

images
1TEZSjF
1TEZSjF

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
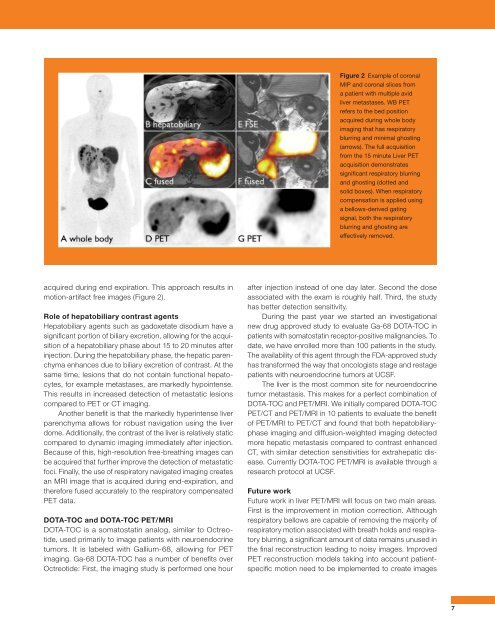
Figure 2 Example of coronal<br />
MIP and coronal slices from<br />
a patient with multiple avid<br />
liver metastases. WB PET<br />
refers to the bed position<br />
acquired during whole body<br />
imaging that has respiratory<br />
blurring and minimal ghosting<br />
(arrows). The full acquisition<br />
from the 15 minute Liver PET<br />
acquisition demonstrates<br />
significant respiratory blurring<br />
and ghosting (dotted and<br />
solid boxes). When respiratory<br />
compensation is applied using<br />
a bellows-derived gating<br />
signal, both the respiratory<br />
blurring and ghosting are<br />
effectively removed.<br />
acquired during end expiration. This approach results in<br />
motion-artifact free <strong>images</strong> (Figure 2).<br />
Role of hepatobiliary contrast agents<br />
Hepatobiliary agents such as gadoxetate disodium have a<br />
significant portion of biliary excretion, allowing for the acquisition<br />
of a hepatobiliary phase about 15 to 20 minutes after<br />
injection. During the hepatobiliary phase, the hepatic parenchyma<br />
enhances due to biliary excretion of contrast. At the<br />
same time, lesions that do not contain functional hepatocytes,<br />
for example metastases, are markedly hypointense.<br />
This results in increased detection of metastatic lesions<br />
compared to PET or CT imaging.<br />
Another benefit is that the markedly hyperintense liver<br />
parenchyma allows for robust navigation using the liver<br />
dome. Additionally, the contrast of the liver is relatively static<br />
compared to dynamic imaging immediately after injection.<br />
Because of this, high-resolution free-breathing <strong>images</strong> can<br />
be acquired that further improve the detection of metastatic<br />
foci. Finally, the use of respiratory navigated imaging creates<br />
an MRI image that is acquired during end-expiration, and<br />
therefore fused accurately to the respiratory compensated<br />
PET data.<br />
DOTA-TOC and DOTA-TOC PET/MRI<br />
DOTA-TOC is a somatostatin analog, similar to Octreotide,<br />
used primarily to image patients with neuroendocrine<br />
tumors. It is labeled with Gallium-68, allowing for PET<br />
imaging. Ga-68 DOTA-TOC has a number of benefits over<br />
Octreotide: First, the imaging study is performed one hour<br />
after injection instead of one day later. Second the dose<br />
associated with the exam is roughly half. Third, the study<br />
has better detection sensitivity.<br />
During the past year we started an investigational<br />
new drug approved study to evaluate Ga-68 DOTA-TOC in<br />
patients with somatostatin receptor-positive malignancies. To<br />
date, we have enrolled more than 100 patients in the study.<br />
The availability of this agent through the FDA-approved study<br />
has transformed the way that oncologists stage and restage<br />
patients with neuroendocrine tumors at UCSF.<br />
The liver is the most common site for neuroendocrine<br />
tumor metastasis. This makes for a perfect combination of<br />
DOTA-TOC and PET/MRI. We initially compared DOTA-TOC<br />
PET/CT and PET/MRI in 10 patients to evaluate the benefit<br />
of PET/MRI to PET/CT and found that both hepatobiliaryphase<br />
imaging and diffusion-weighted imaging detected<br />
more hepatic metastasis compared to contrast enhanced<br />
CT, with similar detection sensitivities for extrahepatic disease.<br />
Currently DOTA-TOC PET/MRI is available through a<br />
research protocol at UCSF.<br />
Future work<br />
Future work in liver PET/MRI will focus on two main areas.<br />
First is the improvement in motion correction. Although<br />
respiratory bellows are capable of removing the majority of<br />
respiratory motion associated with breath holds and respiratory<br />
blurring, a significant amount of data remains unused in<br />
the final reconstruction leading to noisy <strong>images</strong>. Improved<br />
PET reconstruction models taking into account patientspecific<br />
motion need to be implemented to create <strong>images</strong><br />
7