
You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
The neuromuscular system<br />
Section 2<br />
To summarise:<br />
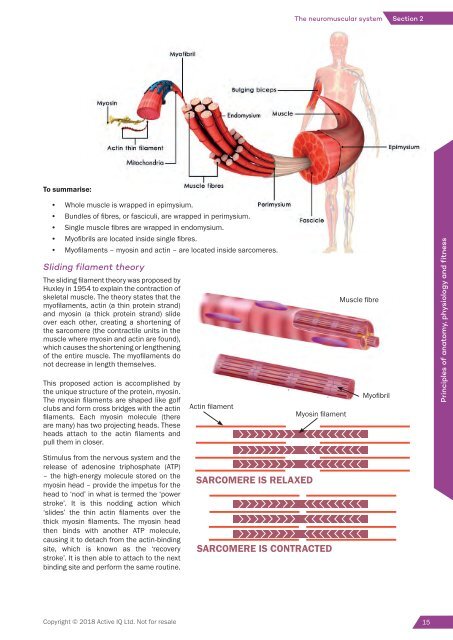
• Whole muscle is wrapped <strong>in</strong> epimysium.<br />
• Bundles of fibres, or fasciculi, are wrapped <strong>in</strong> perimysium.<br />
• S<strong>in</strong>gle muscle fibres are wrapped <strong>in</strong> endomysium.<br />
• Myofibrils are located <strong>in</strong>side s<strong>in</strong>gle fibres.<br />
• Myofilaments – myos<strong>in</strong> <strong>and</strong> act<strong>in</strong> ‒ are located <strong>in</strong>side sarcomeres.<br />
Slid<strong>in</strong>g filament theory<br />
The slid<strong>in</strong>g filament theory was proposed by<br />
Huxley <strong>in</strong> 1954 to expla<strong>in</strong> the contraction of<br />
skeletal muscle. The theory states that the<br />
myofilaments, act<strong>in</strong> (a th<strong>in</strong> prote<strong>in</strong> str<strong>and</strong>)<br />
<strong>and</strong> myos<strong>in</strong> (a thick prote<strong>in</strong> str<strong>and</strong>) slide<br />
over each other, creat<strong>in</strong>g a shorten<strong>in</strong>g of<br />
the sarcomere (the contractile units <strong>in</strong> the<br />
muscle where myos<strong>in</strong> <strong>and</strong> act<strong>in</strong> are found),<br />
which causes the shorten<strong>in</strong>g or lengthen<strong>in</strong>g<br />
of the entire muscle. The myofilaments do<br />
not decrease <strong>in</strong> length themselves.<br />
This proposed action is accomplished by<br />
the unique structure of the prote<strong>in</strong>, myos<strong>in</strong>.<br />
The myos<strong>in</strong> filaments are shaped like golf<br />
clubs <strong>and</strong> form cross bridges with the act<strong>in</strong><br />
filaments. Each myos<strong>in</strong> molecule (there<br />
are many) has two project<strong>in</strong>g heads. These<br />
heads attach to the act<strong>in</strong> filaments <strong>and</strong><br />
pull them <strong>in</strong> closer.<br />
Act<strong>in</strong> filament<br />
Myos<strong>in</strong> filament<br />
Muscle fibre<br />
Myofibril<br />
Pr<strong>in</strong>ciples of anatomy, physiology <strong>and</strong> fitness<br />
Stimulus from the nervous system <strong>and</strong> the<br />
release of adenos<strong>in</strong>e triphosphate (ATP)<br />
– the high-energy molecule stored on the<br />
myos<strong>in</strong> head – provide the impetus for the<br />
head to ‘nod’ <strong>in</strong> what is termed the ‘power<br />
stroke’. It is this nodd<strong>in</strong>g action which<br />
‘slides’ the th<strong>in</strong> act<strong>in</strong> filaments over the<br />
thick myos<strong>in</strong> filaments. The myos<strong>in</strong> head<br />
then b<strong>in</strong>ds with another ATP molecule,<br />
caus<strong>in</strong>g it to detach from the act<strong>in</strong>-b<strong>in</strong>d<strong>in</strong>g<br />
site, which is known as the ‘recovery<br />
stroke’. It is then able to attach to the next<br />
b<strong>in</strong>d<strong>in</strong>g site <strong>and</strong> perform the same rout<strong>in</strong>e.<br />
SARCOMERE IS RELAXED<br />
SARCOMERE IS CONTRACTED<br />
Copyright © 2018 <strong>Active</strong> <strong>IQ</strong> Ltd. Not for resale 15
Nervous system anatomy<br />
Every system depends on other<br />
systems for optimal function<strong>in</strong>g.<br />
The body is a liv<strong>in</strong>g structure comprised of many<br />
fi nely <strong>in</strong>tegrated <strong>and</strong> <strong>in</strong>terconnected systems.<br />
Each system can be described <strong>in</strong>dependently <strong>and</strong><br />
separately, but it is important to remember that they<br />
are actually <strong>in</strong>terdependent.<br />
To give a very basic example of the <strong>in</strong>terconnection: the skeletal system of bones <strong>and</strong> jo<strong>in</strong>ts provides<br />
the framework; the muscles generate movement of the skeletal framework; the heart <strong>and</strong> circulatory<br />
system pump oxygen <strong>and</strong> nutrients to fuel the muscles; the respiratory system takes <strong>in</strong> oxygen<br />
<strong>and</strong> removes waste products; the nervous system is the control centre responsible for oversee<strong>in</strong>g<br />
<strong>and</strong> respond<strong>in</strong>g to all dem<strong>and</strong>s <strong>and</strong> actions; <strong>and</strong> the digestive system breaks down <strong>and</strong> stores the<br />
nutrients required for energy production.<br />
Skeletal anatomy<br />
Digestive anatomy<br />
Copyright © 2018 <strong>Active</strong> <strong>IQ</strong> Ltd. Not for resale
KEY LEGAL AND REGULATORY<br />
REQUIREMENTS<br />
Health <strong>and</strong> Safety at Work Act, 1974<br />
Report<strong>in</strong>g of Injuries, Diseases <strong>and</strong> Dangerous Occurrences<br />
Regulations, 2013 (RIDDOR)<br />
Control of Substances Hazardous to Health Regulations, 2002 (COSHH)<br />
Manual H<strong>and</strong>l<strong>in</strong>g Operations Regulations, 1992<br />
Health <strong>and</strong> Safety (First Aid) Regulations, 1981<br />
DUTY OF CARE<br />
FOR FITNESS<br />
PROFESSIONALS:<br />
<strong>Personal</strong> safety<br />
Client safety<br />
Environmental safety<br />
Equipment safety<br />
HOW A FITNESS<br />
PROFESSIONAL<br />
MAINTAINS SAFETY<br />
OF THE GYM:<br />
Supervision of the gym environment<br />
H<strong>and</strong>over<br />
Ma<strong>in</strong>tenance checks<br />
Follow<strong>in</strong>g Normal Operat<strong>in</strong>g Procedures<br />
Follow<strong>in</strong>g Emergency Action Plans<br />
Report<strong>in</strong>g of <strong>in</strong>cidents <strong>and</strong> accidents<br />
HAZARDS<br />
IN A FITNESS<br />
ENVIRONMENT:<br />
Facilities<br />
Equipment<br />
Work<strong>in</strong>g practices<br />
Clients<br />
Client behaviour<br />
Security<br />
Hygiene<br />
Copyright © 2018 <strong>Active</strong> <strong>IQ</strong> Ltd Not for resale
Healthy Eat<strong>in</strong>g <strong>and</strong> hydration<br />
Eatwell Guide<br />
Energy<br />
1046kJ<br />
250kcal<br />
13%<br />
Check the label on<br />
packaged foods<br />
Each serv<strong>in</strong>g (150g) conta<strong>in</strong>s<br />
Fat Saturates Sugars Salt<br />
3.0g 1.3g 34g 0.9g<br />
LOW LOW HIGH MED<br />
4%<br />
7%<br />
38%<br />
15%<br />
of an adult’s reference <strong>in</strong>take<br />
Typical values (as sold) per 100g: 697kJ/ 167kcal<br />
Choose foods lower<br />
<strong>in</strong> fat, salt <strong>and</strong> sugars<br />
Frozen<br />
peas<br />
Use the Eatwell Guide to help you get a balance of healthier <strong>and</strong> more susta<strong>in</strong>able food. It<br />
shows how much of what you eat overall should come from each food group.<br />
Fruit <strong>and</strong> vegetables<br />
Chopped<br />
tomatoes<br />
Eat at least 5 portions of a variety of fruit <strong>and</strong> vegetables every day<br />
Rais<strong>in</strong>s<br />
Eatwell Guide<br />
Lentils<br />
Potatoes<br />
Whole<br />
gra<strong>in</strong><br />
cereal<br />
Choose wholegra<strong>in</strong> or higher fibre versions with less added fat, salt <strong>and</strong> sugar<br />
Cous<br />
Cous<br />
Porridge<br />
Potatoes, bread, rice, pasta <strong>and</strong> other starchy carbohydrates<br />
Whole<br />
wheat<br />
pasta<br />
Bagels<br />
Rice<br />
6-8<br />
a day<br />
Water, lower fat<br />
milk, sugar-free<br />
dr<strong>in</strong>ks <strong>in</strong>clud<strong>in</strong>g<br />
tea <strong>and</strong> coffee all<br />
count.<br />
Limit fruit juice<br />
<strong>and</strong>/or smoothies<br />
to a total of<br />
150ml a day.<br />
Tuna<br />
Beans<br />
lower<br />
salt<br />
<strong>and</strong><br />
sugar<br />
s Low fat<br />
oft cheese<br />
Spaghetti<br />
Crisps<br />
Pla<strong>in</strong><br />
nut<br />
nuts<br />
Chick<br />
peas<br />
Lean<br />
m<strong>in</strong>ce<br />
Semi<br />
skimmed<br />
milk<br />
Soya<br />
dr<strong>in</strong>k<br />
Pla<strong>in</strong><br />
Low fat<br />
yoghurt<br />
Veg<br />
Oil<br />
Lower fat<br />
spread<br />
Sauce<br />
Eat less often <strong>and</strong><br />
<strong>in</strong> small amounts<br />
Beans, pulses, fish, eggs, meat <strong>and</strong> other prote<strong>in</strong>s<br />
Eat more beans <strong>and</strong> pulses, 2 portions of susta<strong>in</strong>ably<br />
sourced fish per week, one of which is oily. Eat less<br />
red <strong>and</strong> processed meat<br />
Dairy <strong>and</strong> alternatives<br />
Choose lower fat <strong>and</strong><br />
lower sugar options<br />
Per day 2000kcal<br />
Oil & spreads<br />
Choose unsaturated oils<br />
<strong>and</strong> use <strong>in</strong> small amounts<br />
2500kcal = ALL FOOD + ALL DRINKS<br />
Source: Public Health Engl<strong>and</strong> <strong>in</strong> association with the Welsh Government, Food St<strong>and</strong>ards Scotl<strong>and</strong> <strong>and</strong> the Food St<strong>and</strong>ards Agency <strong>in</strong> Northern Irel<strong>and</strong> © Crown copyright 2016<br />
CARBOHYDRATE<br />
ENERGY<br />
PROTEIN<br />
GROWTH AND REPAIR<br />
FAT<br />
ENERGY AND INSULATION<br />
FATS<br />
Oily fi sh<br />
Avocado<br />
Olive oil<br />
Healthy eat<strong>in</strong>g guidel<strong>in</strong>es<br />
Calorie <strong>in</strong>take<br />
MEN:<br />
2,500<br />
calories / day<br />
WOMEN:<br />
2,000<br />
calories / day<br />
Copyright © 2018 <strong>Active</strong> <strong>IQ</strong> Ltd Not for resale<br />
GOOD Base your meals on starchy carbohydrates<br />
•<br />
Eat lots of fruit <strong>and</strong> veg (at least 5<br />
portions per day)<br />
•<br />
Eat more fi sh – two portions, <strong>in</strong>clud<strong>in</strong>g<br />
1 portion of oily fi sh<br />
Cut down on saturated fat <strong>and</strong> sugar<br />
•<br />
Eat less salt – no more than 6g a day for<br />
adults<br />
Get active <strong>and</strong> be a healthy weight<br />
•<br />
Ma<strong>in</strong>ta<strong>in</strong> healthy hydration levels<br />
(dr<strong>in</strong>k 6–8 glasses o f water every day)<br />
•<br />
Don’t skip breakfast<br />
BAD FATS<br />
Pumpk<strong>in</strong> seeds<br />
Red meat<br />
Cheese<br />
Cream<br />
Crisps
Section 1<br />
Underst<strong>and</strong><strong>in</strong>g how to plan gym-based exercise<br />
Body weight exercises<br />
PRESS-UP<br />
Start<br />
F<strong>in</strong>ish<br />
Muscles worked<br />
• Pectoralis.<br />
• Triceps brachii.<br />
• Deltoids (anterior).<br />
Teach<strong>in</strong>g po<strong>in</strong>ts<br />
• Prone position with arms extended <strong>and</strong><br />
feet <strong>in</strong> contact with floor.<br />
• Body aligned; head, shoulder, hip, knee<br />
<strong>and</strong> ankle.<br />
• Neutral sp<strong>in</strong>e <strong>and</strong> abdom<strong>in</strong>als<br />
engaged.<br />
• Bend the elbows to lower chest<br />
towards floor.<br />
• Extend elbows to return to start<br />
position.<br />
• Elbows unlocked.<br />
• Repeat for desired repetitions.<br />
Options<br />
• Box position with knees under hips.<br />
• Three-quarter position on thighs.<br />
• Perform aga<strong>in</strong>st a wall (across gravity).<br />
CHIN-UP – PRONATED GRIP, JUST WIDER THAN SHOULDER WIDTH.<br />
PULL-UP – SUPINATED GRIP, SHOULDER WIDTH.<br />
Start Start Teach<strong>in</strong>g po<strong>in</strong>ts<br />
F<strong>in</strong>ish<br />
F<strong>in</strong>ish<br />
• Grip bar us<strong>in</strong>g relevant h<strong>and</strong><br />
position.<br />
• Feet crossed.<br />
• Sp<strong>in</strong>e neutral, abdom<strong>in</strong>als<br />
braced, arms extended but<br />
unlocked, shoulders away<br />
from ears.<br />
• Pull body upwards towards<br />
bar.<br />
• Lower body under control to<br />
start position.<br />
• Repeat for desired<br />
repetitions.<br />
Muscles worked<br />
Options<br />
• Latissimus dorsi <strong>and</strong> posterior deltoid (shoulder extension).<br />
• Middle trapezius <strong>and</strong> rhomboids (shoulder girdle retraction).<br />
• Lower trapezius (shoulder girdle depression).<br />
• Biceps brachii (elbow flexion).<br />
• Lat pull-down.<br />
• Assisted ch<strong>in</strong>-up or pull-up<br />
mach<strong>in</strong>e.<br />
22<br />
Copyright © 2018 <strong>Active</strong> <strong>IQ</strong> Ltd. Not for resale
Unit 1<br />
Section 1: The cardiovascular system<br />
Heart valves<br />
Heart valves are formed from tough connective tissue <strong>and</strong> are made up of cusps, or flaps, that cover the entrance<br />
or exit to a vessel or chamber. They open <strong>and</strong> close passively, either sucked <strong>in</strong>to place or blown open depend<strong>in</strong>g on<br />
the differential pressure <strong>in</strong> each chamber or vessel.<br />
• Semilunar valves lie between the ventricles <strong>and</strong> arteries <strong>and</strong> prevent backflow of blood from the chamber<br />
to the vessel. The aortic semilunar valve separates the left ventricle <strong>and</strong> the aorta, <strong>and</strong> the pulmonary<br />
semilunar valve separates the right ventricle <strong>and</strong> pulmonary artery.<br />
• Atrioventricular (AV) valves lie between the atria <strong>and</strong> ventricles <strong>and</strong> prevent backflow of blood from the<br />
upper to lower chambers. The left AV valve is also known as the bicuspid valve (two cusps) or the mitral valve.<br />
The right AV valve is also known as the tricuspid valve (three cusps).<br />
Figure 1.1 The valves of the heart<br />
Contraction of the heart<br />
SA node<br />
The stimulation starts <strong>in</strong> the s<strong>in</strong>oatrial<br />
(SA) node.<br />
The heart is stimulated to contract by a complex series of <strong>in</strong>tegrated<br />
systems. The heart’s pacemaker – the s<strong>in</strong>oatrial (SA) node – <strong>in</strong>itiates the<br />
cardiac muscle contraction. The SA node is located <strong>in</strong> the wall of the right<br />
atrium (see Figure 1.2). The heart muscle is stimulated to contract about<br />
72 times per m<strong>in</strong>ute.<br />
Atria contract<br />
The <strong>in</strong>terconnected cardiac muscle<br />
fibres pass the impulse across the atria.<br />
AV node<br />
The atrioventricular (AV) node<br />
is stimulated <strong>and</strong> allows the full<br />
contraction of the atria before<br />
stimulat<strong>in</strong>g the ventricular muscle to<br />
contract.<br />
Ventricles contract<br />
The AV node stimulates the ventricular<br />
muscles to contract.<br />
Figure 1.2 The contraction of the heart<br />
8<br />
Copyright © 2017 <strong>Active</strong> <strong>IQ</strong> Ltd. Not for resale
Unit 5<br />
Section 2: Periodisation<br />
Section 2: Periodisation<br />
Programme periodisation is def<strong>in</strong>ed as: ‘The logical <strong>and</strong> systematic sequenc<strong>in</strong>g of tra<strong>in</strong><strong>in</strong>g factors <strong>in</strong> an <strong>in</strong>tegrative<br />
fashion <strong>in</strong> order to optimise specific tra<strong>in</strong><strong>in</strong>g outcomes at pre-determ<strong>in</strong>ed time po<strong>in</strong>ts’ (Bompa <strong>and</strong> Haff, 2009).<br />
Pr<strong>in</strong>ciples of periodisation<br />
The basic pr<strong>in</strong>ciple of periodisation is to break long-term programm<strong>in</strong>g <strong>in</strong>to separate blocks of tra<strong>in</strong><strong>in</strong>g. Each block<br />
is designed to progress a client towards a specific goal <strong>and</strong> elicit a specific adaptive response. These blocks are<br />
called phases or cycles.<br />
A periodised programme can be a strictly controlled structure that aims to improve elite competitive sport<strong>in</strong>g<br />
performance. In this form, the periodised plan could last a year or more. For example, an athlete who is work<strong>in</strong>g<br />
towards peak performance at a World Cup or at the Olympics could follow a periodised plan which lasts four years.<br />
Periodised plans can also be useful tools when work<strong>in</strong>g with general fitness <strong>and</strong> health-related clients as they<br />
can help to m<strong>in</strong>imise the risk of plateau or exhaustion whilst maximis<strong>in</strong>g progression, as well as add variety <strong>in</strong>to a<br />
programme to encourage adherence <strong>and</strong> enjoyment.<br />
General adaptation syndrome (GAS)<br />
Selye’s general adaptation syndrome theory (1984) was <strong>in</strong>itially developed to expla<strong>in</strong> how we cope with life <strong>in</strong><br />
general, however it has s<strong>in</strong>ce been used to expla<strong>in</strong> how we respond to <strong>and</strong> cope with the stresses placed on the<br />
body dur<strong>in</strong>g exercise (Baechle et al., 2000; Bompa <strong>and</strong> Haff, 2009). This theory also expla<strong>in</strong>s why periodisation <strong>and</strong><br />
variation are necessary with<strong>in</strong> progressive programmes.<br />
GAS – Adaptive responses to a new stimulus/stressor<br />
Stressor Phase 1 Phase 2<br />
Alarm phase<br />
Resistance phase<br />
2a - Adaptation<br />
2b - Plateau<br />
Phase 3<br />
Exhaustion<br />
Figure 2.1 General adaptation systems<br />
When a new tra<strong>in</strong><strong>in</strong>g stimulus is <strong>in</strong>troduced, the body <strong>in</strong>itially goes <strong>in</strong>to a type of shock (phase 1 – alarm phase)<br />
which leads to a decrease <strong>in</strong> performance. The alarm phase can last from several days to several weeks. Dur<strong>in</strong>g<br />
this phase the client may experience <strong>in</strong>creased fatigue, muscle soreness <strong>and</strong> stiffness, <strong>and</strong> reduced coord<strong>in</strong>ation<br />
<strong>and</strong> performance.<br />
The body will then beg<strong>in</strong> to adapt to the new stimuli <strong>and</strong> enter the resistance phase. The first part of this phase<br />
(phase 2a – adaptation phase) <strong>in</strong>volves significant change as the body makes a range of physiological adaptations<br />
<strong>in</strong> response to the dem<strong>and</strong>s be<strong>in</strong>g placed upon it (e.g. cardiovascular, respiratory <strong>and</strong> neuromuscular adaptations).<br />
238<br />
Copyright © 2017 <strong>Active</strong> <strong>IQ</strong> Ltd. Not for resale
Toolkit<br />
Section 1: Risk stratification models<br />
Section 1: Risk stratification<br />
models<br />
The risk stratification pyramid<br />
High risk<br />
Cl<strong>in</strong>ical exercise<br />
Specialist sessions<br />
Moderate/Medium risk<br />
Advanced Instructor (2)<br />
Referral scheme<br />
Low risk<br />
Advanced Instructor (1)<br />
Referral scheme<br />
Apparently healthy<br />
<strong>Level</strong> 2 <strong>in</strong>structor<br />
General exercise programmes<br />
Logic model for risk stratification<br />
1<br />
YES<br />
KNOWN CONDITIONS<br />
(CV, pulmonary or metabolic)<br />
CVD/PVD/Stroke/COPD/Asthma/Cystic fibrosis/Diabetes/Thyroid disorders.<br />
NO<br />
HIGH RISK<br />
CLINICALLY<br />
SUPERVISED<br />
PROGRAMME<br />
2<br />
SIGNS AND SYMPTOMS<br />
Ang<strong>in</strong>a pa<strong>in</strong> or discomfort/shortness of breath at rest or mild<br />
exertion/dizz<strong>in</strong>ess or syncope/ankle oedema/palpitations or<br />
tachycardia/<strong>in</strong>termittent claudication/known heart murmur/<br />
unusual fatigue or shortness of breath with usual activities.<br />
YES<br />
NO<br />
HIGH RISK<br />
CLINICALLY<br />
SUPERVISED<br />
PROGRAMME<br />
3<br />
CVD RISK FACTORS<br />
Age, family history,<br />
smok<strong>in</strong>g, sedentary,<br />
obesity, hypertension,<br />
dyslipidaemia, pre-diabetes.<br />
MORE THAN 2 OF<br />
THE ABOVE<br />
MODERATE RISK<br />
SUPERVISED<br />
PROGRAMME-<br />
LEVEL 3<br />
EXERCISE<br />
REFERRAL<br />
LESS THAN 2 OF<br />
THE ABOVE<br />
LOW RISK<br />
UNSUPERVISED<br />
PROGRAMME<br />
312<br />
Copyright © 2017 <strong>Active</strong> <strong>IQ</strong> Ltd. Not for resale