

Nov 2016

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
with<br />
Prof Charles McGhee<br />
& A/Prof Dipika Patel<br />
Series Editors<br />
Age-related macular<br />
degeneration: update<br />
Background<br />
Age-related macular degeneration (AMD) is the<br />
leading cause of blindness or severe irreversible<br />
visual impairment in people over 50, in the<br />
developed world. As of 2009, 49% of the current<br />
blind foundation registrations in New Zealand<br />
were for AMD 1 . The incidence, prevalence and<br />
progression of AMD increases with age and<br />
varies by ethnicity. In the Beaver Dam Eye<br />
Study, a primarily Caucasian population, the<br />
prevalence of AMD was 10% in individuals aged<br />
55 to 64 year rising to 46% for those aged ≥<br />
75 2 . The prevalence of AMD in Asians over 55 is<br />
estimated 6.8% 3 . AMD is comparatively rare in<br />
the Asian subcontinent and Hispanic populations<br />
and is virtually unknown in African, Maori and<br />
Polynesian populations. The subtype of AMD<br />
that is seen clearly differs between ethnicities.<br />
Whilst classical AMD is seen most commonly in<br />
Causasians, polypoidal choriovasculopathy (PCV)<br />
is the commonest type of AMD seen in Asians. In<br />
2014, the prevalence of AMD in New Zealanders<br />
aged 45-85 year age group was estimated to<br />
be 184,000, numbers which are projected to<br />
increase markedly to 208,200 by 2026 4 . With the<br />
impending demographic shift towards an aging<br />
population, AMD represents a significant and<br />
increasing burden on the health care provision in<br />
New Zealand in the coming years.<br />
Risk Factors and pathophysiology<br />
It has long been recognised that the likelihood of<br />
an individual developing AMD is the result of a<br />
complex interplay of genetic and environmental<br />
risk factors; factors which are probably<br />
cumulative with respect to the risk of developing<br />
the disease. Whilst the genetics of AMD are<br />
beyond the scope of this article it is clear that<br />
certain genetic anomalies carry a significant<br />
risk for affected individuals, the classic example<br />
being complement factor H polymorphisms.<br />
Gene products for CFH play an important role<br />
in the regulation of the host immune system<br />
and individuals who carry a CFH polymorphism<br />
therefore posses a dysfunctional and “over active”<br />
immune system. This risk is not insignificant, for<br />
example individuals who are homozygous for<br />
the Y420H risk allele of CFH are known to be 7x<br />
more likely to develop AMD compared to normal<br />
controls. These results suggest that inflammation,<br />
plays a significant although as yet ill understood<br />
role in the development of AMD. Apart from age,<br />
ethnicity and genetics – strong non-modifiable<br />
risk factors – numerous studies have identified<br />
cigarette smoking to increase the risk of<br />
developing AMD. Smoking significantly increases<br />
AMD risk in a dose response relationship with<br />
the relative risk increasing in proportion to<br />
the number of pack years 5 . Smoking cessation<br />
reduces the risk of progression and thus smoking<br />
cessation remains the single most effective<br />
population intervention to reduce the burden<br />
that AMD represents.<br />
The conventional hypothesis for the<br />
development of AMD holds that the primary<br />
event in the development of AMD is dysfunction<br />
of the RPE, with build-up of drusen, RPE<br />
atrophy, ischaemia of the outer retina and<br />
ultimately the production of VEGF and subretinal<br />
neovascularization. However this conventional<br />
hypothesis ignores the role of the choroid and in<br />
particular the role that the choriocapillaris plays<br />
in the maintenance of the Bruchs/ RPE complex<br />
and the outer retina. What is now clear is that<br />
irrespective of the mechanism a thin choroid, and<br />
in particular a thin inner choroid is a significant<br />
risk factor for the development of “classical” AMD.<br />
How “risk” CFH polymorphisms and smoking fits<br />
into this story remains a matter of conjecture<br />
but it is highly likely that inflammation plays<br />
a key role in the loss of the choroicapillaris.<br />
Whether this is the primary event, or the end<br />
game of AMD needs further study but the answer<br />
to this question has huge implications for the<br />
development of new therapeutic targets in both<br />
dry and wet AMD.<br />
DAVID SQUIRRELL AND PAVANI KURRA*<br />
Classification and natural history<br />
Most readers will be familiar with the classification<br />
of AMD and recognise that AMD encompasses<br />
a wide spectrum of disease. Dry AMD is<br />
characterised by the presence of one or more of<br />
the following: presence of at least intermediate<br />
size drusen (63 microns or larger in diameter),<br />
retinal pigment epithelium (RPE) abnormalities,<br />
reticular pseudodrusen and/or of geographical<br />
-atrophy (GA) of RPE. Wet AMD is characterised<br />
by the development of subretinal and intraretinal<br />
neovascularisation. Soft drusen and pigmentary<br />
abnormalities increase with age and strongly<br />
predict progression towards advanced AMD.<br />
The risk of progression of AMD also seems<br />
to accelerate the more advanced the disease<br />
becomes. Whilst approximately 15% of patients<br />
with early AMD developed large drusen at 10<br />
years the risk of advanced AMD developing over<br />
this time period was low. However if a patient has<br />
Intermediate AMD the five year risk of developing<br />
advanced AMD increases steeply to near 20%. It<br />
is also noteworthy that patients with reticular<br />
pseudodrusen have a particularly high propensity<br />
to develop advanced AMD. The risk of a patient<br />
who has advanced AMD in one eye, developing<br />
advanced AMD in the other eye is approximately<br />
50% at five years. In all cases the risk of progression<br />
to advanced AMD, is inversely associated with<br />
choroidal thickness.<br />
Prevention<br />
By far and away the single most effective<br />
preventative strategy for the development of<br />
advanced AMD is to stop smoking. The large and<br />
hugely influential AREDS studies demonstrated<br />
that antioxidant supplements may slow the<br />
progression of moderate AMD (soft drusen<br />
and pigmentary changes) to wet AMD but the<br />
therapeutic effects are sometimes overstated.<br />
Although the relative risk reduction for patients<br />
taking antioxidant supplements was around 25%<br />
in real terms the more important absolute risk<br />
reduction was smaller at around 8%. There have<br />
also been concerns raised by some that, in a small<br />
sub-set of patients, antioxidant supplements may<br />
actually accelerate AMD. However, generally one<br />
would still advocate antioxidant supplements in<br />
all patients with moderate AMD. There is currently<br />
no evidence to suggest AREDS supplements help in<br />
halting progression of dry AMD.<br />
The reported ability of lutein, xeothanine and<br />
mesoxanthine supplementation to increase the<br />
density of macular pigments is interesting and<br />
the results emerging from the clinical trials with<br />
subjects on these supplements report better<br />
subjective and objective measures of visual<br />
functioning compared to controls. However<br />
whether such interventions actually reduce the<br />
risk of the development of AMD remains uncertain<br />
and at the present time one can only say that their<br />
role is unknown.<br />
The drug treatment of dry AMD remains an<br />
exciting area of research with a number of<br />
neuroprotective and inflammatory modulating<br />
agents the subject of large clinical trials. The<br />
technologies underpinning stem cell transplants<br />
also continue to improve and show great promise,<br />
but at the time of writing the drug treatment of<br />
dry AMD remains a story of unfulfilled promises.<br />
Wet AMD treatment<br />
It is perhaps not too much of an exaggeration to say<br />
that the use of antiVEGF agents in ophthalmology<br />
has been one of the single greatest advances in<br />
modern medicine. Certainly the advent of the<br />
antiVEGF era has transformed the outcome of<br />
wet AMD with the improvement in visual acuity<br />
observed in the key note ANCHOR and MARINA<br />
trials extending out to five years and beyond 6,7 . The<br />
question of which antiVEGF agent to use (Avastin,<br />
Lucentis or Eylea) remains the subject of debate<br />
and the choice of which drug is used in which<br />
country may have as much to do with politics and<br />
economics as it does evidence. The key note trials<br />
demonstrated that regardless of the drug used,<br />
most patients with classical<br />
wet AMD did well and,<br />
at a population level at<br />
least, there was little to<br />
choose between the agents.<br />
However as always there<br />
are nuances; not every<br />
patient responds equally<br />
well to each drug and the<br />
treating clinician needs<br />
to be prepared to switch<br />
drugs early if the agent used<br />
proves to be ineffective. One<br />
exception is that Aflibercept<br />
is more effective than the<br />
other two agents at treating<br />
patients who have the PCV<br />
variant of AMD. Currently in<br />
New Zealand avastin is the<br />
first line treatment for wet<br />
AMD, Lucentis being the<br />
funded second line agent.<br />
In <strong>Nov</strong>ember, Pharmac will<br />
announce the results of<br />
their long-awaited review<br />
of antiVEGF agents and it<br />
is anticipated that they will<br />
add Eylea to this list. The<br />
drug treatment of wet AMD<br />
continues to evolve at a fast<br />
pace and whilst it is not<br />
possible to “pick a winner”<br />
at this time, what is certain<br />
is that new, longer-acting<br />
treatments will enter the<br />
market over the coming<br />
years.<br />
Putting the excitement of<br />
emerging drug treatments<br />
to one side, currently the<br />
greatest challenge for<br />
clinicians, particularly<br />
those in the public sector,<br />
is to provide the treatment<br />
patients need. Despite<br />
innervations such as<br />
utilising trained nursing<br />
staff to deliver injections,<br />
most public eye clinics are<br />
struggling to provide the<br />
treatments their patients need. In Auckland alone,<br />
we are now providing about 20,000 appointments<br />
annually to treat wAMD, a growth in demand that<br />
has not been matched by increased resources. It is<br />
widely accepted that under treatment of wet AMD<br />
is associated with worse outcomes and MDNZ and<br />
others continue to lobby central government and<br />
local DHBs for more resources.<br />
In summary the outlook for our patients with AMD<br />
has never looked better. Challenges do however<br />
remain. Early detection and treatment is crucial and<br />
MDNZ and others continue to work hard raising<br />
awareness of AMD. Once diagnosed patients,<br />
optometrists and general practitioners need an easily<br />
accessible “fast track” referral process to ensure<br />
treatment is delivered promptly. The availability of<br />
these “fast track” services are patchy and patients<br />
often have to rely on the private sector in the first<br />
instance to get prompt treatment. Thereafter, eye<br />
clinics need the resource to provide capacity for the<br />
ongoing review and treatment of what is a chronic<br />
disease. Our score card for the management of wet<br />
AMD in New Zealand remains “heading in the right<br />
direction, but could do better” ▀<br />
About the authors<br />
* Dr David Squirrell<br />
David is a specialist whose primary interest is medical retina<br />
and AMD. David has severed as the principle investigator for<br />
numerous studies in AMD, including the key note IVAN trial.<br />
David works at Greenlane Clinical centre and Milford Eye clinic<br />
Auckland.<br />
* Dr Pavani Kurra<br />
Pavani is currently working as a junior clinical fellow<br />
in medical retina at the University of Auckland and<br />
Greenlane Clinical Centre. She also spent time undertaking<br />
ophthalmology electives at L. V. Prasad Eye Institute and in<br />
Alice Springs prior to her fellowship in New Zealand.<br />
Fig 1. (a) Colour photograph, (b) fluorescein angiogram and (c) OCT of patient with classic wet AMD.<br />
Fig 2. (a) Colour photograph, (b) infrared image and (c) OCT of a patient with reticulo-pseudodrusen.<br />
Note there are very few drusen seen on fundoscopy but marked changes are seen on the infrared<br />
image. The OCT image is characteristic with focal subretinal protrusions and a thin choroid<br />
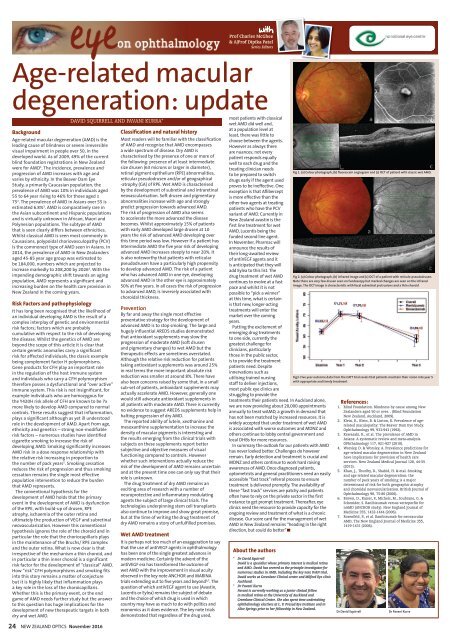
Fig3. Five year outcome data from the CATT trial revels that patients maintain their vision into year 5<br />
with appropriate and timely treatment<br />
References:<br />
1. Blind Foundation. Blindness by cause among New<br />
Zealanders aged 50 or over. . (Blind Foundation<br />
New Zealand, Auckland, 2009).<br />
2. Klein, R., Klein, B. & Linton, K. Prevalence of agerelated<br />
maculopathy: The Beaver Dam Eye Study.<br />
Ophthalmology 99, 933-943 (1992).<br />
3. Kawasaki, R., et al. The prevalence of AMD in<br />
Asians: A systematic review and meta-analysis.<br />
OPhthalmology 117, 921-927 (2010).<br />
4. Worsley, D. & Worsley, A. Prevalence predictions for<br />
age-related macular degeneration in New Zealand<br />
have implications for provision of health care<br />
services. New Zealand Medical Journal 128, 44-55<br />
(2015).<br />
5. Khan, J., Thurlby, D., Shahid, H. & etal. Smoking<br />
and age related macular degeneration: the<br />
number of pack years of smoking is a major<br />
determinant of risk for both geographic atrophy<br />
and choroidal neovascularisation. British Journal of<br />
Ophthalmology 90, 75-80 (2006).<br />
6. Brown, D., Kaiser, P., Michels, M., Soubrane, G. &<br />
Schenider, S. Ranibizumab versus verteporfin for<br />
nAMD (ANCHOR study). New England Journal of<br />
Medicine 355, 1432-1444 (2006).<br />
7. Rosenfeld, P., et al. Ranibizumab for neovascular<br />
AMD. The New England Journal of Medicine 355,<br />
1419-1431 (2006).<br />
Dr David Squirrell<br />
Dr Pavani Kurra<br />
24 NEW ZEALAND OPTICS <strong>Nov</strong>ember <strong>2016</strong>













