Medication Administration Daily Log (To be ... - School District 68
Medication Administration Daily Log (To be ... - School District 68
Medication Administration Daily Log (To be ... - School District 68

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
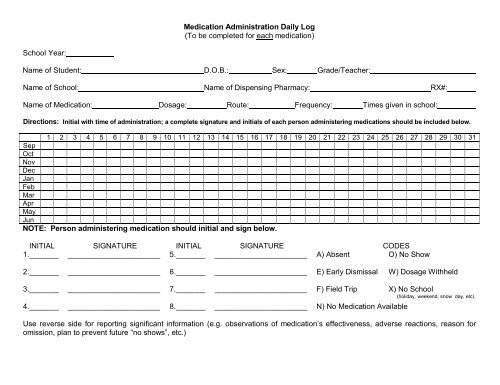
<strong>Medication</strong> <strong>Administration</strong> <strong>Daily</strong> <strong>Log</strong>(<strong>To</strong> <strong>be</strong> completed for each medication)<strong>School</strong> Year:Name of Student: D.O.B.: Sex: Grade/Teacher:Name of <strong>School</strong>: Name of Dispensing Pharmacy: RX#:Name of <strong>Medication</strong>: Dosage: Route: Frequency: Times given in school:Directions: Initial with time of administration; a complete signature and initials of each person administering medications should <strong>be</strong> included <strong>be</strong>low.1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31SepOctNovDecJanFebMarAprMayJunNOTE: Person administering medication should initial and sign <strong>be</strong>low.INITIAL SIGNATURE INITIAL SIGNATURE CODES1._______ ______________________ 5._______ ______________________ A) Absent O) No Show2._______ ______________________ 6._______ ______________________ E) Early Dismissal W) Dosage Withheld3._______ ______________________ 7._______ ______________________ F) Field Trip X) No <strong>School</strong>4._______ ______________________ 8._______ ______________________ N) No <strong>Medication</strong> Available(holiday, weekend, snow day, etc).Use reverse side for reporting significant information (e.g. observations of medication’s effectiveness, adverse reactions, reason for omission, plan to prevent future “no shows”, etc.)
Date Explanation (with signature) Date Explanation (with signature)
<strong>School</strong> Name: _________________________________________________________MEDICATION ADMINISTRATION LOG<strong>School</strong> Year: Name of Student: D.O.B.:_____Sex: Grade/Teacher: _________________________________Name of Dispensing Pharmacy:RX#: _________________Name of <strong>Medication</strong>: _________________ Dosage: Route:Frequency: ____________ Times given in school: ____________________________Directions: Sign with time of administration; a complete signature of each person administering medications must <strong>be</strong> included <strong>be</strong>low.DATE & TIMEMEDICATION/DOSESPECIALINSTRUCTIONS SIGNATURE COMMENTSThis form is part of the permanent record for students receiving medication during school hours. Fill in the above areas with the date and time the medication is given and the signature of the person administering the medication.
Directions: Sign with time of administration; a complete signature of each person administering medications must <strong>be</strong> included <strong>be</strong>low.DATE & TIMEMEDICATION/DOSESPECIALINSTRUCTIONS SIGNATURE COMMENTS