Original article - Ethiopian Review
Original article - Ethiopian Review
Original article - Ethiopian Review
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
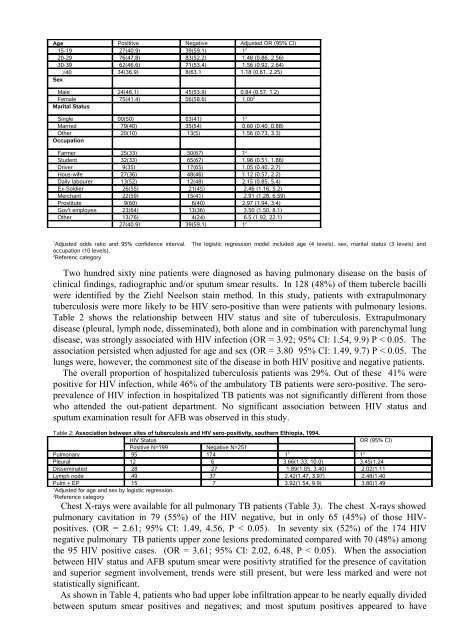
Age Posititve Negative Adjusted OR (95% CI)15-19 27(40.9) 39(59.1) 1 220-29 76(47.8) 83(52.2) 1.48 (0.86, 2.56)30-39 62(46.6) 71(53.4) 1.56 (0.92, 2.64)≥40 34(36.9) 8(63.1 1.18 (0.61, 2.25)SexMale 24(46.1) 45(53.9) 0.84 (0.57, 1.2)Female 75(41.4) 06(58.6) 1.00 2Marital StatusSingle 00(50) 03(41) 1 2Married 79(40) 35(54) 0.60 (0.40, 0.88)Other 20(10) 13(5) 1.56 (0.73, 3.3)OccupationFarmer 25(33) 50(67) 1 2Student 32(33) 65(67) 1.98 (0.51, 1.86)Driver 9(35) 17(65) 1.05 (0.40, 2.7)Hous-wife 27(36) 48(46) 1.12 (0.57, 2.2)Daily labourer 13(52) 12(48) 2.15 (0.85, 5.4)Ex-Soldier 26(55) 21(45) 2.46 (1.16, 5.2)Merchant 22(59) 15(41) 2.91 (1.28, 6.59)Prostitute 9(60) 6(40) 2.97 (1.94, 3.4)Gov’t employee 23(64) 13(36) 3.50 (1.50, 8.1)Other 13(76) 4(24) 6.5 (1.92, 22.1)27(40.9) 39(59.1) 1 21Adjusted odds ratio and 95% confidence interval. The logistic regression model included age (4 levels), sex, marital status (3 levels) andoccupation (10 levels).2Referenc categoryTwo hundred sixty nine patients were diagnosed as having pulmonary disease on the basis ofclinical findings, radiographic and/or sputum smear results. In 128 (48%) of them tubercle bacilliwere identified by the Ziehl Neelson stain method. In this study, patients with extrapulmonarytuberculosis were more likely to be HIV sero-positive than were patients with pulmonary lesions.Table 2 shows the relationship between HIV status and site of tuberculosis. Extrapulmonarydisease (pleural, lymph node, disseminated), both alone and in combination with parenchymal lungdisease, was strongly associated with HIV infection (OR = 3.92; 95% CI: 1.54, 9.9) P < 0.05. Theassociation persisted when adjusted for age and sex (OR = 3.80 95% CI: 1.49, 9.7) P < 0.05. Thelungs were, however, the commonest site of the disease in both HIV positive and negative patients.The overall proportion of hospitalized tuberculosis patients was 29%. Out of these 41% werepositive for HIV infection, while 46% of the ambulatory TB patients were sero-positive. The seroprevalenceof HIV infection in hospitalized TB patients was not significantly different from thosewho attended the out-patient department. No significant association between HIV status andsputum examination result for AFB was observed in this study.Table 2: Association between sites of tuberculosis and HIV sero-positivity, southern Ethiopia, 1994.HIV StatusOR (95% CI)Positive N=199 Negative N=251Pulmonary 95 174 1 1 1 2Pleural 12 6 3.66(1.33, 10.0) 3.45(1.24Disseminated 28 27 1.89(1.05, 3.40) 2.02(1.11Lymph node 49 37 2.42(1.47, 3.97) 2.48(1.40Pulm + EP 15 7 3.92(1.54, 9.9) 3.80)1.491Adjusted for age and sex by logistic regression.2Reference categoryChest X-rays were available for all pulmonary TB patients (Table 3). The chest X-rays showedpulmonary cavitation in 79 (55%) of the HIV negative, but in only 65 (45%) of those HIVpositives.(OR = 2.61; 95% CI: 1.49, 4.56, P < 0.05). In seventy six (52%) of the 174 HIVnegative pulmonary TB patients upper zone lesions predominated compared with 70 (48%) amongthe 95 HIV positive cases. (OR = 3.61; 95% CI: 2.02, 6.48, P < 0.05). When the associationbetween HIV status and AFB sputum smear were positivty stratified for the presence of cavitationand superior segment involvement, trends were still present, but were less marked and were notstatistically significant.As shown in Table 4, patients who had upper lobe infiltration appear to be nearly equally dividedbetween sputum smear positives and negatives; and most sputum positives appeared to have
![to read the full report [pdf, Amharic] - Ethiopian Review](https://img.yumpu.com/52737829/1/190x245/to-read-the-full-report-pdf-amharic-ethiopian-review.jpg?quality=85)