

Techniques for cryopreservation of individual or ... - Cleveland Clinic
Techniques for cryopreservation of individual or ... - Cleveland Clinic
Techniques for cryopreservation of individual or ... - Cleveland Clinic

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Human Reproduction Update, Vol.15, No.2 pp. 153–164, 2009<br />
Advanced Access publication on December 24, 2008 doi:10.1093/humupd/dmn061<br />
<strong>Techniques</strong> <strong>f<strong>or</strong></strong> <strong>cryopreservation</strong> <strong>of</strong><br />
<strong>individual</strong> <strong>or</strong> small numbers <strong>of</strong> human<br />
spermatozoa: a systematic review<br />
Faten AbdelHafez 1 , Mohamed Bedaiwy 2,3 , Sherif A. El-Nashar 2 ,<br />
Edmund Sabanegh 4 , and Nina Desai 1,5<br />
1 Department <strong>of</strong> Obstetrics and Gynecology, <strong>Cleveland</strong> <strong>Clinic</strong> Fertility Centre, <strong>Cleveland</strong> <strong>Clinic</strong> Foundation, <strong>Cleveland</strong>, OH, USA<br />
2 Department <strong>of</strong> Obstetrics and Gynecology, Assiut University Hospitals, Assiut, Egypt 3 Case Medical Centre, University Hospitals,<br />
Case Western Reserve University, <strong>Cleveland</strong>, Ohio, USA 4 Glickman Urological and Kidney Institute, <strong>Cleveland</strong> <strong>Clinic</strong> Foundation, <strong>Cleveland</strong>,<br />
OH, USA<br />
5<br />
C<strong>or</strong>respondence address. The <strong>Cleveland</strong> <strong>Clinic</strong> Fertility Center, 26900 Cedar Road, Beachwood, OH 44122, USA. Tel: þ1-216-839-2907;<br />
Fax: þ1-216-839-3180; E-mail: desain@ccf.<strong>or</strong>g<br />
table <strong>of</strong> contents<br />
...........................................................................................................................<br />
† Introduction<br />
† Methods<br />
† Results<br />
† Discussion<br />
† Conclusions<br />
background: Despite interest in <strong>cryopreservation</strong> <strong>of</strong> <strong>individual</strong> <strong>or</strong> small number <strong>of</strong> human spermatozoa, to date, little data is available<br />
as regards its effectiveness. We systematically reviewed the outcome after <strong>cryopreservation</strong> <strong>of</strong> <strong>individual</strong> <strong>or</strong> small numbers <strong>of</strong> human spermatozoa<br />
in patients with severe male fact<strong>or</strong> <strong>of</strong> infertility.<br />
methods: We searched the MEDLINE, EMBASE, Cochrane Systematic Reviews, CENTRAL, Web <strong>of</strong> Science, Scopus databases <strong>f<strong>or</strong></strong> relevant<br />
studies up to June <strong>of</strong> 2008. The search used terms referring to <strong>cryopreservation</strong> <strong>of</strong> small amount <strong>of</strong> sperm. Included studies were<br />
limited to human studies with no language restrictions.<br />
results: We identified 30 rep<strong>or</strong>ts including 9 carriers used <strong>f<strong>or</strong></strong> <strong>cryopreservation</strong> <strong>of</strong> small quantities/numbers <strong>of</strong> human spermatozoa<br />
(7 non-biological and 2 biological carriers). A wide variety <strong>of</strong> <strong>cryopreservation</strong> vehicles were rep<strong>or</strong>ted. The recovery rate <strong>of</strong> spermatozoa cryopreserved<br />
in a known small number varied widely from 59 to 100%. Fertilization rates were in the range <strong>of</strong> 18–67%. Frozen–thawed spermatozoa,<br />
using this method, were subsequently used <strong>f<strong>or</strong></strong> intracytoplasmic sperm injection in only five studies, with few pregnancies rep<strong>or</strong>ted so far.<br />
To date, there remains no consensus as to the ideal carrier <strong>f<strong>or</strong></strong> <strong>cryopreservation</strong> <strong>of</strong> small number <strong>of</strong> spermatozoa <strong>f<strong>or</strong></strong> clinical purposes.<br />
conclusions: Cryopreservation <strong>of</strong> <strong>individual</strong> <strong>or</strong> small numbers <strong>of</strong> human spermatozoa may replace the need <strong>f<strong>or</strong></strong> repeated surgical sperm<br />
retrieval. A controlled multicenter trial with sufficient follow-up would provide valid evidence <strong>of</strong> the potential benefit <strong>of</strong> this approach.<br />
Key w<strong>or</strong>ds: Epidydimal sperm / Testicular sperm / Single-sperm <strong>cryopreservation</strong> / Zona carrier / Cryoloop<br />
Introduction<br />
Couples with male fact<strong>or</strong> infertility represent 30–40% <strong>of</strong> the infertile<br />
population. Azoospermia accounts <strong>f<strong>or</strong></strong> 10% <strong>of</strong> all male fact<strong>or</strong> cases<br />
(Chandley, 1979). The birth <strong>of</strong> the first baby from intracytoplasmic<br />
sperm injection (ICSI) in 1992 (Palermo et al., 1992) marked a new era<br />
in the treatment <strong>of</strong> azoospermic men, who previously had no chance <strong>of</strong><br />
fathering a biologic child. New fertility treatments, such as ICSI combined<br />
with new advances in minimally invasive sperm recovery from the testis/<br />
epididymis (Schoysman et al., 1993; Devroey et al., 1995; Aboulghar et al.,<br />
1997; Ghazzawi et al., 1998; Nicopoullos et al., 2004), have proven to be<br />
viable and m<strong>or</strong>e practical treatment alternatives, in some patients, to<br />
microsurgical reconstruction <strong>of</strong> the male genital tract (Craft et al., 1993;<br />
Schoysman et al., 1993; Devroey et al., 1995).<br />
& The Auth<strong>or</strong> 2008. Published by Ox<strong>f<strong>or</strong></strong>d University Press on behalf <strong>of</strong> the European Society <strong>of</strong> Human Reproduction and Embryology. All rights reserved.<br />
F<strong>or</strong> Permissions, please email: journals.permissions@ox<strong>f<strong>or</strong></strong>djournals.<strong>or</strong>g
154 AbdelHafez et al.<br />
Surgical sperm recovery is <strong>of</strong>ten the rate-limiting step in successful<br />
IVF. With epididymal sperm aspirations, sperm recovery can be<br />
quite variable (45–97%) (Bladou et al., 1991; Craft et al., 1995;<br />
Lania et al., 2006). Testicular sperm recovery is even m<strong>or</strong>e difficult<br />
and subject to variation. Sperm recovery rates have been rep<strong>or</strong>ted<br />
to be only 36–64% with testicular biopsies (Schlegel et al., 1997;<br />
Palermo et al., 1999; Prins et al., 1999) and even lower in testicular<br />
aspirates (Hauser et al., 2006). Newer techniques involving testicular<br />
microdissection <strong>of</strong>fer improved sperm retrieval rates, even when previous<br />
conventional testicular biopsy has been unsuccessful. Regardless<br />
<strong>of</strong> the techniques used, sperm, if successfully recovered, are <strong>of</strong>ten<br />
weakly motile and present in small numbers, necessitating repeat surgical<br />
interventions if pregnancy is not achieved. This is costly and can<br />
entail significant risks to the patient. Multiple testicular biopsies can<br />
lead to inflammation <strong>or</strong> hematoma at the biopsy site and also to<br />
maj<strong>or</strong> complications such as testicular devascularization and fibrosis<br />
(Schlegel and Su, 1997). Serum testosterone levels can remain low<br />
<strong>f<strong>or</strong></strong> up to 1 year post-surgery (Manning et al., 1998). Although a<br />
study by Westlander et al. (2001) suggested that no maj<strong>or</strong> complications<br />
occur after repeated testicular aspiration, testicular damage<br />
could not be ruled out (Westlander et al., 2001). Further prospective<br />
studies are needed to address this possibility.<br />
Cryopreservation <strong>of</strong> surgically retrieved spermatozoa is there<strong>f<strong>or</strong></strong>e a<br />
very attractive and necessary strategy when dealing with severe male<br />
fact<strong>or</strong> infertility. Efficient <strong>cryopreservation</strong> <strong>of</strong> small numbers <strong>of</strong> sperm<br />
reduces the number <strong>of</strong> surgical interventions and thus avoids the complications<br />
and expenses associated with repeated surgeries. Using<br />
cryopreserved sperm also eliminates the logistical issues associated<br />
with co<strong>or</strong>dinating the women’s oocyte retrieval, with the urologist<br />
availability <strong>f<strong>or</strong></strong> surgical sperm retrieval from her partner. An indirect<br />
advantage <strong>of</strong> per<strong>f<strong>or</strong></strong>ming the sperm retrieval pri<strong>or</strong> to initiation <strong>of</strong> the<br />
IVF stimulation cycle is that the risk <strong>of</strong> no sperm being found on the<br />
day <strong>of</strong> oocyte retrieval can be avoided. Given the unique characteristics<br />
<strong>of</strong> epididymal and testicular spermatozoa, conventional<br />
methods <strong>of</strong> sperm <strong>cryopreservation</strong> may not be optimal. Novel <strong>cryopreservation</strong><br />
approaches are needed to improve recovery and postthaw<br />
parameters in these highly compromised sperm specimens.<br />
We per<strong>f<strong>or</strong></strong>med a systematic review <strong>of</strong> the literature to summarize<br />
the current evidence on the feasibility and efficacy <strong>of</strong> various<br />
methods <strong>f<strong>or</strong></strong> <strong>cryopreservation</strong> <strong>of</strong> surgically retrieved sperm <strong>f<strong>or</strong></strong> use<br />
in conjunction with assisted reproductive technology including techniques<br />
specifically designed <strong>f<strong>or</strong></strong> <strong>cryopreservation</strong> <strong>of</strong> small quantities/<br />
numbers <strong>of</strong> spermatozoa.<br />
Methods<br />
We rep<strong>or</strong>t this review acc<strong>or</strong>ding to the standards <strong>of</strong> the Quality <strong>of</strong> Rep<strong>or</strong>ting<br />
<strong>of</strong> Meta-analysis <strong>of</strong> Randomized Trials (QUOROM) and Observational<br />
Studies (MOOSE) statements (Stroup et al., 2000).<br />
Search strategy and identification <strong>of</strong> studies<br />
We per<strong>f<strong>or</strong></strong>med an electronic search on MEDLINE, EMBASE, Cochrane<br />
Systematic Reviews, CENTRAL, Web <strong>of</strong> Science, Scopus databases <strong>f<strong>or</strong></strong><br />
relevant studies from inception through June 2008. No language restrictions<br />
were applied. The search was limited to humans and used the following<br />
key w<strong>or</strong>ds: (cryopreserv* OR freez*) AND (small number OR Low OR<br />
few OR single) AND (sperm*). M<strong>or</strong>eover, we did a manual search in the<br />
abstract books <strong>of</strong> the American Society <strong>of</strong> Reproductive Medicine (ASRM)<br />
and the European Society <strong>of</strong> Human Reproduction and Embryology<br />
(ESHRE) meetings during the same time period. We decided be<strong>f<strong>or</strong></strong>ehand<br />
to include all studies related to <strong>cryopreservation</strong> <strong>of</strong> sperm in small quantities<br />
and numbers, regardless <strong>of</strong> the source <strong>of</strong> spermatozoa (ejaculated<br />
<strong>or</strong> surgically retrieved).<br />
Selection criteria and outcomes <strong>of</strong> interest<br />
The inclusion criteria <strong>f<strong>or</strong></strong> retrieved studies included published studies on<br />
the <strong>cryopreservation</strong> <strong>of</strong> small amount <strong>or</strong> number <strong>of</strong> spermatozoa. The<br />
primary outcome <strong>of</strong> the study was the post-thaw recovery rate. Secondary<br />
outcomes included: post-thaw motility, survival, fertilization, cleavage,<br />
clinical pregnancy, implantation and/<strong>or</strong> live birth rates. Recovery rate<br />
was defined as the number <strong>of</strong> spermatozoa recovered on post-thaw<br />
divided by the number <strong>of</strong> spermatozoa initially frozen 100. It was<br />
rep<strong>or</strong>ted only <strong>f<strong>or</strong></strong> the studies freezing a known number <strong>of</strong> spermatozoa.<br />
Motility rate, unless mentioned otherwise, was defined as the number <strong>of</strong><br />
motile spermatozoa divided by total number <strong>of</strong> spermatozoa 100.<br />
Two reviewers (F.A. and M.B.) independently reviewed the identified<br />
rep<strong>or</strong>ts. Disagreements in study inclusion were resolved by consensus.<br />
In addition, both reviewers independently reviewed the bibliographies <strong>of</strong><br />
the retrieved articles and the recent reviews <strong>f<strong>or</strong></strong> additional studies.<br />
Data extraction<br />
A standardized data extraction sheet was developed. One reviewer (F.A.)<br />
extracted the <strong>individual</strong> data from each included rep<strong>or</strong>t. The baseline<br />
clinical and demographic characteristics <strong>of</strong> the included studies were<br />
extracted. The procedure-specific data including the technique and the<br />
approach <strong>f<strong>or</strong></strong> sperm collection and <strong>cryopreservation</strong> were rec<strong>or</strong>ded.<br />
Study outcomes included post-thaw recovery, motility and viability rates,<br />
fertilization and cleavage rates, clinical pregnancy and implantation rates.<br />
Methodological quality <strong>of</strong> the included<br />
studies<br />
The methodological characteristics <strong>of</strong> the included studies including<br />
study design, number <strong>of</strong> participants and procedure-specific characteristics<br />
were collected. We developed a quality assessment <strong>f<strong>or</strong></strong>m using the<br />
validity criteria proposed by Juni et al. <strong>f<strong>or</strong></strong> clinical trials and the<br />
Newcastle–Ottawa Scale <strong>f<strong>or</strong></strong> coh<strong>or</strong>t studies (Hallak et al., 2000; Juni<br />
et al., 2001; Wells et al., 2007). Quality evaluation was per<strong>f<strong>or</strong></strong>med by<br />
two reviewers independently (M.B., F.A.) and any disagreement was<br />
resolved by consensus.<br />
Results<br />
Characteristics <strong>of</strong> the included studies<br />
Our initial electronic search identified 212 studies published in full text,<br />
<strong>of</strong> which 199 were excluded, whereas the manual search <strong>of</strong> the ASRM<br />
and ESHRE conferences books retrieved 10 abstracts from the proceedings<br />
<strong>of</strong> the relevant meetings in the field and a further 7<br />
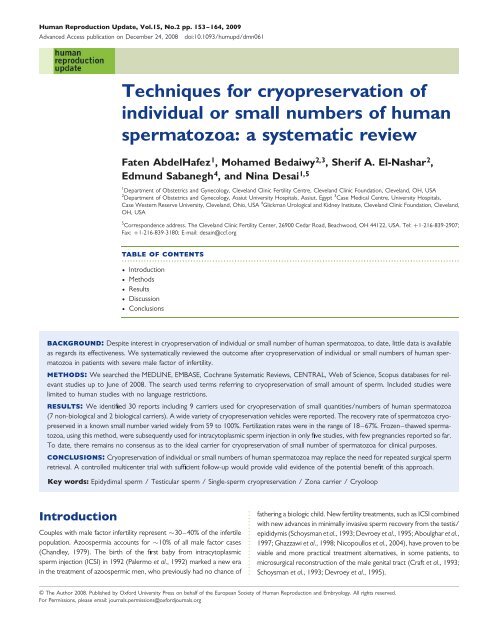
rep<strong>or</strong>ts were added from bibliography searches. A total <strong>of</strong> 30<br />
rep<strong>or</strong>ts <strong>of</strong> non-randomized trials were included in the current<br />
review (Fig. 1). The frozen–thawed sperm was subsequently used<br />
clinically via ICSI with subsequent transfer <strong>of</strong> the resultant embryos<br />
in only five (16.6%) studies. The methodological quality <strong>of</strong> the included<br />
studies was evaluated (Table I).<br />
A summary <strong>of</strong> published rep<strong>or</strong>ts addressing freezing spermatozoa<br />
(ejaculated <strong>or</strong> surgically retrieved) in microquantities <strong>or</strong> small
Methods <strong>f<strong>or</strong></strong> cryopreserving spermatozoa in small numbers 155<br />
Figure 1 Flow chart <strong>of</strong> the included peer-reviewed published<br />
studies and abstracts presented in the ASRM and ESHRE meetings.<br />
numbers was presented (Tables II and III). The quantity <strong>of</strong> cryopreserved<br />
sperm was noted in 20 rep<strong>or</strong>ts (12 full studies and 8 abstracts)<br />
(Cohen et al., 1997; Walmsley et al., 1998; Montag et al., 1999; Suzuki<br />
et al., 1999; B<strong>or</strong>ini et al., 2000; Liu et al., 2000; Quintans et al., 2000;<br />
Hsieh et al., 2000a; Fusi et al., 2001; Gvakharia and Adamson, 2001;<br />
Bouamama et al., 2003; Cesana et al., 2003; Levi-Setti et al., 2003;<br />
Sohn et al., 2003; Just et al., 2004; Desai et al., 2004a, b; Hassa<br />
et al., 2006; Isaev et al., 2007; Sereni et al., 2008) (Table II),<br />
whereas in the remaining studies, the number <strong>of</strong> cryopreserved spermatozoa<br />
was not known (Table III). Eleven <strong>of</strong> the studies documented<br />
sperm function by fertilization/cleavage data (Cohen et al., 1997;<br />
Walmsley et al., 1998; B<strong>or</strong>ini et al., 2000; Gil-Salom et al., 2000;<br />
Fusi et al., 2001; Nawroth et al., 2002; Desai et al., 2004a, b;<br />
Isachenko et al., 2004b; Koscinski et al., 2007; Sereni et al., 2008).<br />
Only five studies per<strong>f<strong>or</strong></strong>med embryo transfer (ET) and rep<strong>or</strong>ted pregnancy<br />
results (Walmsley et al., 1998; Gil-Salom et al., 2000; Fusi et al.,<br />
2001; Koscinski et al., 2007; Sereni et al., 2008). Nine types <strong>of</strong> <strong>cryopreservation</strong><br />
carriers were identified (seven non-biological and two biological).<br />
The different carrier types included: empty zona pellucida (Cohen<br />
et al., 1997; Walmsley et al., 1998; Montag et al., 1999; Suzuki et al.,<br />
1999; B<strong>or</strong>ini et al., 2000; Hsieh et al., 2000a; Fusi et al., 2001; Cesana<br />
et al., 2003; Levi-Setti et al., 2003; Hassa et al., 2006); straws,<br />
mini-straws and open-pulled straws (Desai et al., 1998; Isachenko<br />
et al., 2005; Koscinski et al., 2007); direct <strong>cryopreservation</strong> <strong>of</strong><br />
sperm in microdroplets (Gil-Salom et al., 2000; Quintans et al., 2000;<br />
Bouamama et al., 2003; Isachenko et al., 2005; Sereni et al., 2008);<br />
ICSI pipette (Gvakharia and Adamson, 2001; Sohn et al., 2003);<br />
Volvox globat<strong>or</strong> spheres (Just et al., 2004); alginate beads (Herrler<br />
et al., 2006); 5-mm copper loop (Nawroth et al., 2002; Isachenko<br />
et al., 2004b, 2005); cryoloop <strong>f<strong>or</strong></strong> microquantities (Schuster et al.,<br />
2003) and <strong>f<strong>or</strong></strong> small numbers <strong>of</strong> sperm (Desai et al., 2004b); and<br />
agarose microspheres (Isaev et al., 2007).<br />
Overall outcome <strong>of</strong> small known numbers <strong>of</strong><br />
spermatozoa frozen using different carriers<br />
Regarding studies that investigated freezing a selected small known<br />
number <strong>of</strong> spermatozoa, the overall average recovery rate was<br />
79.5% with a range <strong>of</strong> 59–100%. Whereas the motility rates rep<strong>or</strong>ted<br />
were distributed in a wide range starting from 0 to 100%. Survival rate<br />
was assessed in only three studies, and the overall average survival rate<br />
was 46.5% with a range <strong>of</strong> (8–85%). In studies that took a further step<br />
and per<strong>f<strong>or</strong></strong>med fertilization, the overall average fertilization rate was<br />
42.5% with a range <strong>of</strong> 18–67% (Table II).<br />
Overall outcome <strong>of</strong> microquantities <strong>of</strong><br />
spermatozoa frozen using different carriers<br />
F<strong>or</strong> studies where spermatozoa were frozen in microquantities, the<br />
overall average survival rate assessed using viability stains was 42%<br />
with a range <strong>of</strong> 24–60%. In addition, the post-thaw average number<br />
<strong>of</strong> motile spermatozoa was 32.5% with a range <strong>of</strong> 5–60% from the<br />
initially frozen spermatozoa. When fertilization was attempted, the<br />
average fertilization rate was 64.5% with a range <strong>of</strong> 54–75% (Table III).<br />
Outcome <strong>of</strong> IVF cycles using frozen–thawed<br />
sperm cryopreserved in small numbers<br />
In this group, only three studies used the frozen–thawed spermatozoa <strong>f<strong>or</strong></strong><br />
ICSI and ET <strong>of</strong> the resultant embryos (Walmsley et al., 1998; Fusi et al.,<br />
2001; Sereni et al., 2008). Two studies used the empty zona pellucida<br />
as the sperm carrier (Walmsley et al., 1998; Fusi et al., 2001), whereas<br />
Serini et al. froze the spermatozoa in microdroplets on a plastic dish<br />
(Sereni et al., 2008). In five patients using their frozen–thawed spermatozoa,<br />
Walmesly et al. rep<strong>or</strong>ted an average fertilization and cleavage rates <strong>of</strong><br />
65 and 90%, respectively. Thirty-one <strong>of</strong> the transferred embryos<br />
implanted resulted in the live birth <strong>of</strong> two set <strong>of</strong> twins (Walmsley et al.,<br />
1998). Similarly, Fusi et al. (2001) used thawed spermatozoa frozen in<br />
empty human zona pellucida <strong>f<strong>or</strong></strong> two couples in four cycles. Fifty-seven<br />
percent <strong>of</strong> the injected oocytes fertilized, <strong>of</strong> which 76% cleaved. ET was<br />
per<strong>f<strong>or</strong></strong>med in all four cycles with the mean <strong>of</strong> 3.25 embryos/cycle, resulting<br />
in the occurrence <strong>of</strong> one singleton pregnancy. In addition, the study by<br />
Sereni et al. rep<strong>or</strong>ted ICSI results using frozen–thawed testicular spermatozoa<br />
in six cases. The average fertilization and cleavage rates rep<strong>or</strong>ted<br />
were 17.6 and 77.8%, respectively. Seventy-one percent <strong>of</strong> those<br />
embryos were <strong>of</strong> good quality. ET in three cases resulted in only one biochemical<br />
pregnancy (Table II).<br />
Outcome <strong>of</strong> IVF cycles using frozen–thawed<br />
sperm cryopreserved in microquantities<br />
Regarding sperm freezing in microquantities, only two studies used the<br />
frozen–thawed spermatozoa <strong>f<strong>or</strong></strong> subsequent ICSI and ET (Gil-Salom<br />
et al., 2000; Koscinski et al., 2007).
Table I Quality assessment <strong>of</strong> the included coh<strong>or</strong>t studies acc<strong>or</strong>ding to the Newcastle–Ottawa Scale<br />
Included coh<strong>or</strong>t studies Selection<br />
................................................<br />
Comparability<br />
................................................................<br />
Outcome Total stars<br />
...........................................................<br />
........................................................................................................................................................................................................................................................<br />
a<br />
External validity Selection <strong>of</strong> (a) (b) Adequacy Selection Comparability Outcome<br />
(intervention) non-exposed Etiology <strong>of</strong> male Other fact<strong>or</strong>s including <strong>of</strong> follow-up<br />
coh<strong>or</strong>t<br />
coh<strong>or</strong>t<br />
fact<strong>or</strong> infertility age, female fact<strong>or</strong><br />
Bouamama et al. (2003) C E Yes No X ** *<br />
B<strong>or</strong>ini et al. (2000) A F Yes No X *** * *<br />
Cesana et al. (2003) B E No No X *** * *<br />
Cohen et al. (1997) B F No No X *** *<br />
Desai et al. (1998) B E No No X *** *<br />
Desai et al. (2004b) B E No No X *** *<br />
(Desai et al. 2004a) A E No No X *** *<br />
Fusi et al. (2001) A E No No U *** **<br />
Gil-Salom et al. (2000) A F No Yes U *** * **<br />
Gvakharia and Adamson (2001) B E No No X *** *<br />
Hassa et al. (2006) B F No No X *** *<br />
Herrler et al. (2006) C E Yes No X ** * **<br />
Hsieh et al. (2000a) A E No Yes X *** * *<br />
Isachenko et al. (2004b) C E Yes No X ** * *<br />
(Isachenko et al. 2004a) C E Yes No X ** * *<br />
Isachenko et al. (2005) B E Yes No X *** * *<br />
Isaev et al. (2007) B E No No X *** *<br />
Just et al. (2004) B E No No X *** *<br />
Koscinski et al. (2007) B F No No U *** **<br />
Levi-Setti et al. (2003) D E No No X ** *<br />
Liu et al. (2000) A E No No X ** *<br />
Montag et al. (1999) D E No No X ** *<br />
Nawroth et al. (2002) C E Yes No X ** * *<br />
Quintans et al. (2000) D E No No X ** *<br />
Quintans et al. (2000) C E Yes No X ** * *<br />
156 AbdelHafez et al.
Methods <strong>f<strong>or</strong></strong> cryopreserving spermatozoa in small numbers 157<br />
Schuster et al. (2003) C E Yes No X ** * *<br />
Sereni et al. (2008) A E No No U *** **<br />
Sohn et al. (2003) B E Yes No X *** * **<br />
Suzuki et al. (1999) D E No No X ** *<br />
Walmsley et al. (1998) A E No No U *** **<br />
External validity: A, truly representative <strong>of</strong> the azoospermic samples; B, somewhat representative <strong>of</strong> the average patient seen with the problem <strong>of</strong> interest; C, selected group; D, no description <strong>of</strong> the derivation <strong>of</strong> the coh<strong>or</strong>t.<br />
Selection <strong>of</strong> non-exposed coh<strong>or</strong>t: E, drawn from the same source as the intervention coh<strong>or</strong>t (concurrent controls); F, drawn from a different source (hist<strong>or</strong>ical controls); G, no description <strong>of</strong> the derivation <strong>of</strong> the non-exposed coh<strong>or</strong>t.<br />
Ascertainment <strong>of</strong> the intervention: categ<strong>or</strong>ies investigated: H, secure rec<strong>or</strong>d (e.g. surgical rec<strong>or</strong>ds); J, structured interview; K, written self-rep<strong>or</strong>t; L, no description. Note: all studies had written self-rep<strong>or</strong>ts (K).<br />
Incident disease: Demonstration that outcome <strong>of</strong> interest was not present at the start <strong>of</strong> the study: M, yes; N, no. Note: All studies were categ<strong>or</strong>y M.<br />
Comparability <strong>of</strong> coh<strong>or</strong>ts on the basis <strong>of</strong> the design <strong>or</strong> analysis: (a) study controls <strong>f<strong>or</strong></strong> the most imp<strong>or</strong>tant fact<strong>or</strong> (sperm <strong>cryopreservation</strong> method); and/<strong>or</strong> (b) study controls <strong>f<strong>or</strong></strong> any additional fact<strong>or</strong> (age, female fact<strong>or</strong>s, etc).<br />
Assesment <strong>of</strong> outcome: Categ<strong>or</strong>ies investigated—O, independent blind assessment; P, rec<strong>or</strong>d linkage; Q, self-rep<strong>or</strong>t; R, no description. Note: All studies had self-rep<strong>or</strong>ts (Q).<br />
Length <strong>of</strong> follow-up: Question asked: was follow-up long enough <strong>f<strong>or</strong></strong> outcomes to occur? S, yes; T, no. Note: In all studies, follow-up was long enough.<br />
Adequacy <strong>of</strong> follow-up: U, complete follow-up; all subjects were accounted <strong>f<strong>or</strong></strong>. V, subjects lost to follow-up were unlikely to introduce bias because small numbers were lost; .80% had follow-up, <strong>or</strong> description was provided <strong>of</strong> those lost. W,<br />
follow-up rate ,80%, and there was no description <strong>of</strong> those lost. X, no statement.<br />
a<br />
Total stars: a study can be awarded a maximum <strong>of</strong> one star <strong>f<strong>or</strong></strong> each item within the Selection and Outcome categ<strong>or</strong>ies and a maximum <strong>of</strong> two stars can be given <strong>f<strong>or</strong></strong> comparability. Thus, a perfect study will be awarded a total <strong>of</strong> nine stars<br />
distributed as follows: a total <strong>of</strong> four stars <strong>f<strong>or</strong></strong> the selection (a star <strong>f<strong>or</strong></strong> each item), two stars <strong>f<strong>or</strong></strong> the comparability (a star <strong>f<strong>or</strong></strong> each item) and three stars <strong>f<strong>or</strong></strong> the outcome (a star <strong>f<strong>or</strong></strong> each item).<br />
The freezing carriers used in those studies were microdroplets on<br />
ice ‘pills’ (Gil-Salom et al., 2000) and straws (Koscinski et al., 2007).<br />
In 234 ICSI cycles using frozen–thawed testicular spermatozoa, Gil<br />
Salom et al. rep<strong>or</strong>ted an average fertilization and cleavage rates <strong>of</strong><br />
63.2 and 84.6%, respectively. Transferring the resultant embryos in<br />
211 ET cycles resulted in a 27.8% clinical pregnancy rate per ET, a<br />
13.1% implantation rate per embryos transferred and 55 live births<br />
(Gil-Salom et al., 2000). The study by Koscinski et al. per<strong>f<strong>or</strong></strong>med<br />
ICSI using frozen–thawed spermatozoa in five cases, resulting in a fertilization<br />
rate <strong>of</strong> 54.7% (Koscinski et al., 2007) (Table III).<br />
Discussion<br />
Given the unique characteristics <strong>of</strong> epididymal and testicular spermatozoa,<br />
conventional methods <strong>of</strong> sperm <strong>cryopreservation</strong> are not<br />
optimal <strong>f<strong>or</strong></strong> <strong>cryopreservation</strong> <strong>of</strong> small numbers <strong>of</strong> sperm. Recognition<br />
<strong>of</strong> those problems has led to the expl<strong>or</strong>ation <strong>of</strong> methodologies specifically<br />
designed <strong>f<strong>or</strong></strong> cryopreserving limited numbers <strong>of</strong> motile sperm in<br />
miniscule volumes to facilitate recovery. The ideal carrier <strong>f<strong>or</strong></strong> <strong>cryopreservation</strong><br />
would allow the freezing <strong>of</strong> multiple tiny aliquots <strong>of</strong> sperm <strong>or</strong><br />
even <strong>individual</strong>ly isolated sperm in small numbers (i.e. 5–10 sperm per<br />
carrier), thus conserving the very small supply <strong>of</strong> motile sperm in<br />
azoospermic patients. This would prevent repeated freezing/thawing<br />
<strong>of</strong> the <strong>or</strong>iginal specimen, and yet allow multiple IVF attempts.<br />
A number <strong>of</strong> alternative <strong>cryopreservation</strong> carriers and techniques<br />
have been expl<strong>or</strong>ed to derive a viable clinical solution <strong>f<strong>or</strong></strong> this<br />
problem (Table IV). This approach is necessary if we are to successfully<br />
treat the severely azoospermic male and not put him at risk <strong>of</strong><br />
medical complications through multiple surgeries <strong>f<strong>or</strong></strong> sperm extraction.<br />
The current w<strong>or</strong>k examines techniques that have been applied<br />
towards this problem.<br />
Empty zona pellucida as sperm st<strong>or</strong>age<br />
vessels<br />
The concept <strong>of</strong> single-sperm <strong>cryopreservation</strong> was first introduced by<br />
Cohen et al. (1997). Their unique and novel idea <strong>of</strong> using an empty<br />
zona as a ‘pocket book’ to st<strong>or</strong>e <strong>individual</strong>ly selected spermatozoa<br />
has been the most widely used methodology <strong>f<strong>or</strong></strong> single-sperm freezing.<br />
This <strong>cryopreservation</strong> technique first requires the acquisition <strong>of</strong> animal<br />
<strong>or</strong> human zonae. Micromanipulation techniques and tools are used to<br />
evacuate cytoplasmic contents <strong>of</strong> animal <strong>or</strong> human oocytes. Individually<br />
selected sperm are then deposited into the empty zonae using an<br />
ICSI pipette (Cohen et al., 1997; B<strong>or</strong>ini et al., 2000). F<strong>or</strong> <strong>cryopreservation</strong>,<br />
the zonae are equilibrated with a test yolk: glycerol cryoprotectant<br />
agent (CPA) pri<strong>or</strong> to loading into conventional straws. Zonae are<br />
either vap<strong>or</strong>-frozen and then plunged in liquid nitrogen <strong>or</strong> frozen using<br />
a slow-rate-programmed freezer (Hassa et al., 2006). Empty zonae<br />
can also be pre-filled with CPA be<strong>f<strong>or</strong></strong>e sperm loading (Levi-Setti<br />
et al., 2003). Empty oocyte <strong>or</strong> embryonic zonae from rodents<br />
(mouse <strong>or</strong> hamster) (Cohen et al., 1997; Walmsley et al., 1998;<br />
Montag et al., 1999; Suzuki et al., 1999; Liu et al., 2000; Hsieh et al.,<br />
2000b) as well as from humans (Cohen et al., 1997; Walmsley<br />
et al., 1998; B<strong>or</strong>ini et al., 2000; Hsieh et al., 2000a; Fusi et al., 2001;<br />
Cesana et al., 2003; Levi-Setti et al., 2003; Hassa et al., 2006) have<br />
been successfully used.
Table II Cryopreservation <strong>of</strong> small known numbers <strong>of</strong> sperm<br />
Auth<strong>or</strong> Study type Number <strong>of</strong> Source <strong>of</strong> sperm Carrier Recovery rate Motility Survival Fertilization<br />
patients<br />
rate rate rate<br />
..........................................................................................................................................................................................................................................................<br />
Cohen et al. (1997) Full published 6 Po<strong>or</strong> ejaculate Human, mouse and hamster zona 73% 82% NA 50%<br />
*Walmsley et al. (1998) Full published 34 Po<strong>or</strong> ejaculate, surgically retrieved Human and hamster zonae 75% 67–100% NA 65%<br />
Montag et al. (1999) Full published NA Laser immobilized ejaculated<br />
sperm<br />
Human zona 92% NA 84% NA<br />
Suzuki et al. (1999) Abstract NA NA Hamster zona pellucida 63–70% 54–73% 65–85% NA<br />
B<strong>or</strong>ini et al. (2000) Full published 4 Testicular Human zonae 88% 27% NA 23%<br />
Hsieh et al. (2000a) Full published 16 Ejaculate, surgically retrieved Human and mouse zonae 82% 83% NA NA<br />
Liu et al. (2000) Full published 9 Testicular Mouse zonae 100% 58% 77% NA<br />
Quintans et al. (2000) Abstract NA NA Droplets on plastic dish 90–100% NA NA NA<br />
**Fusi et al. (2001) Abstract 2 Epidydimal Human zona pellucida NA NA NA 57%<br />
Gvakharia and Adamson (2001) Abstract 18 Ejaculate and testicular ICSI pipetts 92% 52% NA NA<br />
Bouamama et al. (2003) Full published NA N<strong>or</strong>mal ejaculate 0.5 ml microdrop 100% ,50% NA NA<br />
Levi-Setti et al. (2003) Full published 10 Ejaculate Human zona 59% 73% NA NA<br />
Cesana et al. (2003) Abstract NA Po<strong>or</strong> ejaculate Human zona 80–82% 0–***21% NA NA<br />
Sohn et al. (2003) Abstract 10 Po<strong>or</strong> ejaculate ICSI pipetts 80% NA 8% NA<br />
Desai et al. (2004a) Abstract 4 Epidydimal/testicular Cryoloops 72% NA NA 58%<br />
Desai et al. (2004b) Full published 10 Po<strong>or</strong> ejaculate Cryoloop 68% 73% NA 67%<br />
Just et al. (2004) Full published 15 Po<strong>or</strong> ejaculate Volvox globat<strong>or</strong> algae 100% 63% NA NA<br />
Hassa et al. (2006) Full Published NA N<strong>or</strong>mal and po<strong>or</strong> ejaculate Human zona NA 0–100% NA NA<br />
Isaev et al. (2007) Abstract 18 Po<strong>or</strong> ejaculate Agarose gel microspheres 70% <strong>of</strong><br />
microspheres<br />
78% NA<br />
****Sereni et al. (2008) Full Published 15 Testicular 5 ml drops in a plastic dish 100% 2% NA 18%<br />
*First live birth using hamster/human zona <strong>f<strong>or</strong></strong> single-sperm freezing.<br />
**Seventy-six percent <strong>of</strong> fertilized oocytes cleaved. After ET to two patients in four cycles, one singleton pregnancy resulted.<br />
***Induced motility by Pentoxifylline.<br />
****Seventy-eight percent <strong>of</strong> fertilized oocytes cleaved and a biochemical pregnancy resulted from transfer <strong>of</strong> six embryos to three patients.<br />
158 AbdelHafez et al.
Table III Cryopreservation <strong>of</strong> small quantities <strong>of</strong> sperm<br />
Auth<strong>or</strong> Study type Number <strong>of</strong> samples Source <strong>of</strong> sperm Carrier Survival rate Motility rate Fertilization rate<br />
..........................................................................................................................................................................................................................................................<br />
Desai et al. (1998) Abstract 20 Po<strong>or</strong> ejaculate Mini-straws NA *40% NA<br />
**Gil-Salom et al. (2000) Full published 234 ICSI cycle Testicular 100 ml droplets (pills) in cryovials NA NA 63%<br />
Nawroth et al. (2002) Full published 30 N<strong>or</strong>mal ejaculate 5 mm copper loop 60% *57% 3/4<br />
Schuster et al. (2003) Full published NA N<strong>or</strong>mal ejaculate Cryoloop NA 45% NA<br />
Isachenko et al. (2004a) Full published 18 N<strong>or</strong>mal ejaculate 5 mm copper loop NA *52% NA<br />
Isachenko et al. (2004b) Full published 38 N<strong>or</strong>mal ejaculate 5 mm copper loop NA *50–60% 79% (2PN þ 3PN)<br />
Isachenko et al. (2005) Full published 16 Po<strong>or</strong> ejaculate Straw NA *5–10% NA<br />
Open-pulled straw NA *5–10% NA<br />
Droplets NA *5–10% NA<br />
5 mm copper loop NA *,5% NA<br />
Quintans et al. (2000) Abstract 20 N<strong>or</strong>mal ejaculate Pellets in cryotube 24% NA NA<br />
Herrler et al. (2006) Full published 15 N<strong>or</strong>mal ejaculate Alginic acid drops 40–50% 20–30% NA<br />
***Koscinski et al. (2007) Full published 5 Po<strong>or</strong> ejaculate 30–50 ml instraws NA NA 54%<br />
*Percentage <strong>of</strong> post-thaw motility 100 divided by percentage <strong>of</strong> motility be<strong>f<strong>or</strong></strong>e <strong>cryopreservation</strong>.<br />
**<strong>Clinic</strong>al pregnancy and implantation rates were 28 and 13%, respectively.<br />
***<strong>Clinic</strong>al pregnancy rate was 20%.<br />
Methods <strong>f<strong>or</strong></strong> cryopreserving spermatozoa in small numbers 159
160 AbdelHafez et al.<br />
Table IV Summary <strong>of</strong> different used/suggested carriers<br />
<strong>f<strong>or</strong></strong> <strong>cryopreservation</strong> <strong>of</strong> surgically retrieved sperm in<br />
small quantities/numbers<br />
Non-biological Biological<br />
........................................................................................<br />
Straws/mini-straws/open-pulled straws Empty zonae <strong>of</strong> different<br />
species<br />
5 mm copper loop Volvox globat<strong>or</strong> algae<br />
Cryoloops<br />
Calcium alginate beads<br />
ICSI pipette<br />
Microdroplets on dry ice <strong>or</strong> plastic dish<br />
Agarose gel microspheres<br />
Variations in this protocol include making the slit with the aid <strong>of</strong> a<br />
LASER (Montag et al., 1999) and using different micropipette sizes<br />
ranging from 4–15 mm to drill and evacuate the cytoplasmic contents.<br />
Drilling small holes (7.5 mm) <strong>of</strong>ten resulted in oocyte rupture during<br />
cytoplasmic evacuation. This was not ideal since it increased the risk<br />
<strong>of</strong> leaving some host DNA fragments behind. These fragments could<br />
conceivably adhere to the spermatozoa being cryopreserved and<br />
later be inadvertently transferred into the oocyte during ICSI. Transfer<br />
<strong>of</strong> <strong>f<strong>or</strong></strong>eign DNA with sperm as vect<strong>or</strong>s has been rep<strong>or</strong>ted previously<br />
(Camaioni et al., 1992; Spada<strong>f<strong>or</strong></strong>a 1998). Using larger holes <strong>f<strong>or</strong></strong> the<br />
evacuation <strong>of</strong> cytoplasmic contents was also problematic, resulting in<br />
sperm loss. Attempts to seal the hole using oil droplets had limited<br />
effectiveness and interfered with sperm recovery post-thaw (Montag<br />
et al. 1999; Levi-Setti et al., 2003).<br />
Empty zonae as vessels <strong>f<strong>or</strong></strong> sperm st<strong>or</strong>age have several positive features.<br />
This technique is especially valuable in extreme cases <strong>of</strong><br />
oligozoospermia <strong>or</strong> azoospermia, which might require hours <strong>of</strong> microscopic<br />
screening to locate motile sperm. The zonae can be handled<br />
and visualized microscopically. Cryoprotectants can easily be added<br />
and removed without loss <strong>or</strong> dilution <strong>of</strong> sperm enclosed within the<br />
zona. Recovery <strong>of</strong> motile sperm sequestered in the zonae is quite<br />
simple upon thawing. Walmsley et al. rep<strong>or</strong>ted the first live births<br />
using human and hamster zonae <strong>f<strong>or</strong></strong> <strong>cryopreservation</strong> <strong>of</strong> epidydimal<br />
and testicular spermatozoa (Walmsley et al., 1998). They per<strong>f<strong>or</strong></strong>med<br />
five thaw cycles <strong>f<strong>or</strong></strong> five severe oligozoospermic/azoospermic patients.<br />
Three cycles resulted in pregnancies and two <strong>of</strong> them ended in the<br />
birth <strong>of</strong> two sets <strong>of</strong> twins. This was followed 3 years later, by a singleton<br />
pregnancy using oocyte-free human zonae <strong>f<strong>or</strong></strong> single epidydimal<br />
sperm <strong>cryopreservation</strong> (Fusi et al., 2001).<br />
Yet, despite its successful application, the routine use <strong>of</strong> the empty<br />
zona as a carrier vessel <strong>f<strong>or</strong></strong> single-sperm freezing has some drawbacks.<br />
The most serious limitation is the necessity <strong>of</strong> using a biologic carrier.<br />
New FDA and European Tissue Directive regulations, regarding<br />
exposure <strong>of</strong> human gametes and embryos to animal products, make<br />
the use <strong>of</strong> rodent zonae less feasible. Human zonae availability is<br />
also very restricted. M<strong>or</strong>eover, studies suggest lower recovery and fertilization<br />
rates with human sperm cryopreserved in human zonae,<br />
possibly as a result <strong>of</strong> sperm binding to ZP3 and induction <strong>of</strong> the acrosome<br />
reaction (Cohen et al., 1997). Furtherm<strong>or</strong>e, the process <strong>of</strong> zona<br />
preparation is lab<strong>or</strong>-intensive. The technique and hole size can affect<br />
the retention <strong>of</strong> motile sperm (Levi-Setti et al., 2003).<br />
Use <strong>of</strong> straws <strong>f<strong>or</strong></strong> <strong>cryopreservation</strong><br />
<strong>of</strong> microquantities <strong>of</strong> sperm<br />
F<strong>or</strong> surgically retrieved specimens from the epididymis and testis,<br />
cryopreserving multiple tiny aliquots, each sufficient <strong>f<strong>or</strong></strong> a single IVF<br />
attempt, is highly desirable. In our lab<strong>or</strong>at<strong>or</strong>y, mini-straws have been<br />
ideal <strong>f<strong>or</strong></strong> this task (Desai et al., 1998). Applied to specimens where<br />
at least one motile sperm was observed per high-powered field (300<br />
magnification), mini-straws have allowed us to efficiently freeze and<br />
conserve small aliquots <strong>of</strong> sperm. This technique utilizes embryo<br />
<strong>cryopreservation</strong> straws (0.2-mm diameter) aseptically cut into<br />
2.5-cm sections. One end is sealed with a plastic plug. A 15–20-ml<br />
aliquot <strong>of</strong> the sperm:CPA mixture is carefully loaded into the<br />
mini-straw using a drawn-out micropipette and the straw is sealed<br />
with another plastic plug. Five to six mini-straws are placed in conventional<br />
1.8-ml cryovials. The cryovial containing mini-straws is held in<br />
the vap<strong>or</strong> phase <strong>f<strong>or</strong></strong> 30 min be<strong>f<strong>or</strong></strong>e plunging into liquid nitrogen. F<strong>or</strong><br />
ICSI, one mini-straw can be thawed at a time, without affecting the<br />
remaining aliquots. Sperm motility and fertilization capacity were not<br />
affected by <strong>cryopreservation</strong> in smaller aliquots (unpublished data).<br />
However, any further reduction in sample volume was not feasible<br />
using this technique.<br />
Isachenko et al. used conventional and open-pulled straws <strong>f<strong>or</strong></strong><br />
vitrifying very small aliquots <strong>of</strong> 1 <strong>or</strong> 5 ml <strong>of</strong> sperm suspension from<br />
compromised semen samples. To create a closed sterile system,<br />
they placed the straw containing sperm into another 90-mm straw<br />
(Isachenko et al., 2005). M<strong>or</strong>e recently, Koscinski et al. (2007) used<br />
straws to freeze 30–50 ml <strong>of</strong> ejaculated sperm in cryptozoospermic<br />
patients. Using the straw as a carrier <strong>f<strong>or</strong></strong> freezing microquantities <strong>of</strong><br />
sperm is simple and easily applicable. Un<strong>f<strong>or</strong></strong>tunately, it is not ideal<br />
<strong>f<strong>or</strong></strong> severely impaired specimens where only small numbers <strong>of</strong><br />
sperm are present, and sperm can be lost due to adherence to the<br />
vessel wall. M<strong>or</strong>eover, <strong>individual</strong>ly selected sperm cannot be easily<br />
sequestered within the straw.<br />
Direct <strong>cryopreservation</strong> <strong>of</strong> sperm<br />
in microdroplets<br />
To circumvent sperm loss through adherence to the carrier vessel and<br />
to enable freezing <strong>of</strong> small volumes, investigat<strong>or</strong>s have expl<strong>or</strong>ed direct<br />
<strong>cryopreservation</strong> <strong>of</strong> sperm in microdroplets (Gil-Salom et al., 2000;<br />
Quintans et al., 2000). Aliquots <strong>of</strong> 50 <strong>or</strong> 100 ml <strong>of</strong> sperm:CPA<br />
mixture are placed on the surface <strong>of</strong> dry ice <strong>or</strong> cold stainless steel<br />
plate and then directly plunged into liquid nitrogen. These sperm<br />
aliquots <strong>or</strong> ‘pills’ can then be thawed as needed. Gil-Salom et al.<br />
successfully applied this methodology to testicular sperm (Gil-Salom<br />
et al., 2000). The clinical pregnancy and implantation rates with ICSI<br />
using cryopreserved/thawed testicular sperm were comparable with<br />
those using fresh testicular specimens. Similarly, Isachenko et al.<br />
vitrified spermatozoa in 40-ml droplets placed directly on dry ice<br />
but noted that upon warming, the motility was 40% lower than<br />
fresh control samples (Isachenko et al., 2005).<br />
Microdroplets have also been used to cryopreserve <strong>individual</strong>ly<br />
selected spermatozoa (Quintans et al., 2000; Bouamama et al.,<br />
2003; Sereni et al., 2008). Quintans et al. (2000) cryopreserved<br />
selected 4–6 spermatozoa in microdroplets under oil overlay in a<br />
plastic tissue culture dish. The dish was covered, wrapped with<br />
plastic stretch film and st<strong>or</strong>ed h<strong>or</strong>izontally in a liquid nitrogen tank.
Methods <strong>f<strong>or</strong></strong> cryopreserving spermatozoa in small numbers 161<br />
They rep<strong>or</strong>ted a post-thaw recovery rate <strong>of</strong> 90–100% (Quintans<br />
et al., 2000).<br />
Similarly, Bouamama et al. (2003) isolated up to 100 testicular<br />
sperm with the aid <strong>of</strong> an ICSI pipette and deposited them in a<br />
0.5-ml microdroplet <strong>of</strong> cryoprotectant medium under an oil overlay.<br />
The dish containing the microdroplet was then closed, sealed with<br />
parafilm and held in the vap<strong>or</strong> phase <strong>f<strong>or</strong></strong> 2 h be<strong>f<strong>or</strong></strong>e immersing in<br />
liquid nitrogen. Post-thaw recovery and motility rates were 100 and<br />
50%, respectively, but sperm function was not further assessed.<br />
Recently, Sereni et al. (2008) used a similar microdroplet technique<br />
to freeze <strong>individual</strong>ly selected testicular spermatozoa, obtained from a<br />
testicular needle aspiration. They applied this technique clinically in six<br />
cases. Post-thaw recovery rate was 100% (431/431). The pre-freeze<br />
motility rate was only 3.5%, and on thawing, 67% <strong>of</strong> sperm retained<br />
their motility. Nine out <strong>of</strong> 51 oocytes injected were fertilized. Three<br />
cases had an ET resulting in one biochemical pregnancy (Sereni<br />
et al., 2008).<br />
Neither <strong>of</strong> the microdroplet techniques <strong>f<strong>or</strong></strong> sperm <strong>cryopreservation</strong><br />
has been widely adopted. Direct application <strong>of</strong> sperm to the surface <strong>of</strong><br />
dry ice with no container physically isolating the specimen is concerning<br />
in a clinical environment and potentially increases the risk <strong>of</strong> crosscontamination.<br />
Culture dishes with microdroplets are also problematic<br />
since their size and shape make them m<strong>or</strong>e difficult to handle and<br />
st<strong>or</strong>e in conventional freezers and liquid nitrogen tanks. M<strong>or</strong>eover,<br />
polystyrene dishes do not stand up well to long-term st<strong>or</strong>age in<br />
liquid nitrogen and cannot be sealed to create a closed system.<br />
ICSI pipette <strong>f<strong>or</strong></strong> single-sperm freezing<br />
The use <strong>of</strong> the ICSI pipette as a sterile carrier <strong>f<strong>or</strong></strong> <strong>individual</strong>ly frozen<br />
spermatozoa has also been suggested (Gvakharia and Adamson,<br />
2001; Sohn et al., 2003). Gvakharia and Adamson (2001) cryopreserved<br />
ejaculated and testicular spermatozoa in ICSI pipettes<br />
(5–50 spermatozoa in each pipette). The post-thaw recovery and<br />
motility rates were 92 and 52%, respectively. Sohn et al. compared<br />
single-sperm freezing in ICSI pipettes using slow and ultrarapid freezing<br />
methodologies. Twenty-two spermatozoa from severe oligozoospermic<br />
patients were loaded into each ICSI pipette, which was either<br />
directly plunged in liquid nitrogen <strong>or</strong> vap<strong>or</strong>-frozen <strong>f<strong>or</strong></strong> 20 min pri<strong>or</strong><br />
to immersion in liquid nitrogen. The recovery and viability rates<br />
were 90 and 29% <strong>f<strong>or</strong></strong> slow freezing and 80 and 8% <strong>f<strong>or</strong></strong> ultrarapid freezing,<br />
respectively (Sohn et al., 2003).<br />
The use <strong>of</strong> the ICSI pipette as a vehicle <strong>f<strong>or</strong></strong> single-sperm freezing is<br />
simple and convenient but not practical <strong>f<strong>or</strong></strong> long-term st<strong>or</strong>age. The<br />
ICSI pipette tip is very fragile and can be broken easily. M<strong>or</strong>eover,<br />
sperm is being exposed and st<strong>or</strong>ed directly in liquid nitrogen raising<br />
the issue <strong>of</strong> cross-contamination.<br />
Volvox globat<strong>or</strong> spheres <strong>f<strong>or</strong></strong> sperm st<strong>or</strong>age<br />
and <strong>cryopreservation</strong><br />
The challenge <strong>of</strong> single-sperm freezing was addressed in a rather<br />
unique fashion by Just et al. (2004). This group injected ejaculated<br />
sperm from 15 patients, with less than 100 motile sperm/ml, into<br />
spheres <strong>of</strong> Volvox Globat<strong>or</strong> algae. Colonies from this alga consist <strong>of</strong><br />
1500 to 20 000 cells, held tightly in a sphere-like structure. Spheres<br />
were secured to a holding pipette and injected with motile sperm<br />
(n ¼ 8) using an ICSI needle. Algae spheres containing sperm were<br />
placed in CPA pri<strong>or</strong> to loading into straws, which were vap<strong>or</strong>-frozen<br />
and then immersed in liquid nitrogen, following a conventional semen<br />
<strong>cryopreservation</strong> protocol. After thawing <strong>of</strong> straws, sperm were<br />
extracted from algae spheres using an ICSI needle (Just et al., 2004).<br />
Despite the 100% on thaw sperm recovery and the .50% on postthaw<br />
motility, this system has several distinct disadvantages. One is<br />
exposure <strong>of</strong> the sperm to genetic material from the algae that can<br />
be potentially introduced into the oocytes during ICSI. However,<br />
axenic strains <strong>or</strong> radioactive irradiation inactivation can be used to circumvent<br />
this problem (Just et al., 2004). Although algae is inexpensive<br />
and easy to cultivate and handle during sperm loading, this method<br />
does involve preparation in advance <strong>of</strong> the procedure and requires<br />
a constant source <strong>of</strong> algae spheres growing in culture. M<strong>or</strong>eover,<br />
the new FDA and European Tissue Directive regulations make the<br />
use <strong>of</strong> algae (non-human tissue) to st<strong>or</strong>e human sperm unacceptable<br />
in a clinical setting.<br />
Microencapsulation <strong>of</strong> sperm<br />
in alginate beads<br />
Other investigat<strong>or</strong>s have expl<strong>or</strong>ed sperm microencapsulation in alginate<br />
beads as a means to cryopreserve small numbers <strong>of</strong> sperm<br />
(Herrler et al., 2006). Alginate is a non-toxic polysaccharide derived<br />
from different species <strong>of</strong> brown seaweed. Chemically, it is composed<br />
<strong>of</strong> repeated units <strong>of</strong> mannuronic and guluronic acid that can be linked<br />
by exposure to divalent cations as calcium, resulting in a gel <strong>f<strong>or</strong></strong>m<br />
status. Cells and tissues are added to the alginate be<strong>f<strong>or</strong></strong>e gellation.<br />
Cells can be released from the alginate matrix by calcium chelation.<br />
In this method, sperm was washed by centrifugation and the pellet<br />
mixed with CPA. This mixture was immediately mixed with alginic<br />
acid. The encapsulation was initiated by dropping small aliquots <strong>of</strong><br />
this mixture into a calcium chl<strong>or</strong>ide solution. The alginate capsules<br />
containing sperm were then washed, placed in CPA and frozen in<br />
straws using a programmable freezer. On thawing, alginate beads<br />
were dissolved in a sodium citrate solution. Sperm were isolated by<br />
centrifugation and washed free <strong>of</strong> alginate (Herrler et al., 2006).<br />
Good membrane diffusion and the inert nature <strong>of</strong> the alginate beads<br />
were the strongest positive features <strong>of</strong> this microencapsulating<br />
method. However, the initial testing, using ejaculated sperm specimens,<br />
revealed an almost 20% reduction in sperm motility. This significant<br />
decrease in sperm motility with encapsulation was attributed to<br />
the residual effect <strong>of</strong> alginic acid on sperm surfaces (Herrler et al.,<br />
2006). This may present a problem when dealing with severely compromised<br />
samples with po<strong>or</strong> initial motility. Sperm loss during the<br />
washing steps to remove alginic acid may also hamper the usefulness<br />
<strong>of</strong> this technique <strong>f<strong>or</strong></strong> surgically retrieved sperm.<br />
Cryoloop <strong>f<strong>or</strong></strong> sperm <strong>cryopreservation</strong><br />
in microquantities<br />
The cryoloop has also been expl<strong>or</strong>ed as a potential means to cryopreserve<br />
small volumes (Nawroth et al., 2002; Schuster et al., 2003;<br />
Isachenko et al., 2004b, 2005) and numbers <strong>of</strong> sperm (Desai et al.,<br />
2004b). The cryoloop was first introduced <strong>f<strong>or</strong></strong> embryo <strong>cryopreservation</strong><br />
by Lane et al. (1999). The miniscule fluid volume measuring<br />
between one-tenth and one-hundredth <strong>of</strong> a microliter makes this an<br />
excellent vessel <strong>f<strong>or</strong></strong> vitrification protocols that require an ultrarapid<br />
freezing rate to prevent ice crystallization. Sperm <strong>cryopreservation</strong>
162 AbdelHafez et al.<br />
by vitrification on cryoloops has been expl<strong>or</strong>ed (Isachenko et al.,<br />
2004a). Sperm motility after vitrification was found to be similar to<br />
that after conventional slow freeze. However, to date, the conventional<br />
slow and vap<strong>or</strong> freeze methods remain to be the commonly used<br />
sperm <strong>cryopreservation</strong> techniques. To our knowledge, pregnancies<br />
using vitrified/warmed sperm have not been rep<strong>or</strong>ted.<br />
Schuster et al. (2003) and Desai et al. (2004a, b) combined the<br />
cryoloop methodology with the conventional slow-freezing protocol<br />
to cryopreserve very low numbers <strong>of</strong> sperm in tiny aliquots. The cryoloop<br />
proved to be a convenient vessel <strong>f<strong>or</strong></strong> the st<strong>or</strong>age <strong>of</strong> tiny aliquots<br />
<strong>of</strong> sperm. Sperm loss was minimal since there were no surfaces <strong>f<strong>or</strong></strong><br />
sperm adherence. Elimination <strong>of</strong> centrifugation-wash steps also conserved<br />
sperm (Schuster et al., 2003).<br />
Desai et al. (2004a, b) proposed the use <strong>of</strong> the cryoloop as an<br />
alternative to hamster zona <strong>f<strong>or</strong></strong> freezing <strong>individual</strong> sperm. The <strong>individual</strong>ly<br />
selected ejaculated sperm were picked up using an ICSI pipette<br />
and deposited directly on a cryoprotectant film covering the nylon<br />
loop (Desai et al., 2004b). Single-sperm freezing on cryoloops<br />
proved to be straight<strong>f<strong>or</strong></strong>ward. No difference was observed in postthaw<br />
motility after <strong>cryopreservation</strong> on loops versus in conventional<br />
vials. Among the <strong>individual</strong>ly cryopreserved sperm, 73% retained motility.<br />
Further sperm-function testing demonstrated that these <strong>individual</strong>ly<br />
cryopreserved sperm were indeed capable <strong>of</strong> inducing sperm head<br />
decondensation and pronuclear <strong>f<strong>or</strong></strong>mation when injected into human<br />
oocytes (Desai et al., 2004b).<br />
The cryoloop as a carrier was further tested using <strong>individual</strong> sperm<br />
isolated from both epididymal and testicular specimens (Desai et al.,<br />
2004a). Cryoloops were loaded with two to eight <strong>individual</strong>ly selected<br />
epididymal <strong>or</strong> testicular sperm, vap<strong>or</strong>-frozen and then immersed in<br />
liquid nitrogen. Seventy-two percent (23/32) <strong>of</strong> the <strong>individual</strong>ly<br />
selected and cryopreserved epididymal/testicular sperm were recovered.<br />
On thaw, motility was usually minimal (slight head motion <strong>or</strong><br />
twitching), but the maj<strong>or</strong>ity <strong>of</strong> sperm had flexible tails, an indicat<strong>or</strong><br />
<strong>of</strong> potential viability. Both epididymal and testicular sperm cryopreserved<br />
on cryoloops were capable <strong>of</strong> fertilizing oocytes (Desai et al.,<br />
2004a).<br />
As a carrier, the inert, non-biologic nature <strong>of</strong> the nylon material <strong>of</strong><br />
the cryoloop helps to circumvent many <strong>of</strong> the problems associated<br />
with the methodologies involving animal zonae <strong>or</strong> algae spheres.<br />
Sperm can be sequestered easily but without encapsulation, so<br />
there is no need to expose them to compounds that might decrease<br />
motility, such as alginic acid. Cryoloops can be commercially purchased<br />
and require no additional preparation. Cryovials are m<strong>or</strong>e<br />
easily st<strong>or</strong>ed in conventional liquid nitrogen st<strong>or</strong>age containers and<br />
freezers than tissue culture dishes <strong>or</strong> micropipettes containing<br />
sperm. The maj<strong>or</strong> drawback <strong>of</strong> the cryoloop as a carrier is that it is<br />
an open system. Since sperm are directly exposed to liquid nitrogen<br />
within the vial, the potential risk <strong>of</strong> cross-contamination has been<br />
raised. The miniscule volumes <strong>of</strong> fluid on the loop, generally less<br />
than one-tenth <strong>of</strong> a microliter in the case <strong>of</strong> single-sperm freezing, realistically<br />
make this risk negligible. However, new FDA and European<br />
Tissue Directive regulations discourage the use <strong>of</strong> open systems <strong>f<strong>or</strong></strong><br />
gamete preservation. Modifications <strong>of</strong> the <strong>or</strong>iginal technique by enclosure<br />
<strong>of</strong> cryoloop-containing vials (Larman et al., 2006), st<strong>or</strong>age and<br />
freezing in the vap<strong>or</strong> phase and sterile liquid nitrogen delivery<br />
systems are all potential approaches to improving the widespread<br />
acceptance <strong>of</strong> cryoloops as carrier vessels <strong>f<strong>or</strong></strong> <strong>individual</strong>ly selected<br />
sperm. Future clinical trials with sperm frozen on cryoloops in a<br />
closed system are needed to further evaluate this carrier system.<br />
Sperm freezing in agarose microspheres<br />
Recently, Isaev et al. used 2% agarose microspheres (100 mm in diameter)<br />
as a non-biological analogue to zona pellucida (Isaev et al., 2007).<br />
Using micromanipulation tools, each microsphere was loaded with<br />
1–10 spermatozoa and placed in CPA solution <strong>f<strong>or</strong></strong> 5 min to equilibrate.<br />
One to five agarose microspheres loaded with sperm were<br />
then put in to 0.25 cc plastic straws, vap<strong>or</strong>-frozen and then plunged<br />
into liquid nitrogen. Using this technique, a total <strong>of</strong> 318 motile<br />
spermatozoa were cryopreserved in 67 microspheres. On thaw,<br />
78% <strong>of</strong> recovered spermatozoa were motile (Isaev et al., 2007).<br />
Two microspheres containing seven sperm were lost. Agarose microspheres<br />
represent another inert non-biologic carrier <strong>f<strong>or</strong></strong> freezing small<br />
numbers <strong>of</strong> sperm. M<strong>or</strong>e details on the steps involved in microsphere<br />
preparation and use, along with sperm function testing data, will<br />
however be needed to assess functionality as a potential carrier <strong>f<strong>or</strong></strong><br />
clinical application.<br />
Conclusions<br />
Cryopreservation <strong>of</strong> surgically retrieved spermatozoa from the epididymis<br />
and testis is a valuable component in effective treatment and<br />
management <strong>of</strong> male infertility, reducing the necessity <strong>of</strong> repeat surgeries.<br />
Biological and non-biological carriers have been tried <strong>f<strong>or</strong></strong> <strong>cryopreservation</strong><br />
<strong>of</strong> low numbers <strong>of</strong> spermatozoa. Thawed spermatozoa<br />
were used <strong>f<strong>or</strong></strong> subsequent ICSI and ET in only five studies. No prospective,<br />
randomized controlled trials were per<strong>f<strong>or</strong></strong>med to show that<br />
any single carrier is superi<strong>or</strong> to the others. It is clear that conventional<br />
methodology cannot effectively address these problems. Surgically<br />
retrieved specimens are <strong>of</strong>ten heavily loaded with red blood cells,<br />
cellular debris, testicular cells and a large number <strong>of</strong> dead <strong>or</strong> immotile<br />
sperm. Concentrating such samples into small volumes to cryopreserve<br />
can actually have a detrimental effect on the few observed<br />
motile sperm (Aitken and Clarkson, 1988; M<strong>or</strong>timer and M<strong>or</strong>timer,<br />
1992). Lack <strong>of</strong> easily implemented technology to handle such cases<br />
remains a maj<strong>or</strong> deterrent to single-sperm freezing.<br />
M<strong>or</strong>e than a decade had passed since pregnancies were described<br />
after the use <strong>of</strong> human <strong>or</strong> hamster zonae <strong>f<strong>or</strong></strong> st<strong>or</strong>ing one <strong>or</strong> few spermatozoa.<br />
To date, there is a limited use <strong>of</strong> this technology by urologists<br />
and gynecologists in the maj<strong>or</strong>ity <strong>of</strong> the IVF programs. It is<br />
indeed a missed opp<strong>or</strong>tunity to improve on the quality <strong>of</strong> care provided<br />
to that subset <strong>of</strong> patients. Failure <strong>of</strong> this technology to have<br />
mainstream use remains multi-fact<strong>or</strong>ial. First, there is a paucity <strong>of</strong><br />
clinical data on its effectiveness. In addition, there is a lack <strong>of</strong> the<br />
ideal container <strong>or</strong> vehicle that could be used universally. Even the<br />
cryoloop that we proposed 3 years ago has its own limitations and<br />
drawbacks. We are now trying some modifications to the cryoloop<br />
technique to be m<strong>or</strong>e feasible <strong>f<strong>or</strong></strong> clinical application.<br />
Novel <strong>cryopreservation</strong> technology specifically designed to handle<br />
small numbers and quantities <strong>of</strong> sperm needs to be further expl<strong>or</strong>ed.<br />
To date, there have been few published studies on <strong>cryopreservation</strong> <strong>of</strong><br />
small numbers <strong>of</strong> testicular <strong>or</strong> epididymal sperm in extremely impaired<br />
surgical specimens. The current evidence is not sufficient to supp<strong>or</strong>t<br />
the use <strong>of</strong> one technology over the other. Well-designed clinical
Methods <strong>f<strong>or</strong></strong> cryopreserving spermatozoa in small numbers 163<br />
trials with appropriate sample sizes are needed to assess the feasibility<br />
and efficiency <strong>of</strong> various low sperm count freezing methodologies.<br />
References<br />
Aboulghar MA, Mansour RT, Serour GI, Fahmy I, Kamal A, Tawab NA,<br />
Amin YM. Fertilization and pregnancy rates after intracytoplasmic<br />
sperm injection using ejaculate semen and surgically retrieved sperm.<br />
Fertil Steril 1997;68:108–111.<br />
Aitken RJ, Clarkson JS. Significance <strong>of</strong> reactive oxygen species and<br />
antioxidants in defining the efficacy <strong>of</strong> sperm preparation techniques.<br />
J Androl 1988;9:367–376.<br />
Bladou F, Grillo JM, Rossi D, Noizet A, Gamerre M, Erny R, Luciani JM,<br />
Serment G. Epididymal sperm aspiration in conjunction with in-vitro<br />
fertilization and embryo transfer in cases <strong>of</strong> obstructive azoospermia.<br />
Hum Reprod 1991;6:1284–1287.<br />
B<strong>or</strong>ini A, Sereni E, Bonu MA, Flamigni C. Freezing a few testicular<br />
spermatozoa retrieved by TESA. Mol Cell Endocrinol 2000;169:27–32.<br />
Bouamama N, Briot P, Testart J. Comparison <strong>of</strong> two methods <strong>of</strong><br />
cryoconservation <strong>of</strong> sperm when in very small numbers. Gynecol<br />
Obstet Fertil 2003;31:132–135.<br />
Camaioni A, Russo MA, Od<strong>or</strong>isio T, Gandolfi F, Fazio VM, Siracusa G.<br />
Uptake <strong>of</strong> exogenous DNA by mammalian spermatozoa: specific<br />
localization <strong>of</strong> DNA on sperm heads. J Reprod Fertil 1992;96:203–212.<br />
Cesana A, Novara P, Bianchi S, Marras A, Albani E, Negri L, Levi-Setti PE.<br />
Sperm <strong>cryopreservation</strong> in oligo-asthenospermic patients. The 19th<br />
Annual Meeting <strong>of</strong> the ESHRE, Madrid, Spain. Hum Reprod 2003;<br />
18:xviii76.<br />
Chandley AC. The chromosomal basis <strong>of</strong> human infertility. Br Med Bull<br />
1979;35:181–186.<br />
Cohen J, Garrisi GJ, Congedo-Ferrara TA, Kieck KA, Schimmel TW,<br />
Scott RT. Cryopreservation <strong>of</strong> single human spermatozoa. Hum<br />
Reprod 1997;12:994–1001.<br />
Craft I, Bennett V, Nicholson N. Fertilising ability <strong>of</strong> testicular<br />
spermatozoa. Lancet 1993;342:864.<br />
Craft I, Tsirigotis M, Bennett V, Taranissi M, Khalifa Y, Hogewind G,<br />
Nicholson N. Percutaneous epididymal sperm aspiration and<br />
intracytoplasmic sperm injection in the management <strong>of</strong> infertility due<br />
to obstructive azoospermia. Fertil Steril 1995;63:1038–1042.<br />
Desai N, Glavan D, Goldfarb J. A convenient technique <strong>f<strong>or</strong></strong><br />
<strong>cryopreservation</strong> <strong>of</strong> micro quantities <strong>of</strong> sperm. Fertil Steril 1998;<br />
S197–S198. Annual meeting program supplement.<br />
Desai N, Culler C, Goldfarb J. Cryopreservation <strong>of</strong> single sperm from<br />
epidydimal and testicular samples on cryoloops: preliminary case<br />
rep<strong>or</strong>t. Fertil Steril 2004a;82:S264.<br />
Desai NN, Blackmon H, Goldfarb J. Single sperm <strong>cryopreservation</strong> on<br />
cryoloops: an alternative to hamster zona <strong>f<strong>or</strong></strong> freezing <strong>individual</strong><br />
spermatozoa. Reprod Biomed Online 2004b;9:47–53.<br />
Devroey P, Liu J, Nagy Z, Goossens A, Tournaye H, Camus M, Van<br />
Steirteghem A, Silber S. Pregnancies after testicular sperm extraction<br />
and intracytoplasmic sperm injection in non-obstructive azoospermia.<br />
Hum Reprod 1995;10:1457–1460.<br />
Fusi F, Calzi F, Rabellotti E, Papaleo E, Gonfiantini C, Bonzi V, Santis LD,<br />
Ferrari A. Fertilizing capability <strong>of</strong> frozen-thawed spermatozoa recovered<br />
from microsurgical epidydimal sperm aspiration and cryopreserved in<br />
oocyte-free human zona pellucida. Hum Reprod 2001;16:117.<br />
Ghazzawi IM, Sarraf MG, Taher MR, Khalifa FA. Comparison <strong>of</strong> the<br />
fertilizing capability <strong>of</strong> spermatozoa from ejaculates, epididymal<br />
aspirates and testicular biopsies using intracytoplasmic sperm injection.<br />
Hum Reprod 1998;13:348–352.<br />
Gil-Salom M, Romero J, Rubio C, Ruiz A, Remohi J, Pellicer A.<br />
Intracytoplasmic sperm injection with cryopreserved testicular<br />
spermatozoa. Mol Cell Endocrinol 2000;169:15–19.<br />
Gvakharia M, Adamson GD. A method <strong>of</strong> successful <strong>cryopreservation</strong> <strong>of</strong><br />
small numbers <strong>of</strong> human spermatozoa. Fertil Steril 2001;76:S101.<br />
Hallak J, Sharma RK, Wellstead C, Agarwal A. Cryopreservation <strong>of</strong> human<br />
spermatozoa: comparison <strong>of</strong> TEST-yolk buffer and glycerol. Int J Fertil<br />
Womens Med 2000;45:38–42.<br />
Hassa H, Gurer F, Yildirm A, Can C, Sahinturk V, Tekin B. A new<br />
protection solution <strong>f<strong>or</strong></strong> freezing small numbers <strong>of</strong> sperm inside empty<br />
zona pellucida: Osmangazi-Turk solution. Cell Preserv Technol 2006;<br />
4:199–208.<br />
Hauser R, Yogev L, Paz G, Yavetz H, Azem F, Lessing JB, Botchan A.<br />
Comparison <strong>of</strong> efficacy <strong>of</strong> two techniques <strong>f<strong>or</strong></strong> testicular sperm<br />
retrieval in nonobstructive azoospermia: multifocal testicular sperm<br />
extraction versus multifocal testicular sperm aspiration. J Androl 2006;<br />
27:28–33.<br />
Herrler A, Eisner S, Bach V, Weissenb<strong>or</strong>n U, Beier HM. Cryopreservation<br />
<strong>of</strong> spermatozoa in alginic acid capsules. Fertil Steril 2006;85:208–213.<br />
Hsieh Y, Tsai H, Chang C, Lo H. Cryopreservation <strong>of</strong> human spermatozoa<br />
within human <strong>or</strong> mouse empty zona pellucidae. Fertil Steril 2000a;<br />
73:694–698.<br />
Hsieh YY, Tsai HD, Chang CC, Lo HY. Sperm <strong>cryopreservation</strong> with<br />
empty human <strong>or</strong> mouse zona pellucidae. A comparison. J Reprod Med<br />
2000b;45:383–386.<br />
Isachenko E, Isachenko V, Katkov II, Rahimi G, Schond<strong>or</strong>f T, Mallmann P,<br />
Dessole S, Nawroth F. DNA integrity and motility <strong>of</strong> human<br />
spermatozoa after standard slow freezing versus cryoprotectant-free<br />
vitrification. Hum Reprod 2004a;19:932–939.<br />
Isachenko V, Isachenko E, Katkov II, Montag M, Dessole S, Nawroth F,<br />
Van Der Ven H. Cryoprotectant-free <strong>cryopreservation</strong> <strong>of</strong> human<br />
spermatozoa by vitrification and freezing in vap<strong>or</strong>: effect on motility,<br />
DNA integrity, and fertilization ability. Biol Reprod 2004b;71:1167–1173.<br />
Isachenko V, Isachenko E, Montag M, Zaeva V, Krivokharchenko I,<br />
Nawroth F, Dessole S, Katkov II, van der Ven H. Clean technique <strong>f<strong>or</strong></strong><br />
cryoprotectant-free vitrification <strong>of</strong> human spermatozoa. Reprod Biomed<br />
Online 2005;10:350–354.<br />
Isaev DA, Zaletov SY, Zaeva VV, Zakharova EE, Shafei RA,<br />
Krivokharchenko IS. Artificial microcontainers <strong>f<strong>or</strong></strong> <strong>cryopreservation</strong> <strong>of</strong><br />
solitary spermatozoa. Hum Reprod 2007;22:i154.<br />
Juni P, Altman DG, Egger M. Systematic reviews in health care: assessing<br />
the quality <strong>of</strong> controlled clinical trials. BMJ 2001;323:42–46.<br />
Just A, Gruber I, Wober M, Lahodny J, Obruca A, Strohmer H. Novel<br />
method <strong>f<strong>or</strong></strong> the <strong>cryopreservation</strong> <strong>of</strong> testicular sperm and ejaculated<br />
spermatozoa from patients with severe oligospermia: a pilot study.<br />
Fertil Steril 2004;82:445–447.<br />
Koscinski I, Wittemer C, Lefebvre-Khalil V, Marcelli F, Defossez A,<br />
Rigot JM. Optimal management <strong>of</strong> extreme oligozoospermia by an<br />
appropriate <strong>cryopreservation</strong> programme. Hum Reprod 2007;<br />
22:2679–2684.<br />
Lane M, Bavister BD, Lyons EA, F<strong>or</strong>est KT. Containerless vitrification<br />
<strong>of</strong> mammalian oocytes and embryos. Nat Biotechnol 1999;<br />
17:1234–1236.<br />
Lania C, Grasso M, F<strong>or</strong>tuna F, De Santis L, Fusi F. Open epididymal sperm<br />
aspiration (OESA): minimally invasive surgical technique <strong>f<strong>or</strong></strong> sperm<br />
retrieval. Arch Esp Urol 2006;59:313–316.<br />
Larman MG, Sheehan CB, Gardner DK. Vitrification <strong>of</strong> mouse pronuclear<br />
oocytes with no direct liquid nitrogen contact. Reprod Biomed Online<br />
2006;12:66–69.<br />
Levi-Setti PE, Albani E, Negri L, Cesana A, Novara P, Bianchi S.<br />
Cryopreservation <strong>of</strong> a small number <strong>of</strong> spermatozoa in yolk-filled<br />
human zonae pellucidae. Arch Ital Urol Androl 2003;75:195–198.
164 AbdelHafez et al.<br />
Liu J, Zheng XZ, Baramki TA, Compton G, Yazigi RA, Katz E.<br />
Cryopreservation <strong>of</strong> a small number <strong>of</strong> fresh human testicular<br />
spermatozoa and testicular spermatozoa cultured in vitro <strong>f<strong>or</strong></strong> 3 days<br />
in an empty zona pellucida. J Androl 2000;21:409–413.<br />
Manning M, Junemann KP, Alken P. Decrease in testosterone blood<br />
concentrations after testicular sperm extraction <strong>f<strong>or</strong></strong> intracytoplasmic<br />
sperm injection in azoospermic men. Lancet 1998;352:37.<br />
Montag M, Rink K, Dieckmann U, Delacretaz G, van der Ven H.<br />
Laser-assisted <strong>cryopreservation</strong> <strong>of</strong> single human spermatozoa in<br />
cell-free zona pellucida. Andrologia 1999;31:49–53.<br />
M<strong>or</strong>timer D, M<strong>or</strong>timer ST. Methods <strong>of</strong> sperm preparation <strong>f<strong>or</strong></strong> assisted<br />
reproduction. Ann Acad Med Singap<strong>or</strong>e 1992;21:517–524.<br />
Nawroth F, Isachenko V, Dessole S, Rahimi G, Farina M, Vargiu N,<br />
Mallmann P, Dattena M, Capobianco G, Peters D et al. Vitrification <strong>of</strong><br />
human spermatozoa without cryoprotectants. Cryo Letters 2002;<br />
23:93–102.<br />
Nicopoullos JD, Gilling-Smith C, Almeida PA, N<strong>or</strong>man-Tayl<strong>or</strong> J, Grace I,<br />
Ramsay JW. Use <strong>of</strong> surgical sperm retrieval in azoospermic men: a<br />
meta-analysis. Fertil Steril 2004;82:691–701.<br />
Palermo G, J<strong>or</strong>is H, Devroey P, Van Steirteghem AC. Pregnancies after<br />
intracytoplasmic injection <strong>of</strong> single spermatozoon into an oocyte.<br />
Lancet 1992;340:17–18.<br />
Palermo GD, Schlegel PN, Hariprashad JJ, Ergun B, Mielnik A, Zaninovic N,<br />
Veeck LL, Rosenwaks Z. Fertilization and pregnancy outcome with<br />
intracytoplasmic sperm injection <strong>f<strong>or</strong></strong> azoospermic men. Hum Reprod<br />
1999;14:741–748.<br />
Prins GS, Dolgina R, Studney P, Kaplan B, Ross L, Niederberger C. Quality<br />
<strong>of</strong> cryopreserved testicular sperm in patients with obstructive and<br />
non-obstructive azoospermia. J Urol 1999;161:1504–1508.<br />
Quintans CJ, Donaldson MJ, Asprea I, Geller M, Rocha M, Pasqualini RS.<br />
Development <strong>of</strong> a novel approach <strong>f<strong>or</strong></strong> <strong>cryopreservation</strong> <strong>of</strong> very small<br />
numbers <strong>of</strong> spermatozoa. Hum Reprod 2000;15:99.<br />
Schlegel PN, Su LM. Physiological consequences <strong>of</strong> testicular sperm<br />
extraction. Hum Reprod 1997;12:1688–1692.<br />
Schlegel PN, Palermo GD, Goldstein M, Menendez S, Zaninovic N,<br />
Veeck LL, Rosenwaks Z. Testicular sperm extraction with<br />
intracytoplasmic sperm injection <strong>f<strong>or</strong></strong> nonobstructive azoospermia.<br />
Urology 1997;49:435–440.<br />
Schoysman R, Vanderzwalmen P, Nijs M, Segal L, Segal-Bertin G, Geerts L,<br />
van Roosendaal E, Schoysman D. Pregnancy after fertilisation with<br />
human testicular spermatozoa. Lancet 1993;342:1237.<br />
Schuster TG, Keller LM, Dunn RL, Ohl DA, Smith GD. Ultra-rapid freezing<br />
<strong>of</strong> very low numbers <strong>of</strong> sperm using cryoloops. Hum Reprod 2003;<br />
18:788–795.<br />
Sereni E, Bonu MA, Fava L, Sciajno R, Serrao L, Preti S, Distratis V,<br />
B<strong>or</strong>ini A. Freezing spermatozoa obtained by testicular fine needle<br />
aspiration: a new technique. Reprod Biomed Online 2008;16:89–95.<br />
Sohn JO, Jun SH, Park LS, Kim EK, Chung TG, Lee DR. Comparison <strong>of</strong><br />
recovery and viability <strong>of</strong> sperm in ICSI pipette after ultra rapid<br />
freezing <strong>or</strong> slow freezing. Fertil Steril 2003;80:S128.<br />
Spada<strong>f<strong>or</strong></strong>a C. Sperm cells and <strong>f<strong>or</strong></strong>eign DNA: a controversial relation.<br />
Bioessays 1998;20:955–964.<br />
Stroup DF, Berlin JA, M<strong>or</strong>ton SC, Olkin I, Williamson GD, Rennie D, Moher D,<br />
Becker BJ, Sipe TA, Thacker SB. Meta-analysis <strong>of</strong> observational<br />
studies in epidemiology: a proposal <strong>f<strong>or</strong></strong> rep<strong>or</strong>ting. Meta-analysis Of<br />
Observational Studies in Epidemiology (MOOSE) group. JAMA 2000;283:<br />
2008–2012.<br />
Suzuki N, Suzuki Y, Sato T, Matsubara H, Ikuta K, Suzum<strong>or</strong>i K.<br />
Cryopreservation <strong>of</strong> a few spermatozoa in hamster zonae pellucidae.<br />
Hum Reprod 1999;14:289.<br />
Wells GA, Shea A, O’Connell D, Peterson J, Welch J, Losos M et al. The<br />
Newcastle-Ottawa Scale (NOS) <strong>f<strong>or</strong></strong> Assessing the Quality <strong>of</strong> Nonrandomised<br />
Studies in Meta-Analyses (Homepage on the Internet). Ottawa Health<br />
Research Institute: Ottawa, c1996–2006. Available from: http://<br />
www.ohri.ca/programs/clinical_epidemiology/ox<strong>f<strong>or</strong></strong>d.htm [updated 9<br />
June 2007; cited 6 September 2007].<br />
Walmsley R, Cohen J, Ferrara-Congedo T, Reing A, Garrisi J. The<br />
first births and ongoing pregnancies associated with sperm<br />
<strong>cryopreservation</strong> within evacuated egg zonae. Hum Reprod 1998;<br />
13(Suppl. 4):61–70.<br />
Westlander G, Rosenlund B, Soderlund B, Wood M, Bergh C. Sperm<br />
retrieval, fertilization, and pregnancy outcome in repeated testicular<br />
sperm aspiration. J Assist Reprod Genet 2001;18:171–177.<br />
Submitted on January 18, 2008; resubmitted on November 4, 2008; accepted on<br />
December 2, 2008














