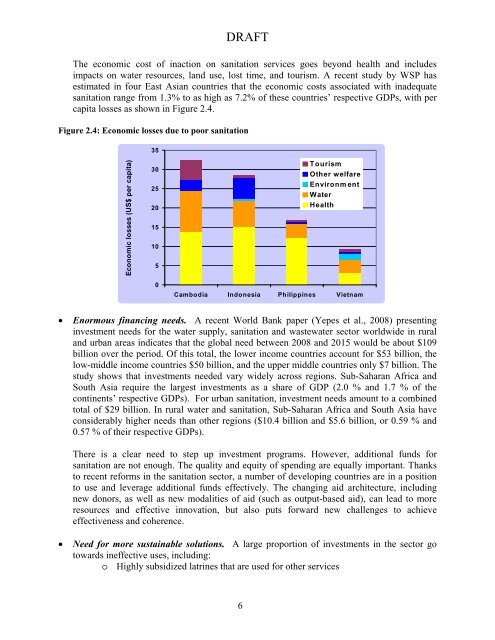
DRAFT<strong>The</strong> economic cost of inaction on sanit<strong>at</strong>ion services goes beyond health <strong>and</strong> includesimpacts on w<strong>at</strong>er resources, l<strong>and</strong> use, lost time, <strong>and</strong> tourism. A recent study by WSP hasestim<strong>at</strong>ed in four East Asian countries th<strong>at</strong> the economic costs associ<strong>at</strong>ed with inadequ<strong>at</strong>esanit<strong>at</strong>ion range from 1.3% to as high as 7.2% of these countries’ respective GDPs, with percapita losses as shown in Figure 2.4.Figure 2.4: Economic losses due to poor sanit<strong>at</strong>ion35Economic losses (US$ per capita)302520151050TourismOther welfareEnvironment<strong>W<strong>at</strong>er</strong><strong>Health</strong>Cambodia Indonesia Philippines Vietnam• Enormous financing needs. A recent World Bank paper (Yepes et al., 2008) presentinginvestment needs for the w<strong>at</strong>er supply, sanit<strong>at</strong>ion <strong>and</strong> wastew<strong>at</strong>er sector worldwide in rural<strong>and</strong> urban areas indic<strong>at</strong>es th<strong>at</strong> the global need between 2008 <strong>and</strong> 2015 would be about $109billion over the period. Of this total, the lower income countries account for $53 billion, thelow-middle income countries $50 billion, <strong>and</strong> the upper middle countries only $7 billion. <strong>The</strong>study shows th<strong>at</strong> investments needed vary widely across regions. Sub-Saharan Africa <strong>and</strong>South Asia require the largest investments as a share of GDP (2.0 % <strong>and</strong> 1.7 % of thecontinents’ respective GDPs). For urban sanit<strong>at</strong>ion, investment needs amount to a combinedtotal of $29 billion. In rural w<strong>at</strong>er <strong>and</strong> sanit<strong>at</strong>ion, Sub-Saharan Africa <strong>and</strong> South Asia haveconsiderably higher needs than other regions ($10.4 billion <strong>and</strong> $5.6 billion, or 0.59 % <strong>and</strong>0.57 % of their respective GDPs).<strong>The</strong>re is a clear need to step up investment programs. However, additional funds forsanit<strong>at</strong>ion are not enough. <strong>The</strong> quality <strong>and</strong> equity of spending are equally important. Thanksto recent reforms in the sanit<strong>at</strong>ion sector, a number of developing countries are in a positionto use <strong>and</strong> leverage additional funds effectively. <strong>The</strong> changing aid architecture, includingnew donors, as well as new modalities of aid (such as output-based aid), can lead to moreresources <strong>and</strong> effective innov<strong>at</strong>ion, but also puts forward new challenges to achieveeffectiveness <strong>and</strong> coherence.• Need for more sustainable solutions. A large proportion of investments in the sector gotowards ineffective uses, including:o Highly subsidized l<strong>at</strong>rines th<strong>at</strong> are used for other services6
DRAFTo Ineffective solutions purchased by households who do not have access to a broadrange of optionso Extension of sewerage networks without the commensur<strong>at</strong>e r<strong>at</strong>es of connectionsfrom householdso Wastew<strong>at</strong>er tre<strong>at</strong>ment plants th<strong>at</strong> are not oper<strong>at</strong>ed, or even when oper<strong>at</strong>ed, do noteffectively benefit the environment due to the existence of other pollution sourcesof gre<strong>at</strong>er importance.Rapidly changing new technologies bring new opportunities to change the developmentparadigm <strong>and</strong> to provide new responses to development challenges. <strong>The</strong> sanit<strong>at</strong>ion sectorhas unfortun<strong>at</strong>ely not seen the same impressive technological development of othersectors (such as the expansion of mobile phone technology <strong>and</strong> internet access).However, it will be critical to bring in new membrane technologies, innov<strong>at</strong>ive paradigmsfor non-w<strong>at</strong>er based sanit<strong>at</strong>ion systems, decentralized tre<strong>at</strong>ment (particularly for therapidly exp<strong>and</strong>ing peri-urban areas of large cities), new bio-tre<strong>at</strong>ment for small towns,<strong>and</strong> radically different approaches to reduce sludge gener<strong>at</strong>ion from basic solutions,among many others.3. Experiences of WSP in <strong>Sanit<strong>at</strong>ion</strong>3.1 Evolution of Areas of Focus in <strong>Sanit<strong>at</strong>ion</strong>Since its establishment 30 years ago, WSP has gone through three phases of support of thesanit<strong>at</strong>ion sector. <strong>The</strong> 1980s were characterized by an emphasis on engineering technologies,with specific focus on low-cost technologies, including the Ventil<strong>at</strong>ed Improved Pit (VIP),SanPl<strong>at</strong> (plastic l<strong>at</strong>rine slabs), <strong>and</strong> pour flush l<strong>at</strong>rines, among others. <strong>The</strong> hypothesis <strong>at</strong> the timewas th<strong>at</strong> upgrades in technological innov<strong>at</strong>ion <strong>and</strong> their dissemin<strong>at</strong>ion in developing countries —through a top-down <strong>and</strong> heavily subsidized infrastructure approach — was the key trigger torapidly exp<strong>and</strong> access to sanit<strong>at</strong>ion.In the 1990s, WSP changed its focus to more str<strong>at</strong>egic approaches <strong>and</strong> gre<strong>at</strong>er involvement in thefocus to bottom-up <strong>and</strong> community-driven options. Some of the tools used during th<strong>at</strong> decadeincluded Str<strong>at</strong>egic <strong>Sanit<strong>at</strong>ion</strong> Planning, a strong emphasis on condominium systems, <strong>and</strong> thedevelopment, testing <strong>and</strong> replic<strong>at</strong>ion of the Particip<strong>at</strong>ory Hygiene <strong>and</strong> <strong>Sanit<strong>at</strong>ion</strong> Transform<strong>at</strong>ion(PHAST). This decade also saw a clear emphasis on integr<strong>at</strong>ed solutions th<strong>at</strong> included w<strong>at</strong>ersupply <strong>and</strong> sanit<strong>at</strong>ion, r<strong>at</strong>her than the traditional focus on w<strong>at</strong>er supply first (assuming sanit<strong>at</strong>ionwould follow l<strong>at</strong>er on which rarely happened). During th<strong>at</strong> decade, about five technologiescontinued to be considered acceptable <strong>and</strong> there was an inherent, if not explicit, requirement ofminimum technical st<strong>and</strong>ards for sanit<strong>at</strong>ion. <strong>The</strong> st<strong>at</strong>e was seen as the main provider of sanit<strong>at</strong>ioninfrastructure <strong>and</strong> subsidies, with NGOs being promoters of sanit<strong>at</strong>ion <strong>and</strong> hygiene, generally <strong>at</strong>the household level <strong>and</strong> through labor-intensive PHAST approaches. At th<strong>at</strong> time, sanit<strong>at</strong>ion wasnot in the original list of MDG targets.Over the last five years, the importance given to sanit<strong>at</strong>ion development in WSP’s projects hasbeen steadily increasing, reaching 46% of its annual budget in 2008 (Figure 3.1). For the firsttime, the proportion of the WSP’s budget dedic<strong>at</strong>ed to sanit<strong>at</strong>ion is larger than the one dedic<strong>at</strong>edto w<strong>at</strong>er supply (33%).7