
You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Progress to date:<br />
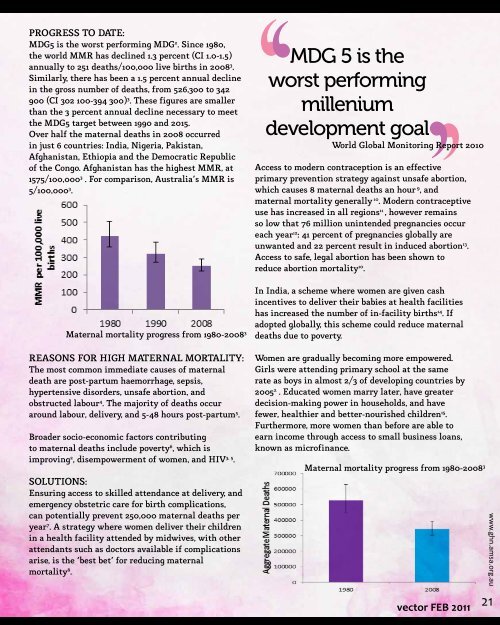
MDG5 is the worst performing MDG 2 . Since 1980,<br />
the world MMR has declined 1.3 percent (CI 1.0-1.5)<br />
annually to 251 deaths/100,000 live births in 2008 3 .<br />
Similarly, there has been a 1.5 percent annual decline<br />
in the gross number of deaths, from 526,300 to 342<br />
900 (CI 302 100-394 300) 3 . These figures are smaller<br />
than the 3 percent annual decline necessary to meet<br />
the MDG5 target between 1990 and 2015.<br />
Over half the maternal deaths in 2008 occurred<br />
in just 6 countries: India, Nigeria, Pakistan,<br />
Afghanistan, Ethiopia and the Democratic Republic<br />
of the Congo. Afghanistan has the highest MMR, at<br />
1575/100,000 3 ]. For comparison, Australia’s MMR is<br />
5/100,000 3 .<br />
‘‘<br />
MDG 5 is the<br />
worst performing<br />
millenium<br />
Access to modern contraception is an effective<br />
primary prevention strategy against unsafe abortion,<br />
which causes 8 maternal deaths an hour [9 , and<br />
maternal mortality generally 10 . Modern contraceptive<br />
use has increased in all regions 11] , however remains<br />
so low that 76 million unintended pregnancies occur<br />
each year <strong>12</strong> : 41 percent of pregnancies globally are<br />
unwanted and 22 percent result in induced abortion 13 .<br />
Access to safe, legal abortion has been shown to<br />
reduce abortion mortality 10 .<br />
‘‘<br />
development goal<br />
World Global Monitoring Report 2010<br />
Maternal mortality progress from 1980-2008 3<br />
Reasons for high maternal mortality:<br />
The most common immediate causes of maternal<br />
death are post-partum haemorrhage, sepsis,<br />
hypertensive disorders, unsafe abortion, and<br />
obstructed labour 4 . The majority of deaths occur<br />
around labour, delivery, and 5-48 hours post-partum 5 .<br />
Broader socio-economic factors contributing<br />
to maternal deaths include poverty 6 , which is<br />
improving 2 , disempowerment of women, and HIV 3, 5 .<br />
Solutions:<br />
Ensuring access to skilled attendance at delivery, and<br />
emergency obstetric care for birth complications,<br />
can potentially prevent 250,000 maternal deaths per<br />
year 7 . A strategy where women deliver their children<br />
in a health facility attended by midwives, with other<br />
attendants such as doctors available if complications<br />
arise, is the ‘best bet’ for reducing maternal<br />
mortality 8 .<br />
In India, a scheme where women are given cash<br />
incentives to deliver their babies at health facilities<br />
has increased the number of in-facility births 14 . If<br />
adopted globally, this scheme could reduce maternal<br />
deaths due to poverty.<br />
Women are gradually becoming more empowered.<br />
Girls were attending primary school at the same<br />
rate as boys in almost 2/3 of developing countries by<br />
2005 2 ]. Educated women marry later, have greater<br />
decision-making power in households, and have<br />
fewer, healthier and better-nourished children 15 .<br />
Furthermore, more women than before are able to<br />
earn income through access to small business loans,<br />
known as microfinance.<br />
Maternal mortality progress from 1980-2008 3<br />
vector FEB <strong>2011</strong><br />
21<br />
www.ghn.amsa.org.au