Pelvic Disruption: Assessment and Classification
Pelvic Disruption: Assessment and Classification
Pelvic Disruption: Assessment and Classification

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
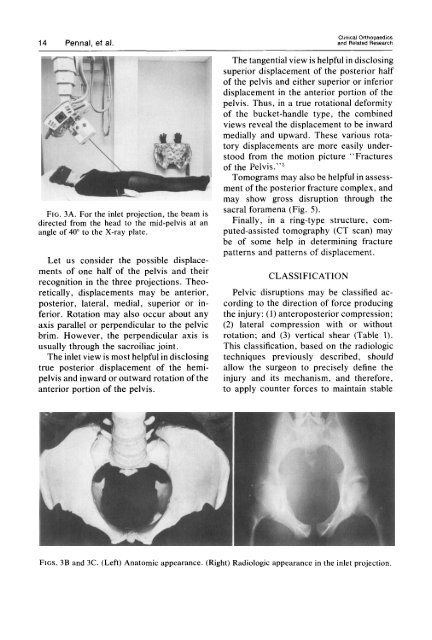
Clinical Orthopaedics14 Pennal, et al. <strong>and</strong> Related ResearchFIG. 3A. For the inlet projection, the beam isdirected from the head to the mid-pelvis at anangle of 40" to the X-ray plate.Let us consider the possible displacementsof one half of the pelvis <strong>and</strong> theirrecognition in the three projections. Theoretically,displacements may be anterior,posterior, lateral, medial, superior or inferior.Rotation may also occur about anyaxis parallel or perpendicular to the pelvicbrim. However, the perpendicular axis isusually through the sacroiliac joint.The inlet view is most helpful in disclosingtrue posterior displacement of the hemipelvis<strong>and</strong> inward or outward rotation of theanterior portion of the pelvis.The tangential view is helpful in disclosingsuperior displacement of the posterior halfof the pelvis <strong>and</strong> either superior or inferiordisplacement in the anterior portion of thepelvis. Thus, in a true rotational deformityof the bucket-h<strong>and</strong>le type, the combinedviews reveal the displacement to be inwardmedially <strong>and</strong> upward. These various rotatorydisplacements are more easily understoodfrom the motion picture "Fracturesof the Pelvis.""Tomograms may also be helpful in assessmentof the posterior fracture complex, <strong>and</strong>may show gross disruption through thesacral foramena (Fig. 5).Finally, in a ring-type structure, computed-assistedtomography (CT scan) maybe of some help in determining fracturepatterns <strong>and</strong> patterns of displacement.CLASSIFICATION<strong>Pelvic</strong> disruptions may be classified accordingto the direction of force producingthe injury: (1) anteroposterior compression;(2) lateral compression with or withoutrotation; <strong>and</strong> (3) vertical shear (Table I).This classification, based on the radiologictechniques previously described, shouldallow the surgeon to precisely define theinjury <strong>and</strong> its mechanism, <strong>and</strong> therefore,to apply counter forces to maintain stableFIGS. 3B <strong>and</strong> 3C. (Left) Anatomic appearance. (Right) Radiologic appearance in the inlet projection.