Anaesthesia Clinical Indicators Version 5.1CI 4.1CI 5.1CI 5.2CI 6.1CI 6.2for medical reasonsUnplanned patientadmission to an intensivecare unit within 24 hours<strong>of</strong> a procedure.Measurement <strong>and</strong>documentation <strong>of</strong> painintensity scores aftermajor surgery.At least daily review by ananaesthetist <strong>of</strong> patientsreceiving postoperativeepidural analgesia, untilremoval <strong>of</strong> catheter.Minimisation <strong>of</strong> post-duralpuncture headache.Commencement <strong>of</strong>surgery within 30 minutes<strong>of</strong> a request foremergency Caesareanwww.ncepod.org.au/pdf/2002/02sum.pdf2. Vimlati L, Gilsanz F, Goldik Z. Quality <strong>and</strong> safetyguidelines <strong>of</strong> postanaesthesia care: Working Party onPost Anaesthesia Care. Eur J Anaesthesiol 2009 Apr22.1. Haller G, Myles PS, Wolfe R, Weeks AM, StoelwinderJ, McNeil J. Validity <strong>of</strong> uplanned admission to anintensive care unit as a measure <strong>of</strong> patient safety insurgical patients. Anesthesiology 2005; 103:1121-1129.2. Haller G, Stoelwinder J, Myles PS, McNeil J. Quality<strong>and</strong> safety <strong>indicators</strong> in anesthesia: a systematicreview. Anesthesiology 2009; 110:1058-75.1. NHMRC. Acute pain management: scientificevidence, 2 nd ed. 20052. Acute postoperative pain (APOP) project.http://www.health.vic.gov.au/qualitycouncil/downloads/acute/apop_project.pdf.3. Gould TH, Crosby DL, Harmer M, et al. Policy forcontrolling pain after surgery: effect <strong>of</strong> sequentialchanges in management. BMJ 2005; 305:1187-93.4. JCAHO & NPC. Pain: current underst<strong>and</strong>ing <strong>of</strong>assessment, management <strong>and</strong> treatments. JointCommission on Accreditation <strong>of</strong> HealthcareOrganisations <strong>and</strong> the National PharmaceuticalCouncil, Inc.www.jcaho.org/news+room/health+care+issues/pm+monographs.htm1. Policy Document PS3: Guidelines for theManagement <strong>of</strong> Major Regional Analgesia. <strong>Australian</strong><strong>and</strong> <strong>New</strong> Zeal<strong>and</strong> <strong>College</strong> <strong>of</strong> Anaesthetists.www.anzca.edu.au/resources/pr<strong>of</strong>essionaldocuments2. Horlocker TT, Wedel DJ, Benzon H, et al. Regionalanesthesia in the anticoagulated patient: defining therisks (the second ASRA Consensus Conference onNeuraxial Anesthesia <strong>and</strong> Anticoagulation). RegAnesth Pain Med 2003;28(3):172-97.3. Tryba M. European practice guidelines:thromboembolism prophylaxis <strong>and</strong> regionalanesthesia. Reg Anesth Pain Med 1998;23(6 Suppl2):178-82.1. Choi PT, Galinski SE, Takeuchi L, et al. PDPH is acommon complication <strong>of</strong> neuraxial blockade inparturients: a meta-analysis <strong>of</strong> obstetrical studies.Can J Anaesth 2003; 50(5):460-9.2. Halpern S, Preston R. Postdural puncture headache<strong>and</strong> spinal needle design. Meta-analyses.Anesthesiology 1994; 81(6):1376-83.1. American <strong>College</strong> <strong>of</strong> Obstetricians <strong>and</strong> Gynecologists.Optimal goals for anesthesia care in obstetrics.ACOG Committee Opinion #256. Washington, DC:American <strong>College</strong> <strong>of</strong> Obstetricians <strong>and</strong> Gynecologists,ACHS Clinical Indicator User Manual 2011 27
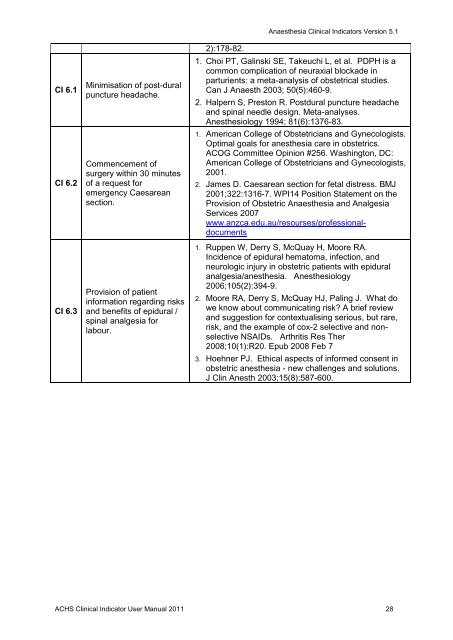
CI 6.1CI 6.2CI 6.3Minimisation <strong>of</strong> post-duralpuncture headache.Commencement <strong>of</strong>surgery within 30 minutes<strong>of</strong> a request foremergency Caesareansection.Provision <strong>of</strong> patientinformation regarding risks<strong>and</strong> benefits <strong>of</strong> epidural /spinal analgesia forlabour.2):178-82.Anaesthesia Clinical Indicators Version 5.11. Choi PT, Galinski SE, Takeuchi L, et al. PDPH is acommon complication <strong>of</strong> neuraxial blockade inparturients: a meta-analysis <strong>of</strong> obstetrical studies.Can J Anaesth 2003; 50(5):460-9.2. Halpern S, Preston R. Postdural puncture headache<strong>and</strong> spinal needle design. Meta-analyses.Anesthesiology 1994; 81(6):1376-83.1. American <strong>College</strong> <strong>of</strong> Obstetricians <strong>and</strong> Gynecologists.Optimal goals for anesthesia care in obstetrics.ACOG Committee Opinion #256. Washington, DC:American <strong>College</strong> <strong>of</strong> Obstetricians <strong>and</strong> Gynecologists,2001.2. James D. Caesarean section for fetal distress. BMJ2001;322:1316-7. WPI14 Position Statement on theProvision <strong>of</strong> Obstetric Anaesthesia <strong>and</strong> AnalgesiaServices 2007www.anzca.edu.au/resourses/pr<strong>of</strong>essionaldocuments1. Ruppen W, Derry S, McQuay H, Moore RA.Incidence <strong>of</strong> epidural hematoma, infection, <strong>and</strong>neurologic injury in obstetric patients with epiduralanalgesia/anesthesia. Anesthesiology2006;105(2):394-9.2. Moore RA, Derry S, McQuay HJ, Paling J. What dowe know about communicating risk? A brief review<strong>and</strong> suggestion for contextualising serious, but rare,risk, <strong>and</strong> the example <strong>of</strong> cox-2 selective <strong>and</strong> nonselectiveNSAIDs. Arthritis Res Ther2008;10(1):R20. Epub 2008 Feb 73. Hoehner PJ. Ethical aspects <strong>of</strong> informed consent inobstetric anesthesia - new challenges <strong>and</strong> solutions.J Clin Anesth 2003;15(8):587-600.ACHS Clinical Indicator User Manual 2011 28