TNO Finger Pressure Reference Guide - Integral Process
TNO Finger Pressure Reference Guide - Integral Process
TNO Finger Pressure Reference Guide - Integral Process

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong><strong>Reference</strong> <strong>Guide</strong><strong>Guide</strong> for the non-invasive continuous finger bloodpressure measurement and recording systemsPortapres and FinometerTPD Biomedical InstrumentationAmsterdam, The Netherlands © 2001 <strong>TNO</strong>, 04/01-01
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong> <strong>Reference</strong> <strong>Guide</strong> 2<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong><strong>Reference</strong> <strong>Guide</strong><strong>Guide</strong> for the non-invasive continuous finger blood pressuremeasurement and recording systemsPortapres and Finometer© 04/2001 <strong>TNO</strong><strong>TNO</strong> TPD Biomedical InstrumentationAmsterdam, The Netherlands0344
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong> <strong>Reference</strong> <strong>Guide</strong> 3Copyright & Trademarks© 2001 <strong>TNO</strong> TPD Biomedical Instrumentation. All rights reserved.This document is for information purposes only.Warranty, disclaimer of warranties and limitations<strong>TNO</strong> MAKES NO WARRANTY OR REPRESENTATION, EITHER EXPRESSOR IMPLIED, WITH RESPECT TO THE PORTAPRES AND FINOMETERDEVICES, ITS QUALITY, MERCHANTABILITY, OR FITNESS FOR APARTICULAR PURPOSE. THE EQUIPMENT IS PROVIDED AS IS, NOORAL OR WRITTEN INFORMATION OR ADVICE GIVEN BY EITHERPARTY OR ITS EMPLOYEES SHALL CREATE A WARRANTY OR MAKEANY MODIFICATION, EXTENSION OR ADDITION TO THE WARRANTY<strong>TNO</strong> SHALL NOT BE LIABLE FOR ANY DIRECT, INDIRECT, INCIDENTALOR CONSEQUENTIAL DAMAGES, INCLUDING LOST PROFITS ANDDAMAGES FOR PERSONAL INJURY OR PROPERTY DAMAGE, ARISINGFROM OR IN CONNECTION WITH THE LICENSED RIGHTS OR ITS USEWHATSOEVER.IN NO CASE SHALL <strong>TNO</strong> TPD BIOMEDICAL INSTRUMENTATION’SLIABILITY EXCEED THE PURCHASE PRICE FOR THE DEVICE.Information in this document is subject to change without notice and does notrepresent a commitment on the part of <strong>TNO</strong> TPD Biomedical Instrumentation.The BeatScope software is furnished under a license agreement. The software maybe used only in accordance with that agreement.Portapres, Modelflow, Finometer and BeatScope are trademarks of <strong>TNO</strong> TPDBiomedical Instrumentation. Finapres is a registered trademark of OhmedaMonitoring Systems.No part of this publication may be reproduced, transmitted, transcribed, stored in aretrieval system, or translated into any language in any form by any means, for anypurpose other than the purchaser's personal use, without the prior writtenpermission of <strong>TNO</strong> TPD Biomedical Instrumentation
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong> <strong>Reference</strong> <strong>Guide</strong> 4WarningThe data produced by Portapres and Finometer or the accompanyingsoftware is intended as an adjunct in patient assessment and should not beused as the sole means for determining a patient’s diagnosis.
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong> <strong>Reference</strong> <strong>Guide</strong> 5Table of Contents1 Introduction .........................................................................71.1 This reference guide ................................................................................71.2 Related Publications ................................................................................71.3 Finapres ...................................................................................................81.4 Portapres..................................................................................................81.5 Finometer.................................................................................................81.6 Contacting <strong>TNO</strong>-Biomedical Instrumentation.........................................92 Measurement principle .....................................................102.1 Introduction ...........................................................................................102.2 <strong>Finger</strong> cuff .............................................................................................102.3 Plethysmograph .....................................................................................112.4 The pressure-diameter relationship........................................................122.5 Volume-clamp method ..........................................................................132.6 Physiocal algorithm ...............................................................................152.7 Example of a normal Physiocal .............................................................162.8 Example of a multi-step Physiocal ........................................................172.9 Example of a Physiocal with variable pressure levels ...........................182.10 <strong>Pressure</strong> staircase at the start of a measurement ....................................182.11 Physiocal frequency...............................................................................192.12 Note on blue fingertips ..........................................................................203 Measurement accuracy.....................................................223.1 Comparison with intra-arterial blood pressure.......................................223.1.1 <strong>Finger</strong> arterial pressure ..................................................................223.2 Brachial arterial pressure.......................................................................233.2.1 Pulse wave distortion.....................................................................243.2.2 <strong>Pressure</strong> gradient ...........................................................................263.3 Bias and precision .................................................................................263.4 Clinical use ............................................................................................263.5 Waveform filtering and level correction methods .................................273.5.1 Wave distortion correction ............................................................273.5.2 <strong>Pressure</strong> gradient correction ..........................................................283.5.3 Combination of waveform filtering and level correction...............283.6 BeatScope software program.................................................................294 Practical guidelines...........................................................314.1 Selecting the proper hand ......................................................................314.2 Selecting the proper cuff........................................................................314.3 Wrapping the cuff correctly...................................................................324.4 Selecting a finger switching interval......................................................34
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong> <strong>Reference</strong> <strong>Guide</strong> 64.5 Two finger agreement in a finger switching measurement ....................354.6 Applying hydrostatic height correction..................................................354.7 Improving and checking experimental conditions .................................374.7.1 Patient instructions ........................................................................374.7.2 Diagnostic display .........................................................................384.7.3 Checking measurement stability ....................................................394.7.4 Vaso-constriction...........................................................................41
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong> <strong>Reference</strong> <strong>Guide</strong> 71 Introduction1.1 This reference guideWith Portapres and Finometer continuous beat-to-beat finger blood pressure ismeasured. Although it is relatively easy to perform measurements, a basicunderstanding of the principle of the device is recommended to obtain reliablemeasurements. This reference guide addresses the volume-clamp method that isused to measure finger blood pressure in chapter 2. <strong>Finger</strong> blood pressure readingsare compared with intra-arterial measurements in the brachial artery in chapter 3.<strong>Guide</strong>lines to check and to improve the quality of finger blood pressuremeasurements are discussed in chapter 4.This reference guide contains an Appendix with finger blood pressure literaturereferences.Although Portapres and Finometer both measure the non-invasive arterial fingerpressure waveform, there are a number of obvious differences. Therefore, bothdevices are introduced briefly in this chapter.Note: This reference guide addresses the Portapes Model-2 device inparticular, however, since Finometer uses the same measurementmethodology, the guide can also be used by Finometer users.1.2 Related PublicationsThis <strong>Reference</strong> <strong>Guide</strong> is for the operator of the Portapres and Finometer devices. Itprovides background information about both devices. Other relevant documentsare:Portapres Model-2; User’s <strong>Guide</strong>The User’s <strong>Guide</strong> describes the installation and operating instructions, and routinemaintenance procedures.Portapres Model-2; Carrying InstructionsInstruction guide for the patient carrying Portapres.Portapres Model-2; NiCd Battery ChargerInstructions for the use of the Portapres Model-2 NiCd battery charger.
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong> <strong>Reference</strong> <strong>Guide</strong> 8BeatScope, User’s <strong>Guide</strong><strong>Guide</strong> to the Windows NT/9x/2000 BeatScope beat analysis software package.Finometer User’s <strong>Guide</strong>Operator instructions guide for the Finometer1.3 FinapresBoth Portapres and Finometer are special versions of the <strong>TNO</strong> Finapres, a noninvasivedevice, which measures blood pressure continuously in the finger.Finapres was developed and manufactured in small numbers by <strong>TNO</strong> TPDBiomedical Instrumentation and was later commercially available as the OhmedaFinapres 2300 NIPB monitor. The <strong>TNO</strong> Finapres and the commercial OhmedaFinapres are no longer available.1.4 PortapresThe Portapres blood pressure device is similar to Finapres and manufactured by<strong>TNO</strong> TPD Biomedical Instrumentation. Portapres has a number of features thatmake the device suitable for ambulatory use.• The device is light weight and battery powered• Portapres measures blood pressure in two (adjacent) fingers. By pressurizingthe finger cuffs alternately the slight discomfort when a cuff is wrapped arounda finger longer than about an hour, can be prevented.• Portapres uses a hydrostatic height correction system to compensate forvertical movement of the hand with respect to heart level and the concomitantpressure changes in the finger blood pressure.• Portapres stores the data of 24 hr finger arterial blood pressure waveform,hydrostatic height, event marker, and status messages on its built-in FlashMemory Card.• A Control unit is used to enter data, to set-up the device and to start ameasurement. During a measurement this unit may be disconnected. Thisreduces the overall weight of the device.1.5 FinometerFinometer is a blood pressure device similar to Finapres, but with a number ofsignificant extensions.
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong> <strong>Reference</strong> <strong>Guide</strong> 9• Finometer offers the non-invasive monitoring of continuous brachial arteryblood pressure, based on the finger arterial pressure measurement asimplemented in Finapres and Portapres, and published pressure waveformreconstruction and calibration methods.• Cardiac output, based on the Modelflow cardiac output method, developed by<strong>TNO</strong> TPD Biomedical Instrumentation, and other hemodynamic data areavailable in real time on a built-in color display.• Similar to Portapres the Finometer is equipped with a height correctionsystem, a built-in disk for data storage and a serial interface with a PC.1.6 Contacting <strong>TNO</strong>-Biomedical InstrumentationIf you need assistance, service, or further information contact:<strong>TNO</strong> TPD Biomedical InstrumentationAcademic Medical Center, Suite K2-228Meibergdreef 9NL - 1105 AZ AmsterdamThe NetherlandsPhone : +31 20 566 5838Fax : +31 20 697 6424E-mail : bmi@tpd.tno.nlor via the BMI Web site : www.bmi-tno.nl
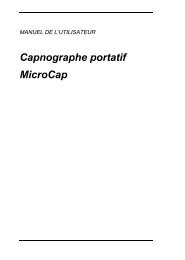
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong> <strong>Reference</strong> <strong>Guide</strong> 102 Measurement principle2.1 IntroductionPortapres and Finometer use the volume-clamp method, originally described by theCzech physiologist Jan Peñáz [PEÑÁZ 1969, PEÑÁZ 1973], to measure bloodpressure in the finger in a manner similar to Finapres. In this method the diameterof an artery under a cuff wrapped around the finger is kept constant (clamped), inspite of the changes in arterial pressure during each heart beat. Changes in arterialdiameter, detected by means of an infrared photo-plethysmograph built in thefinger cuff, are opposed by a fast pressure servo controller that changes pressure inan inflatable air bladder, which is also mounted in the finger cuff. An expert systemis used, Physiocal [WESSELING 1995], to define and maintain the correct diameterat which the finger artery is clamped. The volume-clamp method, and thePhysiocal algorithm are addressed in this chapter.2.2 <strong>Finger</strong> cuffPortapres and Finometer use wraparound finger cuffs.adebcabcdeAir hose connectorCuff cable connectorCuff air bladderLight detector (Photo Diode)Light source (Light Emitting Diode,LED)Figure 2.1 <strong>Finger</strong> cuffThe main components of the finger cuff are an inflatable air bladder, and aplethysmograph consisting of a light source and a light detector. The light source is
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong> <strong>Reference</strong> <strong>Guide</strong> 11a LED (Light Emitting Diode) emitting infrared light. The light detector in thefinger cuff is an infrared photodiode.The air bladder is connected to the Portapres/Finometer frontend unit via an airhose and both components of the infrared plethysmograph via a cuff cable. Thefrontend unit is connected via the frontend cable and air hose to the main unit andpump unit in the Portapres waist belt. Finometer uses a combined air hose andelectrical cable to connect the frontend.Figure 2.2 Frontend unit, finger cuffs and height correction unit.2.3 PlethysmographThis section shows an example of the signal coming from a finger infraredplethysmograph when the pressure in the finger cuff is kept constant. One of theheart beats in the figure is marked by two vertical lines, representing the beginsystole and end diastole of the beat. A sudden rise in finger intra-arterial pressureduring systole causes an increase in arterial diameter, which is detected as anincrease in light absorption and thus as a decrease in the signal detected by theplethysmograph. During the diastolic phase of a beat, when blood pressure declinesgradually, the blood is expelled from the artery and consequently the amount oflight detected by the photodiode will increase again.The mean plethysmogram level is further referred to as DC-plethysmogram, thepulsation of the plethysmogram as AC-plethysmogram. Portapres displays the DCand AC component of the plethysmogram during the start-up phase of ameasurement, and on request when the FINGER key is pressed (refer to thePortapres Model-2 User’s <strong>Guide</strong>). On the display of the Portapres control unit theDC-plethysmogram is abbreviated as V=, the amplitude of the plethysmogram asV:, where the ‘V’ is short for volume signal. Finometer users findplethysmographic information in the ‘Physiocal’ tab if Finometer is in ‘ResearchMode’.
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong> <strong>Reference</strong> <strong>Guide</strong> 12Plethysmogram (a.u.)300250200150100500DC-plethBeatAC-pleth200Cuff pressure150100500Time (s)Figure 2.3 Plethysmogram2.4 The pressure-diameter relationshipThe relationship between changes in arterial diameter and changes in intra-arterialpressure depends on the mechanical properties of the artery. When the artery isvery compliant (low rigidity) diameter changes are relatively large, whereasdiameter changes in stiff arteries are small. It is a well known fact that arterialcompliance depends on the transmural pressure, i.e. the pressure differencebetween the pressure inside the artery and the pressure of the surrounding tissue[LANGEWOUTERS 1986]. At high transmural pressures, when cuff pressure is low,the arterial diameter is relatively large. Therefore, the artery is distended andbecomes stiff, causing small diameter changes. When transmural pressure is low,i.e. when cuff pressure is high with respect to mean blood pressure, the artery isalmost collapsed, and diameter changes will be also small. At near zero transmuralpressure, i.e. when the pressure inside the artery equals the pressure in the fingercuff, diameter changes are largest. This observation was first published by Mareyin 1876 [MAREY 1876]. Figure 2.4 shows a stylized pressure-diameter (p-d) plot ofa finger artery measured in vitro.
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong> <strong>Reference</strong> <strong>Guide</strong> 13d (a.u.)relaxedContractedPt (mmHg)Figure 2.4 Stylized p-d diagrams of human fingers, Pt is the transmural pressure, dthe diameter.Near zero transmural pressure the p-d curve is steepest, that is for a given pressurechange the diameter change will be largest.It is important to realize that at zero transmural pressure the artery is not collapsed.To fully collapse the finger artery requires a cuff pressure larger than the fingerintra-arterial pressure. At zero transmural pressure the artery is 'unloaded'.2.5 Volume-clamp methodWhen the volume clamp method of Peñáz is used the finger cuff pressure is notconstant but variable. Portapres and Finometer are, therefore, not calibratedplethysmographs: the cuff pressure changes actually take away (most of) theplethysmogram. If during systole an increase is detected in arterial diameter thefinger cuff pressure is immediately increased by the servo-controller system toprevent the diameter change. Since the servo-controller system is designed toprevent any change in diameter, the artery is effectively clamped at a certaindiameter, the ‘set-point’. If this diameter corresponds with the unstretched orunloaded state of the finger artery, transmural pressure is zero all the time.Therefore, when the volume-clamp method is active at the proper unloadeddiameter of the finger artery, finger cuff pressure equals intra-arterial pressure.
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong> <strong>Reference</strong> <strong>Guide</strong> 14A servo-controller system usually defines a target value or setpoint and a measuredvalue that is compared with this setpoint. In the servo-controller the setpoint is thesignal of the plethysmogram (unloaded diameter of the artery) that has to beclamped. The measured value comes from the light detector. The amplifieddifference between setpoint and measured value, ‘the error signal’, is used tocontrol a fast pneumatic proportional valve in the frontend unit. This proportionalvalve, modulates the air pressure generated by the air compressor, and thus causeschanges in the finger cuff pressure.FLSV (PG)C 2SWPCDA PID PAC 1M (CP)EPTCompr.Figure 2.5 Block diagram of the volume clamp method of Peñáz.The original block diagram of the method as developed by Peñáz is visualized inFigure 2.5. The arrows indicate a closed servo control loop. The signal V (PG) ofthe photo-plethysmograph, consisting of a light source (L), and photocell (PC)built in a cuff (S) around the finger (F), is compared to a fixed setpoint value (C1).A difference between signal and setpoint, is amplified by DA, PID and PA, anddrives the proportional valve (EPT). Cuff pressure is monitored by the manometer(M). If the switch SW is closed, the servo feedback loop is opened, and a steadycuff pressure (C2) can reach the finger.
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong> <strong>Reference</strong> <strong>Guide</strong> 152.6 Physiocal algorithmUnfortunately, defining the correct unloaded diameter of a finger artery is notstraightforward. An additional problem is that changes in hematocrit, and changesin stress and tone of smooth muscle in the arterial wall affect the unloadeddiameter. Therefore, the unloaded diameter is usually not constant during ameasurement and has to be verified at intervals. Periods of constant cuff pressureare used to adjust the correct unloaded diameter of the finger artery based on thesignal from the plethysmograph in the finger cuff. A disadvantage of this method isthat the measurement of blood pressure is temporarily interrupted during such aperiod. Therefore, the frequency and duration of the periods of interruption arekept to a minimum.It is obvious from the previous sections that the unloaded diameter is close to theaverage diameter at a pressure level where the amplitude of the pulsations in theplethysmogram is largest. However, using only the amplitude of theplethysmogram is relatively inaccurate. The Physiocal algorithm [WESSELING1995] in Portapres and Finometer, developed by the Dutch physicist K.H.Wesseling, not only uses the amplitude, but also interprets the shape of theplethysmogram during periods of constant cuff pressure. By analyzing theplethysmogram at two or more pressure levels, the Physiocal algorithm, explorespart of the pressure-diameter relation and is able to track the unloaded diameter ofa finger artery even if smooth muscle tone changes. The periodic interruption of afinger blood pressure measurement, with constant cuff pressure levels, is furtherreferred to as ‘Physiocal’.Figure 2.6 shows a typical finger plethysmogram at five cuff pressure levels. Themean blood pressure was about 100 mmHg.• When cuff pressure is below mean blood pressure the arterial diameter isrelatively large and therefore the plethysmographic signal is low. Sincecompliance is low in this state the amplitude of the pulsation is small and theplethysmogram only varies significantly during diastole.• When cuff pressure is above mean blood pressure the artery is collapsedduring a substantial part of every heart beat. The plethysmographic signal ishigh (no absorption of arterial blood), and only varies significantly duringsystole.• When the cuff pressure level equals the average intra-arterial pressure theplethysmogram resembles an inverted pressure waveform. The end-diastolicperiod of the plethysmographic waveform is analyzed during a Physiocal.When the top of the plethysmographic signal at end-diastole is too sharp, meancuff pressure is below mean arterial pressure, when it is too flat, cuff pressure
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong> <strong>Reference</strong> <strong>Guide</strong> 16is too high. The shape of the plethysmogram of course also depends on thestate of the artery, and the smooth muscle tone see also Figure 2.4. Therefore,the interpretation ‘too sharp’ and ‘too flat’ always has to be verified byanalyzing the plethysmogram at one or more other pressure levels200Intra-arterial pressure150100500<strong>Finger</strong> arterial pressureCuff pressureTime300Plethysmogram (a.u.)250200150100500Figure 2.6 <strong>Finger</strong> plethysmogram at five cuff pressure levels2.7 Example of a normal PhysiocalDuring a normal Physiocal the blood pressure measurement is interruptedimmediately after the detection of the systolic phase of the heart beat. The firstpressure level is located between diastolic and systolic finger arterial pressure. Theshape and amplitude of the plethysmogram are analyzed and also compared withprevious Physiocal periods. If the end-diastolic phase of the plethysmogram has the
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong> <strong>Reference</strong> <strong>Guide</strong> 17correct shape, an additional measurement of the plethysmogram is performed at adifferent cuff pressure level to confirm that the determination of the unloadedvolume is indeed optimal. The Physiocal algorithm also checks that the unloadeddiameter is not too close to the fully collapsed state of the finger artery.200200<strong>Finger</strong> blood pressure (mmHg)15010050<strong>Finger</strong> blood pressure (mmHg)1501005000 5 1000 5 10Time (s)Time (s)Figure 2.7 Normal Physiocals with either two or three pressure levels2.8 Example of a multi-step PhysiocalIf the correct unloaded diameter can not be confirmed during a normal Physiocaladditional pressure steps are added automatically.200150Portap (mmHg)1005000 5 10Time (s)Figure 2.8 Multi-step Physiocal
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong> <strong>Reference</strong> <strong>Guide</strong> 18This is usually observed immediately after starting a new measurement and whenthe smooth muscle tone is not stable. If these so-called multi-step Physiocals arefrequently observed during a measurement accuracy of the finger blood pressuremay be reduced.2.9 Example of a Physiocal with variable pressure levelsIf during a finger blood pressure measurement the device is unable to recognizebeats in either the finger blood pressure or the plethysmogram the Physiocalalgorithm uses variable pressure levels instead of constant pressure levels during aPhysiocal. In this situation it is assumed that there is no intra-arterial pressurechange during a heart beat, as is the case during certain phases of open heartsurgery. However, it is also possible that this special Physiocal is performed after aperiod of movement artifacts during which the software was unable to recognizeheart beats. During a special Physiocal an inverted pressure waveform issuperimposed on the constant levels. The resulting plethysmogram is used as if theintra-arterial pressure was varying and not the cuff pressure.200<strong>Finger</strong> blood pressure (mmHg)1501005000 5 10Time (s)Figure 2.9 Special Physiocal with variable pressure levels2.10 <strong>Pressure</strong> staircase at the start of a measurementDuring the start-up phase of a finger blood pressure measurement, the cuff pressureis increased stepwise while analyzing the plethysmogram. Based on the amplitudeand shape of the plethysmogram the stepwise increase in pressure is stopped as
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong> <strong>Reference</strong> <strong>Guide</strong> 19soon as cuff pressure is above systolic pressure. Then a Physiocal is performed andthe actual blood pressure measurement is started. The startup procedure usually nottakes more than 15 seconds.150Portap (mmHg)1005000 5 10 15 20Time (s)Figure 2.10 Staircase start-up procedure2.11 Physiocal frequencyIn the first one or two minutes after the start of a finger blood pressuremeasurement the blood pressure device has to deal with the emptying of smallmicrovessels from blood under the cuff. The absorption of the light between lightsource and light detector usually decreases due to this effect. This change inabsorption has nothing to do with the unloaded diameter of the finger artery and iscompensated for by Portapres/Finometer.Since this effect is more pronounced immediately after starting a blood pressuremeasurement, a Physiocal procedure is scheduled initially after every 10th heartbeat. As soon as the setpoint has become sufficiently stable this interval isgradually increased to 70 beats, normally within 4 minutes. An example is shownin Figure 2.11.If stability of the setpoint can not be confirmed, e.g. after movement artifacts, or ifthe change in setpoint is considered too large, the frequency of Physiocal willincrease temporarily automatically.
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong> <strong>Reference</strong> <strong>Guide</strong> 20<strong>Finger</strong> blood pressure (mmHg)2001501005000 60 120 180 240 300Time (s)Figure 2.11 Physiocal frequency2.12 Note on blue fingertipsDuring a normal finger blood pressure measurement some coloring of the finger tipdistal from the finger cuff is observed. The also occurring whiteness of the fingerphalanx below the finger cuff is usually invisible.The arteries below the finger cuff are unloaded, that is, the arterial walls are held atzero transmural pressure and they are therefore at their unstressed diameter, cf.2.5). Unstressed arteries still have about 60% of their original distended diameteror approximately 1/3 or 1/2 their original cross-sectional area and volume. Theother blood vessels below the cuff are collapsed. Therefore, all the vessels behindthe cuff, in the finger tip, are at instantaneous arterial pressure including the microcirculationand the veins. Thus blood entering the finger tip during systole can onlyleave during diastole, when the pressure in the vessels of the finger tip is higherthan the pressure more proximal from the cuff. This causes some congestion. Sinceduring a blood pressure measurement the blood in the finger tip is less efficientlyrefreshed the reduced wash out of metabolites and increased de-oxygenation of thevenous blood, causes blue finger tips. Note, however, that the Physiocal algorithmalways checks that the artery is sufficiently open during a measurement. Inflow intoand outflow from the venous compartments is facilitated by the enlarged capillarydiameters at the arterial pressures their walls sustain. It is also facilitated by relaxedarterioles (including the arterio-venous anasthomoses). Relaxed arteries are present
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong> <strong>Reference</strong> <strong>Guide</strong> 21in the absence of sympathetic nervous tone, vasopressors, or cold. Relaxedarterioles, and a normal colored finger tip, can be seen frequently during normalsleep.Gravenstein (GRAVENSTEIN 1985) reported a substantial capillary oxygen pressureremaining in the finger tip distal of a finger cuff from 49 to 58 mmHg compared to80 mmHg normally and pulse oxymeter saturations of about 93% with muchvariability.With all vessels in the distal finger tip at arterial pressure, one would expect anincreasing diameter of that part of the finger, since at high capillary pressureincreased leakage of liquid through capillary pores is expected to fill the interstitialspace, however this has not been observed. A slight decrease of finger diameterunder the cuff is usually observed after a prolonged period of blood pressuremeasurement. This decrease in finger diameter can be attributed to interstitialliquid being pressed out into the capillaries and the lymphatic system, to return tothe veins. Also, red blood cells trapped in the micro-circulation by the applied cuffpressure have been observed to wash out in a period of several minutes.Although this evidence does not prove that damage to the finger monitored withPortapres/Finometer can not occur, no problems have been apparent since theintroduction of finger blood pressure measurement more than 20 years ago.In order to avoid long lasting congestion discomfort, Portapres is equipped with atwo-finger switching mode that can automatically switch between two fingers inalternation.
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong> <strong>Reference</strong> <strong>Guide</strong> 223 Measurement accuracyPortapres/Finometer enables the measurement of continuous arterial blood pressurein the finger. It is important to realize that the finger arterial blood pressure maydiffer from the blood pressure measured in the brachial artery or aorta. There maybe differences in waveform and in absolute level. As a consequence theinterpretation of finger blood pressure measurements with Portapres/Finometer, inparticular when the outcome of such measurements is used as an adjunct in apatient's diagnosis, should be performed with care.The information in this chapter focuses on Portapres. However, the discussion alsoholds true for the Finometer, when finger blood pressure is measured withwaveform filtering and level correction methods disabled.3.1 Comparison with intra-arterial blood pressureSince blood pressure readings depend on the site of pressure measurement acomparison of Portapres finger blood pressure and intra-arterial pressure is alsoaffected by the choice of this intra-arterial pressure site. We will focus on thefinger and brachial artery measurement sites.3.1.1 <strong>Finger</strong> arterial pressureAlthough it is not possible to measure intra-arterial pressure in a finger artery thereis evidence that Portapres indeed measures finger arterial blood pressure.In simultaneous recordings with two finger blood pressure monitoring devices itcould be determined that the unloaded diameter determined by Physiocal was closeto the theoretically required one-quarter to one-half of the open diameter level[WESSELING 1995]. At this diameter the transmural pressure is close to zero, andtherefore finger cuff pressure is equal to intra-arterial finger blood pressure.A second basis for the assumption that Portapres correctly measures finger arterialblood pressure is a phenomenon that usually can be observed in a pressure tracingat the start of a Portapres measurement.During start-up a pressure staircase is performed to monitor fingerplethysmographic values at different pressure levels. The pressure staircase iscontinued until the arterial diameter changes as detected by the plethysmogramvirtually disappear, provided cuff pressure is above 100 mmHg. Therefore, at thelast pressure level in a pressure staircase finger cuff pressure is just above systolic
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong> <strong>Reference</strong> <strong>Guide</strong> 23pressure. When the continuous finger blood pressure measurement is startedimmediately after the pressure staircase, and when blood pressure is sufficientlystable, the systolic pressure usually matches the cuff pressure during the last step inthe pressure staircase.<strong>Finger</strong> blood pressure (mmHg)150100500Systolic pressure0 5 10 15 20Time (s)Figure 3.1 Relationship between finger arterial systolic pressure and start-upstaircase procedureIf, however, the arterial blood pressure is not stable, or in case of arrhythmia’s,movement artifacts, or contracted arteries, Portapres may decide to explore thepressure-diameter relationship of the finger artery at higher pressure levels duringthe staircase procedure. Therefore, the similarity of the pressure during the last stepof the staircase and the finger arterial systolic pressure, as shown in Figure 3.1, isnot always present.3.2 Brachial arterial pressureIf simultaneous tracings of finger arterial pressure (Finapres or Portapres) andbrachial pressure are available the pressure tracings usually look virtually identical,apart from a (small) level shift and sometimes some pulse amplification.In Figure 3.2 the finger pressure tracing differs from the brachial pressure tracingmainly because of the Physiocal interruptions around 40, 100 and 150srespectively.
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong> <strong>Reference</strong> <strong>Guide</strong> 24<strong>Pressure</strong>0 20 40 60 80 100 120 140 160 180 200Time (s)Figure 3.2 Example of a simultaneous tracing of brachial (black) and fingerarterial blood pressure (gray tracing, plotted with a pressure offset), (data fromstudy of Harms et al, published in Clin Sci 1999; 97; 291-301).3.2.1 Pulse wave distortion<strong>Pressure</strong> pulsations are progressively distorted on their way towards the periphery.<strong>Finger</strong> blood pressure waveforms are more undulatory than brachial arterialpressure waveforms because of reflections of the systolic pulse wave in the arterialsystem of the arm. When finger pressure is compared to the intra-radial pressurethe distortion is less pronounced [SETTELS 1985].The next two figures (Figure 3.3 and Figure 3.4) provide two examples ofsimultaneous recordings of brachial and non-invasive finger arterial pressure in awoman aged 73 and a man aged 27. Note the small delay between the brachialpressure wave and the finger pressure wave due to time needed for the pulse waveto travel along the arm artery.
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong> <strong>Reference</strong> <strong>Guide</strong> 25200Brachial pressure<strong>Pressure</strong> (mmHg)15010050<strong>Finger</strong> pressure025 26 27 28 29 30Time (s)Figure 3.3 <strong>Finger</strong> and brachial artery pressure waveforms in a woman aged 73),(data from a study in elderly healthy volunteers by Rongen et al, Am J Hypertens8: 237-248)200<strong>Pressure</strong> (mmHg)15010050<strong>Finger</strong> pressureBrachial pressure025 26 27 28 29 30Time (s)Figure 3.4 <strong>Finger</strong> and brachial artery pressure waveforms in a man aged 27. (datafrom a study in young healthy volunteers by Harms et al, Clin Sci 1999, 97, 291-301).
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong> <strong>Reference</strong> <strong>Guide</strong> 263.2.2 <strong>Pressure</strong> gradientMean finger blood pressure is lower than mean intra-arterial brachial pressure dueto a pressure gradient over the arm arteries caused by flow. This pressure decaywas found to increase with age, whereas pulse wave amplification is highest in theyoung. Due to the combined effects of pulse wave amplification and pressuredecay, systolic pressure is elevated in the young but equal to or even lower thanbrachial pressure in elderly subjects. The mean pressure gradient is clearly presentin Figure 3.3 and Figure 3.4.3.3 Bias and precisionIn a group of 53 subjects, described in previous studies [BOS 1992, IDEMA 1987,RONGEN 1995] the following data were obtained for brachial and finger pressure:Brachial <strong>Finger</strong> <strong>Finger</strong>-BrachialSystolic 169 ± 33 163 ± 29 -5 ± 15Diastolic 89 ± 17 81 ± 18 -9 ± 10Mean 118 ± 22 104 ± 21 -13 ± 11Table 3-1 <strong>Pressure</strong>s and pressure differences, (53 subjects, aged 22-83 years, allnumbers in mmHg, mean±SD).These numbers tend to vary somewhat per study, presumably because of agedifferences of the subjects in the studies.Thus averaged over a study population finger arterial mean pressure is about 10mmHg lower than intra-arterial pressure in the brachial artery, but individualdifferences may be larger.Although Portapres does not meet all requirements for non-invasive blood pressuremonitoring, according to e.g. the AAMI, the tracking accuracy of Portapres isconsidered sufficiently good to study blood pressure changes, during e.g.orthostatis and cardiovascular maneuvers such as Valsalva straining [IMHOLZ1998].3.4 Clinical useDue to the non-brachial pressure site Portapres should not be used as a replacementfor the upper arm cuff blood pressure measurement devices that are normally used
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong> <strong>Reference</strong> <strong>Guide</strong> 27in a clinical setting. However, Portapres has proven to be very useful in ambulatorylong-term measurements, e.g. to study the circadian 24h blood pressure profile, andin conditions where fast hemodynamic changes are expected, such as duringcardiovascular stress testing, orthostatic tolerance testing, and in many otherphysiological studies. See Appendix A for a list of references.In general all these studies have in common that a Portapres finger blood pressuremeasurement was preferred over a more conventional blood pressure measurementdevice for one or more of the following reasons:• Non invasive measurement• Continuous beat-to-beat blood pressure and heart rate data available• Possibility to perform a comprehensive hemodynamic analysis on the fullpressure waveform with the Modelflow cardiac output software that isincorporated in the <strong>TNO</strong> BeatScope software program.• Ambulatory measurements and data storage on a built-in memory card.3.5 Waveform filtering and level correction methodsThe distortion of the pressure waveform along an artery can be investigated withspecial mathematical techniques such as Fourier spectra. These analyses showedthat the distortion of finger arterial pressure is caused by a resonance, a tendency ofthe arm arterial system to oscillate, at about 8 Hz. The amplification of pulsepressure that is a consequence of this resonance is attributed to a gradual decreasein arterial diameter, to an increase arterial stiffness of the distal arterial tree and towave reflections.Recently a method has been described to derive brachial pressure waveforms fromfinger arterial pressure by means of waveform filtering. Additionally, a method wasdeveloped to correct for the pressure gradient using a regression equation. Bothmethods are addressed in the following sections.3.5.1 Wave distortion correctionFigure 3.5 shows the transfer function from brachial to finger pressure with amaximum at about 8 Hz. The transfer function was calculated by comparingsimultaneous brachial and finger pressure waveforms in a group of patients[GIZDULICH 1996]. The resonance peak at 8 Hz causes oscillatory distortions in thefinger pressure waveform. Using Fourier techniques Gizdulich et al. succeeded inderiving a digital function that can be used to filter a finger pressure waveformback to a brachial pressure waveform.
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong> <strong>Reference</strong> <strong>Guide</strong> 28After this waveform filtering the mean pressure level is not yet equal to brachialmean blood pressure level. A correction method to get a mean pressure level that ison average correct is described next.Figure 3.5 Transfer function from finger to brachial), (Transfer function frombrachial artery to finger, with a maximum near 8Hz. The second curve with ananti-resonant dip at 8Hz is the waveform filter of Gizdulich et al [GIZDULICH1996])3.5.2 <strong>Pressure</strong> gradient correctionUsing the waveform distortion correction method described in the previous sectiona pressure level correction was developed that makes use of a multiple regressionmodel of the blood pressure differences between brachial artery and finger arteryas dependent variable upon diastolic and pulse pressure after wave distortioncorrection [GIZDULICH 1997]:3.5.3 Combination of waveform filtering and level correctionWhen both waveform filtering and level correction are applied on themeasurements in Table 3-1 the following table is found. On average the brachialand non-invasive finger blood pressure readings are virtually identical. Relativelylarge individual differences, however, are still found, as seen in standarddeviations.
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong> <strong>Reference</strong> <strong>Guide</strong> 29Brachial <strong>Finger</strong> <strong>Finger</strong>-Brachial reBAP –BrachialSystolic 169 ± 33 163 ± 29 -5 ± 15 0 ± 15Diastolic 89 ± 17 81 ± 18 -9 ± 10 -0 ± 8Mean 118 ± 22 104 ± 21 -13 ± 11 -1 ± 9Table 3-2 <strong>Pressure</strong>s and pressure differences, reBAP is the reconstructed brachialartery pressure (53 subjects described in [BOS 1992, IDEMA 1987, RONGEN1995], aged 22-83 years, [mmHg] ±SD)3.6 BeatScope software programThe BeatScope software package, developed by <strong>TNO</strong> TPD BiomedicalInstrumentation, enables the beat-to-beat analysis of the original (raw) fingerarterial pressure signal and also enables the usage of waveform filtering and levelcorrection methods to obtain brachial pressure waveforms.200Brachial pressure<strong>Pressure</strong> (mmHg)15010050<strong>Finger</strong> pressure<strong>Finger</strong>BrachialRaw_diasLevl_diasRaw_systLevl_syst025 26 27 28 29 30Time (s)Figure 3.6 <strong>Finger</strong> and brachial artery pressure waveforms and beat data in awoman aged 73), (The triangles are at the diastolic and systolic pressure of theraw finger pressure signal, the square symbols are diastolic and systolic readingsafter waveform filtering and level correction with BeatScope).
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong> <strong>Reference</strong> <strong>Guide</strong> 30With the Modelflow cardiac output method [WESSELING 1993], as implemented inBeatScope, the following data are computer for every heart beat: The instant ofupstroke, systolic, diastolic and mean blood pressure, heart rate, inter-beat interval,stroke volume, cardiac output, ventricular ejection time, peripheral resistance,aortic characteristic impedance and aortic compliance.200<strong>Pressure</strong> (mmHg)15010050<strong>Finger</strong> pressureBrachial pressureBrachial<strong>Finger</strong>Raw_diasLevl_diasRaw_systLevl_syst025 26 27 28 29 30Time (s)Figure 3.7 <strong>Finger</strong> and brachial artery pressure waveforms and beat data in a managed 27, (The triangles are at the diastolic and systolic pressure of the raw fingerpressure signal, the square symbols are diastolic and systolic readings afterwaveform filtering and level correction with BeatScope).
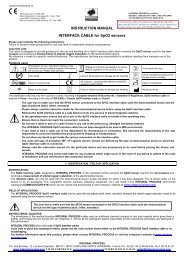
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong> <strong>Reference</strong> <strong>Guide</strong> 314 Practical guidelinesIn this chapter a number of guidelines for a reliable finger blood pressuremeasurement are discussed. The chapter extends the information provided in theChapter 'Performing a measurement' in the Portapres User's <strong>Guide</strong>.4.1 Selecting the proper handIt is recommended to apply the finger cuff(s) on the non-dominant hand so that thesubject can use the dominant hand for daily activities, e.g. to write notes in a diary.Ask the subject whether there are problems with cold or painful fingers, beforedeciding which hand to choose.4.2 Selecting the proper cuffThere are finger cuffs in three sizes: small, medium and large.CUFF SIZINGbladderhiatusgoodfrictionareabladdertouchsmallfrictionareabladderoverlapCuff too small Correct fit Cuff too largeSize:Fits [mm]:S - white 45 - 55M - beige 55 - 65L - blue 65 - 75If in doubt choose smaller cuffFigure 4.1 Cuff size selection depending on circumference (mm) of the fingerEvery size has its color: white for small cuffs, beige for medium cuffs and blue forlarge cuffs. A finger cuff should be wrapped around the middle phalanx of a finger.Best results are obtained on the middle finger and the ring finger although the
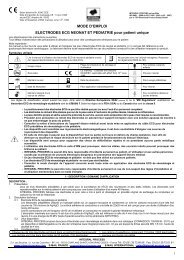
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong> <strong>Reference</strong> <strong>Guide</strong> 32index finger can be used almost equally well. <strong>Finger</strong> cuffs are conically shaped asfingers are.The preformed conical finger cuffs are not designed for application to the thumb.Only apply a finger cuff to the thumb when it is impossible to measure fingerarterial pressure on any other finger and be alerted that incorrect pressure levelsmay result.4.3 Wrapping the cuff correctlyTo wrap a finger cuff around the finger:• Open the finger cuff just enough to be able to see the LED and photodiodecomponents• Place the finger in the cuff such that the LED and photodiode (or photocell,PC) are symmetrically placed on each side of the finger's soft palmar parts andhave a centered position on the middle phalanx.• Lead the cuff cable and air hose in between two fingers to the volar side of thehand to reach the frontend unit.• Make sure the finger cuff is placed centered between two knuckles, touchingeach knuckle.• Wrap the finger cuff so that the airbladder follows the curvature of the fingerskin without noticeable clearance between airbladder and skin. The fingercuffs are designed so that correct wrapping is almost natural. Wrapping wasnot tight enough when it is possible to easily rotate or to shift the cuff from thefinger.• Insert the cuff cable and air hose connectors into the fronted unit.• Repeat steps 1 to 6 for a second finger.
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong> <strong>Reference</strong> <strong>Guide</strong> 33WRONGCable and tube pointIn the wrongdirection.WRONGCuff is rotated 180 degrees.The conicalshape of thecuff does notmatch thefinger.The photoplethysmographis not positionedin front of thearteries.CORRECT CUFF WRAPPINGCuff wrapping instructions:1. Point cable and tube towards wrist.2. Center cuff between joints.bone3. Center LED and photodiodesymmetrically.4. Wrap cuff tightly.5. Place hand onside, thumbup.LED photodiodearteriesfinger cross sectionWRONGCuff is shifted proximally.WRONGCuff is rotated.The middlephalanx isthe preferredposition.The photoplethysmographis not positionedin front of thearteries.Figure 4.2 Cuff wrapping
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong> <strong>Reference</strong> <strong>Guide</strong> 34It is a common mistake to wrap a cuff not tight enough around a finger. Inparticular on small fingers with white (small) cuffs, cuff application requires someskill.When you remove a finger cuff, after stopping a measurement, it is recommendedto inspect the finger to see if you can find the place where the two components ofthe plethysmograph have pressed on the finger skin. Usually, some coloring ofthese pressure points can be seen immediately after removing the cuffs. Verify thatthe pressure points were correctly centered between the knuckles andsymmetrically placed.4.4 Selecting a finger switching intervalThe selection of a finger switching interval depends on the kind of measurementyou are going to perform. For measurements longer than 2 h always select fingerswitching, since a prolonged measurement on one finger can be unpleasant for thesubject. Four finger switching periods can be selected : 1, 15, 30 and 60 min. The 1min finger switching interval is for maintenance purposes only. It can also be usedto get a quick impression of the blood pressure measurement in two fingers beforestarting a 24 h blood pressure measurement. However, you should realize that ameasurement of only one minute will not provide stable and reliable blood pressurereadings. The selection of one of the three remaining finger switching intervalsdepends on the protocol of the measurement. During and in the first 1 to 3 minafter a finger switching procedure blood pressure values are less reliable.For measurements up to one hour it is also recommended to select finger switching,and to set the finger switching interval to 60 min. The reason for that is that a runtimeerror such as ‘Connect cuff cable’ or ‘Unacceptable P/V’ will not completelystop a measurement and will not close the file on the built-in memory card, as is thecase if ‘finger fixed’ on C1 or C2 is selected. When finger switching is selected,Portapres will try to restart a measurement after a waiting period and dataacquisition is not interrupted.Use the ‘finger fixed’ selection in measurements of up to one or two hours that youdo not want to be interrupted by a finger switching procedure. To avoid analysisproblems due to pressure differences between fingers it is also recommended to usethe same finger in measurements of up to 1 or 2 hours.<strong>Finger</strong> switching can only be configured when Portapres is in Ready mode. Duringa blood pressure measurement it is not possible to force or to delay a fingerswitching procedure.
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong> <strong>Reference</strong> <strong>Guide</strong> 354.5 Two finger agreement in a finger switchingmeasurement<strong>Finger</strong> arterial pressure from the index, middle and ring finger are not necessarilyequal, although differences are usually small. In some measurements a pressuredifference between fingers is observed. This can both be caused by physiologicaldifferences between fingers and by the differences in cuff application on bothfingers.If a cuff is not wrapped tight enough, i.e. when it is too easy to pull the cuff from afinger, blood pressure readings are too high. This is caused by a pressure gradientover the airbladder when the airbladder is inflated too much. Portapres/Finometerthen needs a higher cuff pressure to achieve the same diameter changes in thefinger artery. Likewise, if a cuff is wrapped (much) too tight, as is illustrated in thefigure, cuff pressure readings may be too low.<strong>Finger</strong> blood pressure(mmHg)150100500Cuff wrappedOKnot tight enough0 1 2 3 4 5Time (s)too tightFigure 4.3 Examples of consequences bad cuff wrapping4.6 Applying hydrostatic height correctionThe height correction unit (Figure 4.4) of Portapres/Finometer should be used,unless it can be guaranteed that the cuffed finger remains at heart level during a
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong> <strong>Reference</strong> <strong>Guide</strong> 36measurement. Without an active height correction system a hydrostatic error of 10mmHg or even more is hard to detect and easily made, in particular when the armis stretched and the hand is not close to the chest.The height compensation system consists of a liquid filled tube connected at oneend to a pressure transducer. The other end is closed with a very compliant plasticbag contained in a small cylindrical housing. The tube material and liquid arematched with respect to the coefficient of linear thermal expansion. During ameasurement the transducer is placed at the measured finger and the compliantending at reference level. Thus, height changes of the measured finger arecontinuously sensed.Figure 4.4 Height correction unitHeight level is negative when the hand is below reference level, positive abovereference level. The height correction transducer nulling must be checked beforestarting a Portapres/Finometer measurement and when necessary a nullingprocedure should be performed to take into account its actual offset, as is describedin the Portapres User’s <strong>Guide</strong> and in the Finometer User’s <strong>Guide</strong>.The height signal is low pass filtered and added to the finger pressure. Thus, slowchanges in blood pressure due to hydrostatic effects are compensated. Dynamicpressure effects due to quick hand movements are not fully compensated and may,therefore, introduce motion artifacts. For optimal results, therefore, fast movementsof the measured hand should be avoided.Figure 4.5 shows an example of a blood pressure recording where the hand isinitially at heart level and then suddenly lowered 27 cm (20 mmHg). Withoutheight correction system the hydrostatic height difference causes an increase infinger pressure of about 20 mmHg. When the height correction system is activeblood pressure measured in the finger is hardly affected. However, often a smallchange in pulse pressure (difference between systolic and diastolic pressure) is
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong> <strong>Reference</strong> <strong>Guide</strong> 37apparent after a change in position of the hand with respect to heart level. Thisdifference in pulse pressure has been attributed to a pulse amplification due to theincrease in rigidity of the artery when intra-arterial blood pressure is increasedsubstantially. This physiological response is not compensated for inPortapres/Finometer.The height reference level should be selected carefully. If the subject is walkingaround or sitting it is best to place the reference part on the chest at the level of theright atrium in the mid-axillary line. In the recumbent position it is best to place thereference ending at mid chest level. If the experiment focuses on the dynamicresponse of the hemodynamic system after a change in posture it is usually best tokeep both the transducer and the reference ending at the level of the right atrium toavoid a dynamic response of the height correction system.As a general rule try to keep the cuffed fingers approximately at heart level, evenwith a connected height correction unit.Figure 4.5 <strong>Pressure</strong> change upon lowering the hand (27 cm) without (left) and with(right) height correction4.7 Improving and checking experimental conditions4.7.1 Patient instructionsIf blood pressure is measured on cold fingers, the measurement can be difficult oreven impossible. Therefore, it is recommended to do measurements only at roomtemperature, or to keep the hand warm during ambulatory measurements. Ask thesubject to wear comfortable and sufficiently warm clothes. Make sure the subject is
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong> <strong>Reference</strong> <strong>Guide</strong> 38in an environment at room temperature at least 15 min before the start of ameasurement, especially in winter time. It is important not only to keep the handand fingers warm, but also the arm and neck.• Awake subjects should be comfortable.• Try to distract the attention from the measurement if the subject is nervous.• Explain the subject, before starting a measurement, that only a slight pulsationin the cuffed finger is felt during the measurement.• Always inform the subjects that interruptions in the pulse can be felt that aredue to the physiological calibration (Physiocal) which is performed atintervals.• It is recommended to follow a fixed protocol during an ambulatory bloodpressure measurement. Try to define periods with a predefined activity, suchas sleeping, sitting, walking etc.• Ask the subject to write daily activities in a diary, or write this informationduring the experiment.Continuous blood pressure is often more variable than expected. If you areinterested in a detailed blood pressure response ask the subject to refrain fromspeaking during the measurement and explain the subject that movements of handand fingers, laughing, coughing etc. may cause waveform artifacts in the fingerblood pressure signal.4.7.2 Diagnostic displayIf the subject has cold hands, e.g. in case of vaso-constriction, it is useful toobserve the plethysmographic values in the display by pressing the FINGER keyon the Portapres control unit. The control unit then may show: V=312V: 34 GN 68in its lower display line, cf. the Portapres User’s <strong>Guide</strong>. The V= value representsthe total amount of infrared light coming through the finger. The V: valuerepresents the pulsatile component, i.e. the changes in finger arterial diameter, cf.Figure 2.3.If the pulsatile component remains small (e.g. less than 5) during the start-upprocedure the artery is strongly contracted and a good pressure measurement isdubious. The artery usually relaxes after a few minutes of monitoring. Therefore, itmakes sense to continue a measurement, once started, in this situation to relax thecontraction of the smooth muscles around the finger artery. If the total amount oflight V= does not change during the procedure the finger is practically bloodless.On a normal finger V= may as much as double between zero pressure and thehighest pressure during the start procedure.
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong> <strong>Reference</strong> <strong>Guide</strong> 39When the finger arteries are too much contracted to start a blood pressuremeasurement with Portapres you can try, as a last resort, to use a medium cuffaround the distal phalanx of the thumb and try to start the measurement.4.7.3 Checking measurement stabilityIt is possible to check measurement stability by monitoring:a) the number of beats between Physiocal periods,b) the number of pressure steps during a Physiocal,c) the occurrence of oscillations, andd) the occurrence of peaked waveforms.Number of beats between Physiocal periodsIt is useful to observe the number of beats between Physiocal periods. The numberof beats between Physiocal periods may stay at 10 or 20 beats for a couple ofminutes. When the number of beats between Physiocal periods reaches 30 orhigher a reliable measurement is obtained in our experience.Number of pressure steps per PhysiocalDuring a Physiocal the plethysmogram is analyzed at a number of steady pressurelevels. Correct Portapres/Finometer pressure readings are in our experienceobtained when the arterial pressure-diameter relation can be determined in two orthree steps. If multi-step Physiocals are frequently observed the blood pressuremeasurement may be less reliable, cf. Section 2.8.Occurrence of oscillationsPortapres/Finometer uses a servo system to make cuff pressure follow intra-arterialfinger pressure. Servo-systems in general and the rather complex one needed inPortapres/Finometer in particular may show oscillations occasionally. Two types ofoscillation can be distinguished, the low on/off or ‘railing’ type and the highfrequency sinusoidal type. The presence of oscillations of either type is detected bythe device and appropriate measures are taken when possible. In the case of highfrequency oscillations the servo system loop gain is automatically reduced untiloscillations stop, and an extra servo controller filter may be switched in. APhysiocal is scheduled after two beats, to confirm the setpoint and servo-systemloop gain. After oscillations stop the loop gain is brought back up if necessary toguarantee sufficient gain for a proper waveform measurement. This ‘gain-up’process may take several heart beats to complete.
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong> <strong>Reference</strong> <strong>Guide</strong> 40Portap (mmHg)5004504003503002502001501005000 1 2 3 4Time (s)Figure 4.6 <strong>Pressure</strong> change upon lowering the hand (27 cm) without (left) and with(right) height correctionIn the case of a railing type of oscillations pressure may be switching betweenalmost zero and almost full cuff pressure. In this occurs the servo setpoint and theloop gain are automatically reduced until railing stops. However, a correctmeasurement is no longer guaranteed until after the next Physiocal. Railing, if itoccurs more than just occasionally in a measurement, is almost always a sign of acuff wrapped too loosely or a cuff too wide or the finger. Stop the measurement,rewrap the finger cuff , possibly on a different finger and then restart.Occurrence of peaked waveformsOn some subjects under certain circumstances the pressure waveform recordedfrom Portapres may show a strong double or triple peaked systolic wave.150Portap (mmHg)1005000 1 2 3 4 5Time (s)Figure 4.7 Peaked waveform while using a large cuff on a medium sized finger.
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong> <strong>Reference</strong> <strong>Guide</strong> 41This is often a sign of a contracted artery but can also be caused by a cuff that istoo large for the finger. The instrument tries to correct for this effect but, ifunsuccessful, can be helped by the operator applying a smaller cuff.4.7.4 Vaso-constrictionClinically, the simple word vaso-constriction describes complex phenomenawhereby the peripheral arteries, the arterioles and peripheral veins, individually ortogether, may be affected to various degrees. We have, based on several studies[WESSELING 1985, LANGEWOUTERS 1986] adopted the habit of distinguishingbetween arteriolar constriction and arterial (and perhaps) venous contraction.A patient in shock treated with a ‘vasodilator’ may show the arterial contractionoften accompanying shock, but arteriolar dilation subsequent to the drug. This is adifficult situation for Portapres/Finometer. If contraction is only moderate, meanpressure is often still measured correctly, but the pulse is too small and thus thesystolic level too low, diastolic somewhat too high compared to brachial pressures.A patient in pain, or taking a deep breath or having cool hands probably hastemporary arteriolar vaso-constriction to some degree. This situation is of littleconsequence for Portapres/Finometer, although a mostly insignificant increase insystolic pressure compared to brachial or aortic may be noted [WESSELING 1985].
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong> <strong>Reference</strong> <strong>Guide</strong> 42<strong>Reference</strong>s<strong>Finger</strong> arterial pressure method1 IMHOLZ BP 1993, Langewouters GJ, van Montfrans GA, Parati G, vanGoudoever J, Wesseling KH, Wieling W, Mancia G: Feasibility ofambulatory, continuous 24-hour finger arterial pressure recording.Hypertension 1993; 21(1): 65-73.2 IMHOLZ BP 1998, Wieling W, van Montfrans GA, Wesseling KH: Fifteenyears experience with finger arterial pressure monitoring: assessment of thetechnology. Cardiovascular Research 1998; 38(3): 605-16.3 LANGEWOUTERS GJ 1986, Zwart A, Busse R, Wesseling KH: <strong>Pressure</strong>diameterrelationships of segments of human finger arteries. Clin Phys PhysiolMeas 1986; 7, 54-55.4 PEÑÁZ J 1973, Photoelectric measurement of blood pressure, volume andflow in the finger. Digest 10th Int Conf Med Biol Engng, Dresden: 1973; page104.5 PEÑÁZ J 1969, Patentova Listina, CISLO 133 205 (1969).6 SETTELS JJ 1985, Wesseling KH. Fin. A. Pres. Non-invasive finger arterialpressure waveform registration. In: Orlebeke JF, Mulder G, van Doornen LJP(eds). Psychophysiology of cardiovascular control. Plenum, New York. 1985;267-283.7 TANAKA H 1993, Thulesius O: Effect of temperature on finger arterypressure evaluated by volume clamp technique. Clinical Physiology, 1993;13(5): 535-45.8 WESSELING KH 1985, Settels JJ, van der Hoeven GMA, Nijboer JA, ButijnMWT, Dorlas JC: Effects of peripheral vasoconstriction on the measurementof blood pressure in a finger. Cardiovascular Research 1985; 19: 139-145.9 WESSELING KH 1995, de Wit B, van der Hoeven GMA, van Goudoever J,Settels J: Physiocal, calibrating finger vascular physiology for Finapres.Homeostasis 36, 1995; No 2-3: 67-82.
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong> <strong>Reference</strong> <strong>Guide</strong> 4310 WESSELING KH 1995b: A century of noninvasive arterial pressuremeasurement: from Marey to Peňáz and Finapres. Homeostasis 1995; 36: 50-66.11 WESSELING KH 1996: <strong>Finger</strong> arterial pressure measurement with Finapres.Zeitschrift fur Kardiologie, 1996; 85 Suppl 3:38-44.Waveform filtering and level correction12 BOS WJ 1996, van Goudoever J, van Montfrans GA, van den Meiracker, AH,Wesseling KH: Reconstruction of brachial artery pressure from noninvasivefinger pressure measurements. Circulation. 1996; 94(8):1870-5.13 GIZDULICH P 1996, Imholz BP, van den Meiracker AH, Parati G, WesselingKH: Finapres tracking of systolic pressure and baroreflex sensitivity improvedby waveform filtering. Journal of Hypertension, 1996; 14(2):243-50.14 GIZDULICH P 1997, Prentza A, Wesseling KH: Models of brachial to fingerpulse wave distortion and pressure decrement. Cardiovascular Research. 1997;33(3):698-705.Modelflow cardiac output method15 WESSELING KH 1993, Jansen JRC, Settels JJ, Schreuder JJ: Computation ofaortic flow from pressure in humans using a nonlinear, three-element model.Journal of Applied Physiology 1993; 74:2566-2573.16 HARMS MPM 1999, Wesseling KH, Pott F, Jenstrup M, van Goudoever J,Secher NH, van Lieshout JJ: Continuous stroke volume monitoring bymodeling flow from non-invasive measurement of arterial pressure in humansunder orthostatic stress. Clinical Science, 1999; 97:291—301.17 JELLEMA WT., Wesseling KH., Groeneveld AB., Stoutenbeek CP., ThijsLG., van Lieshout JJ: Continuous cardiac output in septic shock by simulatinga model of the aortic input impedance: a comparison with bolus injectionthermodilution. Anesthesiology. 90(5):1317-28, 1999 May.Clinical experience
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong> <strong>Reference</strong> <strong>Guide</strong> 4418 BARDOCZKY GI 1992, Levarlet M, Engelman E, d'Hollander A, SchmartzD: Continuous noninvasive blood pressure monitoring during thoracic surgery.Journal of Cardiothoracic & Vascular Anesthesia, 1992; 6(1):51-4.19 BOS WJ 1992: Imholz BP, van Goudoever J, Wesseling KH, van MontfransGA: The reliability of noninvasive continuous finger blood pressuremeasurement in patients with both hypertension and vascular disease,American Journal of Hypertension, 1992; 5(8):529-35.20 BOS WJ 1995, van den Meiracker AH, Wesseling KH, Schalekamp MA:Effect of regional and systemic changes in vasomotor tone on finger pressureamplification. Hypertension, 1995; 26(2):315-20.21 BLUM V 1997, Carriere EG, Kolsters W, Mosterd WL, Schiereck P,Wesseling KH: Aortic and peripheral blood pressure during isometric anddynamic exercise. International Journal of Sports Medicine. 1997; 18(1):30-4.22 CASTIGLIONI P 1999, Parati G, Omboni S, Mancia G, Imholz BP,Wesseling KH, Di Rienzo M: Broad-band spectral analysis of 24 h continuousfinger blood pressure: comparison with intra-arterial recordings. ClinicalScience. 1999; 97(2):129-39.23 DORLAS JC 1985, Nijboer JA, Butijn WT, van der Hoeven GM, Settels JJ,Wesseling KH: Effects of peripheral vasoconstriction on the blood pressure inthe finger, measured continuously by a new noninvasive method (theFinapres). Anesthesiology, 1985; 62(3):342-5.24 DROUIN E 1997, Gournay V, Calamel J, Mouzard A, Roze JC: Feasibility ofusing finger arterial pressure in neonates. Archives of Disease in ChildhoodFetal & Neonatal Edition, 1997; 77(2):F139-40, 1997.25 EPSTEIN RH 1991, Bartkowski RR, Huffnagle S: Continuous noninvasivefinger blood pressure during controlled hypotension, A comparison withintraarterial pressure. Anesthesiology, 1991; 75(5):796-803.26 GRAVENSTEIN JS 1985, Paulus DA, Feldman J, McLaughlin G: Tissuehypoxia distal to a Peñáz finger blood pressure cuff. Journal of ClinicalMonitoring 1985; 1, 120-125.27 HIRSCHL MM 1996, Binder M, Herkner H, Bur A, Brunner M, Seidler D,Stuhlinger HG, Laggner AN: Accuracy and reliability of noninvasive
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong> <strong>Reference</strong> <strong>Guide</strong> 45continuous finger blood pressure measurement in critically ill patients. CriticalCare Medicine, 1996; 24(10):1684-9.28 IDEMA RN 1989, van den Meiracker AH, Imholz BP, Man in 't Veld AJ,Settels JJ, Ritsema van Eck HJ, Schalekamp MA: Comparison of Finapresnon-invasive beat-to-beat finger blood pressure with intrabrachial arterypressure during and after bicycle ergometry. Journal of Hypertension –Supplement. 1989; 7(6):S58-9, 1989.29 IMHOLZ BP 1988, van Montfrans GA, Settels JJ, van der Hoeven GM,Karemaker JM, Wieling W: Continuous non-invasive blood pressuremonitoring: reliability of Finapres device during the Valsalva manoeuvre.Cardiovascular Research. 1988; 22(6):390-7.30 IMHOLZ BP 1991, Wieling W, Langewouters GJ, van Montfrans GA:Continuous finger arterial pressure: utility in the cardiovascular laboratory.Clinical Autonomic Research, 1991; 1(1):43-53.31 IMHOLZ BP 1992, Parati G, Mancia G, Wesseling KH: Effects of gradedvasoconstriction upon the measurement of finger arterial pressure. Journal ofHypertension 1992; 10(9):979-84.32 IMHOLZ BP 1996: Automated blood pressure measurement duringergometric stress testing: possibilities of Finapres. Zeitschrift fur Kardiologie,1996; 85 Suppl 3:76-80.33 JAGOMAGI K 1996, Talts J, Raamat R, Lansimies E: Continuous noninvasivemeasurement of mean blood pressure in fingers by volume-clamp anddifferential oscillometric method. Clinical Physiology, 1996; 16(5):551-60.34 JELLEMA WT 1996, Imholz BP, van Goudoever J, Wesseling KH, vanLieshout JJ: <strong>Finger</strong> arterial versus intrabrachial pressure and continuouscardiac output during head-up tilt testing in healthy subjects. Clinical Science,1996; 91(2):193-200.35 DE JONG-DE VOS VAN STEENWIJK CC 1997, Wieling W, Harms MP,Wesseling KH: Variability of near-fainting responses in healthy 6-16-year-oldsubjects. Clinical Science, 1997; 93(3):205-11.36 LINDQVIST A 1995: Beat-to-beat agreement of non-invasive finger arteryand invasive radial artery blood pressure in hypertensive patients takingcardiovascular medication. Clinical Physiology, 1995; 15(3):219-29.
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong> <strong>Reference</strong> <strong>Guide</strong> 4637 MAREY EJ 1878: La méthode graphique dans les sciences expérimentales etprincipalement en physiologie et en médicine. Masson 1878 Paris.38 NIJBOER JA 1988, Dorlas JC, Lubbers J: The difference in blood pressurebetween upper arm and finger during physical exercise. Clinical Physiology,1988; 8(5):501-10.39 OMBONI S 1995, Smit AA, Wieling W: Twenty four hour continuous noninvasivefinger blood pressure monitoring: a novel approach to the evaluationof treatment in patients with autonomic failure. British Heart Journal, 1995;73(3):290-2.40 OMBONI S 1998, Parati G, Castiglioni P, Di Rienzo M, Imholz BP,Langewouters, GJ, Wesseling KH, Mancia G: Estimation of blood pressurevariability from 24-hour ambulatory finger blood pressure. Hypertension,1998; 32(1):52-8.41 PARATI G 1989, Casadei R, Groppelli A, Di Rienzo M, Mancia G:Comparison of finger and intra-arterial blood pressure monitoring at rest andduring laboratory testing. Hypertension, 1989; 13(6 Pt 1):647-55.42 PENZEL T 1992, Mayer J, Peter JH, Podszus T, Voigt KH, von Wichert P:Continuous non-invasive blood pressure monitoring in patients with sleepdisorders. Physiological Research, 1992; 41(1):11-7.43 PETERSEN ME 1995, Williams TR, Sutton R: A comparison of non-invasivecontinuous finger blood pressure measurement (Finapres) with intra-arterialpressure during prolonged head-up tilt. European Heart Journal 1995;16(11):1641-54.44 PORTER KB 1991, O'Brien WF, Kiefert V, Knuppel RA: Finapres: anoninvasive device to monitor blood pressure. Obstetrics & Gynecology, 78(3Pt 1):430-3, 1991.45 RONGEN GA 1995, Bos WJ, Lenders JW, van Montfrans GA, van Lier HJ,van Goudoever J, Wesseling KH, Thien T, Comparison of intrabrachial andfinger blood pressure in healthy elderly volunteers. American Journal ofHypertension, 1995; 8(3):237-48.46 SCHMIDT TF 1992, Wittenhaus J, Steinmetz TF, Piccolo P, Lupsen H,Twenty-four-hour ambulatory noninvasive continuous finger blood pressure
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong> <strong>Reference</strong> <strong>Guide</strong> 47measurement with PORTAPRES: a new tool in cardiovascular research.Journal of Cardiovascular Pharmacology, 1992; 19 Suppl 6:S117-45.47 TANAKA H 1994, Thulesius O, Yamaguchi H, Mino M: Circulatoryresponses in children with unexplained syncope evaluated by continuous noninvasivefinger blood pressure monitoring, Acta Paediatrica, 1994; 83(7):754-61.48 TANAKA H 1994, Thulesius O, Yamaguchi H, Mino M, Konishi K:Continuous non-invasive finger blood pressure monitoring in children. ActaPaediatrica, 1994; 83(6):646-52.49 VEERMAN DP 1994, Imholz BP, Wieling W, Karemaker JM, van MontfransGA: Effects of aging on blood pressure variability in resting conditions.Hypertension, 1994; 24(1):120-30.50 VOOGEL AJ 1997a, Bos WJW, van Goudoever J, van Montfrans GA,Wesseling KH: <strong>Finger</strong>-to-brachial comparability of 'Modelflow' stroke volumeimproves after pulsewave reconstruction. Clinical Physiology 1997; 17: 327-337.51 VOOGEL AJ 1997b, Stok WJ, Pretorius PJ, Van Montfrans GA,Langewouters GJ, Karemaker JM: Circadian blood pressure and systemichemodynamics during 42 days of 6 degrees head-down tilt. Acta PhysiologicaScandinavica, 1997; 161(1):71-80.52 VOOGEL AJ 1997c, van Montfrans GA: Reproducibility of twenty-four-hourfinger arterial blood pressure, variability and systemic hemodynamics. Journalof Hypertension, 1997; 15:1761-5.53 VOOGEL AJ 1999, van Steenwijk RP, Karemaker JM, van Montfrans GA:Effects of treatment of obstructive sleep apnea on circadian hemodynamics.Journal of the Autonomic Nervous System 1999; 77: 177-183.
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong> <strong>Reference</strong> <strong>Guide</strong> 48INDEXAAC-plethysmogram, 11Arterial diameter, 12BBeatScope, 29Bias and precision, 26Blue fingers, 20Brachial artery, 9, 24, 28Clinical use, 27Compliance, 12, 15Contacting <strong>TNO</strong>, 9Copyright, 3Cuff, 10Cuff size, 31Cuff wrapping, 32CDDC-plethysmogram, 11Diagnostic, 38Diameter, 12FFinapres, 8, 10<strong>Finger</strong> arterial blood pressure, 22<strong>Finger</strong> cuffs, 10<strong>Finger</strong> switching, 21, 34Finometer, 7, 8Flash Memory Card, 8Frontend unit, 11HHeight correction, 8, 35Infrared, 10ILLED, 11Level correction, 28MMeasurement stability, 39Modelflow, 9, 30Multi-step Physiocal, 17NNormal Physiocal, 16Ohmeda Finapres, 8Oscillations, 39OPPeaked waveforms, 40Peñáz, 10, 14Photo-plethysmograph, 10Physiocal, 15, 18, 39Physiocal frequency, 20, 39Plethysmogram, 11, 15Plethysmograph, 11, 13Portapres, 7, 8Control unit, 8<strong>Pressure</strong>-diameter relationship, 12Proportional valve, 14Pulse wave, 24
<strong>TNO</strong> <strong>Finger</strong> <strong>Pressure</strong> <strong>Reference</strong> <strong>Guide</strong> 49R<strong>Reference</strong>s, 42Related Publications, 7SServo controller, 10, 13Smooth muscle tone, 16Staircase, 19Start-up, 19TTrademarks, 3Transmural pressure, 12UUnloaded diameter, 13, 15, 19VV:, 11V=, 11Vaso-constriction, 38, 41Volume-clamp method, 10WWaveform filtering, 27Wesseling, 15WWW site, 9