orthopedic problems <strong>of</strong> the limbs,joints, and spine. Access to orthopedic care anddifferent types <strong>of</strong> rehabilitation management isimportant throughout your child’s life to preserveand optimize function; promote comfort,safety, and independent mobility; relieve pain;and maximize quality <strong>of</strong> life.Orthopedic problems may include joint andneck contractures, hypotonia, scoliosis, footdeformity, and hip dislocation or subluxation.• Conditions that may be present at birthinclude arthrogryposis, hypotonia,torticollis, hip dislocation, scoliosis,and clubfoot.• Common orthopedic problems thathappen when a child is older includedevelopment <strong>of</strong> contractures andscoliosis, which may affect your child’srespiratory health (see RespiratoryCare section).Orthopedic treatment and rehabilitationinterventions must be seen as both short-termand long-term issues; they should be viewed asan investment for the future.AssessmentYour child’s multidisciplinary team shouldinclude an orthopedist and a physicalmedication and rehabilitation team. <strong>The</strong>rehabilitation management team includesphysical and occupational therapists, orthotists,and wheelchair, seating, and equipmentspecialists.At least annually, your child should have anevaluation <strong>of</strong> his or her spine curvature, jointmobility, sitting comfort, and activities <strong>of</strong> dailyliving. Commonly used assessment tools includephysical examination, spinal X-ray, goniometry,and myometry.For younger children with severe hypotonia,respiratory insufficiency, or an unstable or rapidprogression in the curvature <strong>of</strong> the spine, or23when there is a poor response to treatmentmeasures, more frequent evaluations by his orher team will be necessary.Parents and caregivers are importantparticipants in monitoring and assisting withtheir child’s orthopedic interventions. You areencouraged to seek expert consultation regardingany orthopedic concerns.Orthopedic ComplicationsAlthough orthopedic complications can occur inall the subtypes <strong>of</strong> <strong>CMD</strong>, their severity, type, andlocation differs between the various subtypes <strong>of</strong><strong>CMD</strong> (see Table 5). Contractures are discussed inmore detail in Box 3.Box 3Contractures in <strong>CMD</strong>• A contracture is a joint that nolonger moves all the way. Most jointsin the body (like the elbow or knee)are like doors that sit on hinges andcan open and close completely. Whena contracture happens, the hingesdon’t work properly and the doorremains stuck in a half-open,half-closed position.• Having a contracture can makelife more difficult because one losesthe ability to move arms or legs,which remain “stuck” in one position.• Most contractures start gradually andget worse over time. <strong>The</strong> onlyintervention currently available forcontractures, with limited success, isstretching and low-impact exercisethat encourages full range <strong>of</strong>supported motion (for example,swimming).• Neck or jaw contractures may have asignificant impact on functionalability (movement, feeding) andrequire special considerationregarding anesthesia prior to surgery.
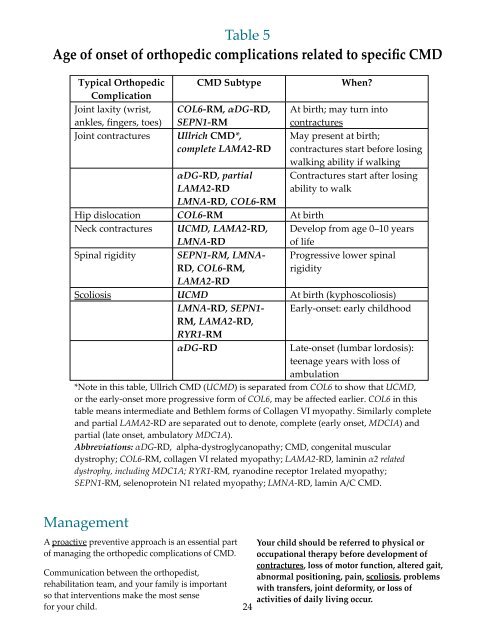
Table 5Age <strong>of</strong> onset <strong>of</strong> orthopedic complications related to specific <strong>CMD</strong>Typical OrthopedicComplicationJoint laxity (wrist,ankles, fingers, toes)Joint contractures<strong>CMD</strong> SubtypeCOL6-RM, DG-RD,SEPN1-RMUllrich <strong>CMD</strong>*,complete LAMA2-RDDG-RD, partialLAMA2-RDLMNA-RD, COL6-RMWhen?At birth; may turn intocontracturesMay present at birth;contractures start before losingwalking ability if walkingContractures start after losingability to walkHip dislocation COL6-RM At birthNeck contractures U<strong>CMD</strong>, LAMA2-RD,LMNA-RDDevelop from age 0–10 years<strong>of</strong> lifeSpinal rigidity SEPN1-RM, LMNA-RD, COL6-RM,Progressive lower spinalrigidityLAMA2-RDScoliosis U<strong>CMD</strong> At birth (kyphoscoliosis)LMNA-RD, SEPN1- Early-onset: early childhoodRM, LAMA2-RD,RYR1-RMDG-RDLate-onset (lumbar lordosis):teenage years with loss <strong>of</strong>ambulation*Note in this table, Ullrich <strong>CMD</strong> (U<strong>CMD</strong>) is separated from COL6 to show that U<strong>CMD</strong>,or the early-onset more progressive form <strong>of</strong> COL6, may be affected earlier. COL6 in thistable means intermediate and Bethlem forms <strong>of</strong> Collagen VI myopathy. Similarly completeand partial LAMA2-RD are separated out to denote, complete (early onset, MDCIA) andpartial (late onset, ambulatory MDC1A).Abbreviations: DG-RD, alpha-dystroglycanopathy; <strong>CMD</strong>, congenital musculardystrophy; COL6-RM, collagen VI related myopathy; LAMA2-RD, laminin 2 relateddystrophy, including MDC1A; RYR1-RM, ryanodine receptor 1related myopathy;SEPN1-RM, selenoprotein N1 related myopathy; LMNA-RD, lamin A/C <strong>CMD</strong>.<strong>Management</strong>A proactive preventive approach is an essential part<strong>of</strong> managing the orthopedic complications <strong>of</strong> <strong>CMD</strong>.Communication between the orthopedist,rehabilitation team, and your family is importantso that interventions make the most sensefor your child.24Your child should be referred to physical oroccupational therapy before development <strong>of</strong>contractures, loss <strong>of</strong> motor function, altered gait,abnormal positioning, pain, scoliosis, problemswith transfers, joint deformity, or loss <strong>of</strong>activities <strong>of</strong> daily living occur.45